Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of integrase inhibitors wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmacognosy wikipedia , lookup
NMDA receptor wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Effects of long-term benzodiazepine use wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Prescription costs wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Toxicodynamics wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Theralizumab wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
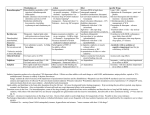
PREMEDICATION DRUGS DR.SUDHIR MUBARAK AL KABEER HOSPITAL PREMEDICATION- DEFINITION Premedication refers to the administration of drugs in the period 1 – 2 hours before induction of anaesthesia OBJECTIVES Allay anxiety and fear Reduce secretions Enhance the hypnotic effects of G.A agents Reduce P.O.N.V Prodcuce amnesia Prevent aspiration Attenuate vagal reflexes Attenuate sympathoadrenal response ALLAY ANXIETY & FEAR The best way to do this is by non –pharmacological means Psychotherapy – Reassurance Benzodiazepines- most commonly used drugs BENZODIAZEPINES Anxiolytic Amnesic Hypnotic Sedative Most commonly used premedication drug Mechanism of action- Site Modification of emotional response & behaviour – by suppressing the neuronal activity between limbic system and hypothalamus Decrease in alertness and arousal- by depressing interaction between limbic system and the RAS Anticonvulsant effect – inhibition of amygdaloid nuclei Muscle relaxant – suppression of polysynaptic reflexes in spinal cord ( central acting relaxant) Mechanism of action- Mode GABA – mediated inhibitory effects GABAA RECEPTORS Cortex & Limbic system GABAB – brain stem & spinalcord – Baclofen GABAA RECEPTORS – they are mebrane protein pentameric structure associated with chloride channel Three sububits – ά ,β, γ GABA binding site Chloride channel Benzodiazepine binding site GABA binding site Chloride channel Benzodiazepine binding site Benzodiazepines enhance the efects of GABA on GABA receptor Thus they increase the frequency of chloride channel opening Channel opening times are unchanged ( contatrast to barbiturates) Increased chloride ions cause neuronal hyper polarisation and thus inhibition Stage 3 sleep is increased Stage 4 sleep and REM sleep decreased Classification Long acting – diazepam Medium acting – temazepam Short acting - midazolam DRUG Half life Active Half lifes Terminal Metabol metaboli tes -ites (hrs) Dose (mg) Potency FLUNITRAZEPAM 1 30 12-20 Y TEMAZEPAM 20 1.5 4-10 Y MIDAZOLAM 10 3 1-3 N ALPROZALAM 0.5 60 10-12 Y CHLORDIAZEPOXIDE 20 1.5 5-30 Y CLONAZEPAM 6 5 20-60 N DIAZEPAM 10 3 24-48 Y LORAZEPAM 1 30 10-20 N OXAZEPAM 30 1 6-25 N 25-30 50-120 Diazepam Most commonly used Insoulble in water so formulated in propylene glycol, which is very irritant to veins. Diazemulus – lipid emulsion Bioavailability 100% Protein binding 90-95%. Dosage Premedication 10-15 mg oral 1- 1.5 hrs preop Sedation- 7-15 mg i.v slowly, increments 1-2 mg Status epilepticus- 2mg every minute , max 20 mg Intensive care- not for infusion – 5-10mg 4th hourly 50 – 120 hrs 4-10 hrs 6-25 hrs Midazolam Imidazo – benzodiazepine derivative It is this imidazole ring which imparts water solubility at pH < 4 At blood pH, drug becomes lipid soluble due to ring closure and penetrates brain rapidly in 90 seconds – peak effect 2- 5 mins Bioavailability – 44% Hepatic elimination( liver blood flow) Hydroxy-midazolam- active metabolite – 1 hrclinically important only after prolonged infusion in renal failure Midazoalm is 1.5 -2 times more potent than diazepam ( ? ) Dosage: Premedication: 15mg oral or 5mg I.M,nasal drops Sedation: 2-7mg I.V incre 0.5 – 1 mg Status epilepticus : not recommended ( ? ) Intensive care 0.03 -0.2 mg/kg/hr Ring open Ring closed LORAZEPAM Longer duration(10-20 hrs) DOC – liver failure CLONZEPAM Can be used in status epilepticus Seizure adjuvant FLUMAZENIL Competetive antagonist, reverses all effects Has slight intrinsic agonist property – so can precipitate seizures ( INVERSE AGONISM ) Short half life – 1 hr, may need repeated injections or infusion 0.2 mg ,then 0.1 mg increments ( don’t exceed 3 mg) PHENOTHIAZINES They produce the following effects Central antiemetic action Sedation Anxiolysis H2 receptor antagonism ά – adrenergic anatagonism Anticholenergic properties Potentiation of opiod analgesia Side effects : extrapyramidal effects Promethazine & trimeprazine ( children) ANTIMUSCURANIC DRUGS Used for there : Antisialogue action Avoid bradycardia due to anaesthetic agents surgical stimulus( occulocardiac reflex, mesenteric traction) Β blocked or digitalised patients Intermittent suxamethonium Avoid reflex bronchospasm ( COPD) Children ( vagal predominance) Disadvantages : Dry mouth ,palpitations, arrthymias, blurred vision Central anticholergic syndrome ATROPINE HYOSCINE Dose 0.6mg 0.4mg potency 1 2 Duration 1-1.5hrs 1-1.5hrs CNS Yes -excitatory Yes- depression Central anticholenergic syndrome Tachycardia Motion sickness,vestibular disorders More less (initial bradycardia- partail agonist- M2 receptors Antisialogue less more Bronchodilatation More less Physiological dead space more less Mydriasis Less More(cycloplegia) GYCOPYRROLATE Synthetic antimuscuranic drug Ionised quaternary amine –so doesnot cross BBB & placenta Prolonged duration of action- 6hrs No or Less tachycardia Ideal for cardiac patients ( IHD) Pupillary and other changes minimal Antisialagogue action more Dose 0.1 – 0.4 mg α2 RECEPTOR AGONISTS Action : they decrease noradrenaline release in both central and peripheral symp. N. CNS : tractus solitarius – hypotension & bradycardia Locus coerulus – sedation Vagal nuclei Spinal & supraspinal level(non opioid) - Analgesia Peripheral : Decrease cardiac rate Decrease smooth muscle tone Increase coronary blood flow Induce diuresis Platelet aggregation Anaesthesia - α2 agonists Decrese MAC requirements Attenuate sympathoadrenal responses associated with intubation and surgery CLONIDINE( 100-300 mics orally) DEXMEDETOMEDINE AZEPEXOLE Side effects : dry mouth, sedation,depression, bradycardia, rebound hypertension Other drugs NSAIDS Diclofenac Ketorolac TAM mixture – children ( trimeprazine,atropine,mefenamic acid) ANTIEMETICS ANTACIDS NEXT CALSSES 8. Atropine: a) may cause bradycardia b) dilates the pupil in premedicant dose c) has a shorter duration of action than glycopyrrolate d) increases the physiological dead space e) has both muscarinic and nicotinic effects TTTTF Flumazenil: a) may induce panic attacks in susceptible patients b) has anticonvulsant activity in patients with epilepsy c) has a long duration of action d) may cause nausea and vomiting e) has inverse agonist action at benzodiazepine receptors TFFTT Glycopyrrolate: a) can act at central cholinergic receptors b) can increase the physiological dead space c) can dilate the pupil d) is equally effective when given orally e) is five times more potent as an antisialagogue than atropine FTTFT c) hence use with caution in glaucoma. Midazolam: a) is an anticonvulsant b) is lipid soluble at physiological pH c) has no active metabolites d) has an elimination half-life of 2-4 hours e) can be administered as nasal drops for premedication TTFTT Hyoscine: a) causes tachycardia b) causes sedation c) causes mydriasis d) is an antiemetic e) has a weaker antisialagogue effect than atropine TTTTF Hyoscine hydrobromide causes: a) antiemesis b) somnolence c) pupillary dilatation d) tachycardia followed by bradycardia e) extrapyramidal symptoms TTTTF Chlorpromazine: a) can cause dystonic reactions b) antagonises apomorphine-induced vomiting c) is a dopamine antagonist at the chemoreceptor trigger zone d) is a weak alpha-adrenergic agonist e) undergoes extensive first-pass metabolism TTTFT Clonidine: a) is an alpha-2 receptor agonist b) is a dopamine antagonist c) causes tachycardia d) inhibits salivation e) reduces the minimum alveolar concentration of halothane TFFTT