Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug interaction wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Pharmacognosy wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Polysubstance dependence wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Toxicodynamics wikipedia , lookup
NMDA receptor wikipedia , lookup
Norepinephrine wikipedia , lookup
Neuropharmacology wikipedia , lookup
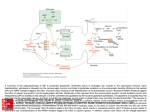
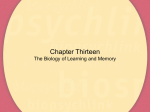
Aniracetam: A Comprehensive Yet Easy Reading Review Dr. Michael P. Ludwig 1-[(4-methoxybenzoyl)]-2-pyrrolidinone Aniracetam Disclaimer: Nothing presented in this article is to be construed as constituting **** medical advice or pharmaceutical consultation. This article is intended purely **** as general knowledge and entertainment ABSTRACT As the purpose of this review article is to provide a general background and hopefully generate interest in aniracetam and other nootropics, many topics will be touched upon. Positive allosteric AMPA receptor modulation and long-term potentiation will be discussed as possible mechanisms of memory enhancement. The hippocampus being a major memory center will be touched upon. Studies, both human and animal, delving into aniracetam's effects on visual enhancement, anxiolysis, anti-depression in the elderly, increased tolerance to alcohol and lastly aniracetam's effects on sleep deprevation will be covered and analyzed. A description of physical properties of the compound and its dosing will be covered before finishing with this author's conclusion regarding aniracetam. INTRODUCTION When presented with the opportunity to possibly increase one's memory and general cognition, reduce anxiety without the common side effect of sedation, enhance one's vision, and reduce the symptoms of depression all from one supplement with a proven safety record, would one make the decision to take such a supplement? The purpose of this article is to provide the reader with enough information to make that decision. The focus of this article is on the supplement aniracetam, although there will also be some basic background information concerning the racetam class of drugs, as well as some background and definition on the word “nootropic”itself. When one thinks of racetams, well those who do think of racetams, they usually think first of piracetam. This is expected, as it is the prototypical racetam; it is the drug that defined the class. Since piracetam was first synthesized in 1964 by Dr. Corneliu Giurgea⁽²⁷⁾, the class has since grown to include more than 25 unique compounds. Only one, levetiracetam, is approved by the FDA for human use in the United States⁽²⁾, however several other members of the class have been approved in Europe and Russia for human use for many years. Over those years they have built a reputation of safety and efficacy in the individuals for which they are approved. One such drug, that is available by prescription overseas, but is sold as a supplement in the United States, is aniracetam. Aniracetam is commonly quoted around the internet as being first synthesized in the 1970's shortly after piracetam, however the earliest issued patent for the synthesis of the compound dates to July 14th 1982, however it claims priority to an earlier patent application dating to February 10th 1978⁽²⁾. The compound was invented by Emilio Kyburz and Werner Aschwanden, and owned via assignment by Hoffmann-La Roche. This first patent for aniracetam was a European patent, however the Patent Cooperation Treaty would have extended its protection to the United States. The first aniracetam patent filed in the United States was issued on January 18th 1983⁽³⁾. It was also invented by Emilio Kyburz and Werner Aschwanden, and owned via assignment by Hoffmann-La Roche. Since then, 183 various utility patents have been issued for aniracetam⁽²⁴⁾. In Europe and Russia, aniracetam is usually sold under the brand name Ampamet™, but may also be sold under the brand names Draganon™, Sarpul™, and Memodrin™⁽²³⁾. In the United States, aniracetam is not currently sold under any official brand names as it is not FDA approved. It is usually sold as a supplement marked simply as generic aniracetam. Some nootropic vendors will assign a pseudo brand name to their aniracetam such as “Neuro Wave” though this is not an official brand name. Why would one want to take aniracetam? That is a good question. Aniracetam exhibits a multitude of positive, efficacious effects, with little to no adverse reactions or side effects. These attributes are what classifies aniracetam as a nootropic drug. Miriam-Webster dictionary defines nootropic as a substance that enhances cognition and enhances memory and facilitates learning⁽¹⁵⁾. However, Dr Corneliu Giurgea, who originally defined the word nootropic, stated that among a few other requirements the drugs must exhibit few side effects and low toxicity⁽⁷⁾. Giurgea's definition is still the generally accepted definition of the word nootropic as his added requirements are what separate nootropics from general cognitive enhancers. Aniracetam fits all the requirements of Giurgea's definition and is thus a true nootropic. MECHANISM OF ACTION Before getting into the actual effects of aniracetam, it will be beneficial to first provide an understanding of what the drug actually does in the brain that ultimately results in its various effects. This is referred to as the drug's mechanism of action, commonly abbreviated to MOA. Aniracetam does not exert its effects on its own. When taken orally, aniracetam is rapidly broken down through the process of first pass metabolism. Roughly 10% of the aniracetam dose survives this process; the rest is metabolized into various metabolites. Of these metabolites, 2-pyyrolidinone and N-anisoyl-GABA are two active metabolites that will be focused on here. Aniracetam and its active metabolites have a multitude of effects on various receptors in the brain which will be briefly touched upon, however due to the scope of this article, positive modulation of AMPA receptors will be the the primary focus. This MOA will be focused upon, because it is an interesting, relatively well understood mechanism that many drugs exhibit to a certain degree; among the drugs exhibiting this MOA are aniracetam itself and the active metabolite 2-pyyrolidinone⁽²⁹⁾. Getting into positive modulation of AMPA receptors, the brain heavily utilizes two main chemicals to result in either inhibition or excitation in various, and selective sites. The main inhibitory chemical is GABA while the main excitatory chemical is glutamate. Glutamate acts on three subsets of ionotropic receptors: NMDA, Kainate, and AMPA. Aniracetam and 2-pyyrolidinone act on the AMPA glutamate receptor, but do not directly activate it. This is where the term “positive modulation” comes in. When glutamate binds to an AMPA receptor in the presence of aniracetam or 2-pyyrolidinone, the AMPA receptor remains sensitized for a longer period than had glutamate bound to the receptor alone without the presence of aniracetam or 2-pyyrolidinone. This MOA allows for a controlled increase in the excitation caused by glutamate⁽⁹⁾. Drugs that bind directly to glutamate receptors and activate them all on their own are referred to as “direct agonists.” Glutamate agonists, especially ones that bind to NMDA receptors, can result in a toxic condition known as excitotoxicity⁽¹⁴⁾. This is generally not seen with positive AMPA receptor modulators due to the more controlled increase in glutamanergic excitation as well as a special function of one of the AMPA receptor's subunits, GluR2, which intrinsically protects against exitotoxity. The other well known active metabolite of aniracetam, N-anisoyl-GABA, exerts its effect on the metabotropic glutamate receptor 2, mGluR2, which is usually found presynaptically⁽³⁰⁾. Being presynaptic means it tends to act in a negative feedback role. It realizes when there is enough glutamate floating around and say "Hey guys that's enough." This results in a decrease of glutamanergic activity. This helps prevent exitotoxicity and may be where the anxiolytic effects of aniracetam arise from. N-anisoyl-GABA also indirectly increases levels of dopamine and serotonin in the prefrontal cortex. It seems to do this via interaction with nicotinic acetylcholine, nACh, receptors. When N-anisoly-GABA acts on nACh receptors in the Ventral Tegmental Area, a specific brain area heavily associated with dopamine, dopamine levels in the prefrontal cortex increase. When N-anisoyl-GABA acts on nACh receptors in the Dorsal Raphe Nucleus, a specific brain area associated with serotonin, serotonin levels in the prefrontal cortex increase⁽³¹⁾. Even with all the mechanisms discussed above, there are still more that are beyond the scope of this article, and there are probably other mechanisms not yet discovered. Though this author focused on positive AMPA modulation, the effects of aniracetam are likely a result of many combined mechanisms with no single, clear MOA. MEMORY ENHANCEMENT Like most popular racetams, aniracetam is usually recognized for its memory enhancing effects. Elderly patients experiencing dementia have been shown to respond better to treatment with aniracetam than to treatment with acetylcholinesterase inhibitors which are currently the gold standard for treatment of dementia and Alzheimer’s disease⁽⁴⁾. Studies have shown aniracetam to increase working memory and spacial awareness in mice exhibiting preexisting cognitive deficit either through the administering of drugs known to cause cognitive decline, or through selective, biotechnological breeding⁽⁵⁾. There is no doubt that aniracetam exhibits positive memory enhancing effects in both animal models and human models with preexisting cognitive deficit. The question now is, does it produce the same effects on healthy subjects? If aniracetam has the ability to bring cognitively impaired subjects either back to or close to baseline, then one might logically infer that an average, non cognitively impaired subject could possibly be brought above baseline, and thus experience a cognitive enhancing nootropic experience. To this day, no trials have been able to show conclusively whether aniracetam has the ability to increase memory and spacial awareness in subjects not experiencing preexisting cognitive deficit. This may sound disappointing, but it is not necessarily the case. Despite the lack of clinical research data supporting the use of aniracetam as a memory enhancer in healthy individuals, there are countless anecdotal reports across nootropic forums of individuals taking aniracetam as a supplement and self reporting noticeable increases in working memory and recall. A common theme among these anecdotal reports is the ability to recall memories long since forgotten. While a good portion of this could be attributed to the placebo effect, this author believes that aniracetam does produce increased memory recall in healthy individuals. The trials that failed to show efficacy in healthy individuals all looked at working memory, not recall. Between the anecdotal reports and the drug's established safety record, aniracetam can still be considered a viable nootropic. So how exactly does aniracetam's positive modulation of AMPA receptors effect memory? To understand this, we first have to understand the concept of long-term potentiation. When neurons talk to one another, they do so with different intensities. Some are able to whisper and get their point across while other have to yell and still might not be heard. The process of two neurons gaining the ability to communicate more efficiently, so that they can whisper as opposed to yell happens through the process of long-term potentiation. Over time, long-term potentiation leads to the strengthening of neuronal circuits which is believed to be the mechanism of memory creation. Long-term potentiation happens in various parts of the brain, but the part of the brain that is usually focused upon in terms of memories is the hippocampus⁽⁴⁾⁽¹³⁾⁽⁸⁾ . Long-term potentiation itself is thought to be influenced mostly by glutamate acting on NMDA receptors, so what does this have to do with aniracetam whose effects are on AMPA receptors and not NMDA receptors? Long-term potentiation of NMDA receptors is thought to causes a downstream potentiation or strengthening of AMPA receptors. When aniracetam positively modulates AMPA receptors in the hippocampus, and possibly other parts of the brain its effect seem to mimic that of long-term potentiation, and thus enhancement of memory⁽⁸⁾. See Figure (A) below for a better understanding of the hippocampus and were it exists in respect to the rest the brain. Figure (A) The Exposed Brain. (see citation in the lower right corner of illustration) The hippocampus, highlighted in purple, normally sits under the temporal lobe of the cerebral cortex. For the sake of clarity, the left temporal lobe has be left out of this illustration, so as to provide easy viewing of the hippocampus. The hippocampus is composed of two individual hippocampi, one located in each hemisphere of the brain. Fairly small and vaguely resembling the shape of a seahorse, the hippocampus is thought to play an important role in memory consolidation. Aniracetam's enhancement of long-term potentiation in the hippocampus may play a major role in its memory enhancing effects. VISUAL ENHANCEMENT Aniracetam possesses many positive effects other than memory enhancement. Many users report a brightening of colors which some describe as intense. There are many drugs that can cause brightening of colors, however they are also usually accompanied by psychedelic effects. Aniracetam has the ability to drastically increase color brightness and saturation without any psychedelic effects. Studies show that aniracetam's positive modulation of retinal AMPA receptors is the likely cause of the effect⁽¹⁶⁾. Retinal AMPA receptors seem to play a part in a phenomenon know as Retinal Spreading Depression. The purpose of Retinal Spreading Depression is thought to control the circadian rhythm through either release or suppression of melatonin⁽¹º⁾. Two studies conflicted over whether aniracetam's positive modulation of the retinal AMPA receptor lead to a Retinal Spreading Depression⁽¹⁰⁾⁽¹⁶⁾. Either way, aniracetam's positive modulatory effect on retinal AMPA receptors does lead to an increase in brightness, saturation, and intensity of color. Having the world appear brighter and thus more interesting could be a possible treatment modality, either as mono-therapy, or add-on therapy for patients experiencing depression and/or anhedonia. This writer personally experienced, after taking aniracetam, the ability to look up at the sky and for the first time appreciate how beautiful the clouds are. This was no placebo effect, as this writer was not aware of aniracetam's effects on retinal AMPA receptors at the time. ANTI-ANXIETY EFFECTS Another possible benefit of aniracetam is anxiolysis, or the quelling of anxiety. It has been known since the early 1990's that aniracetam provides anxiolysis in patients suffering from cerebrovascular disorders such as post-stroke⁽²²⁾. It wasn't until 2001 that a study proved that aniracetam was efficacious in relieving anxiety in healthy mice⁽¹⁹⁾. The study utilized various antagonists, chemicals that block aniracetam's effects at specific receptors, to determine the MOA of aniracetam's anxiolytic properties. Unlike aniracetam's effects on memory and sight, the study determined that the anxiolytic properties were not due to positive AMPA modulation. The study introduced three antagonists: haloperidol which acts to block aniracetam's effects on dopamine D2 receptors, mecamylamine which acts to block aniracetam's effects on nicotinic acetylcholine receptors, and ketanserin which acts to block aniracetam's effects on serotonin 5-HT2a receptors. All three antagonists blocked the anxiolytic effect of aniracetam. Mecamylamine and ketanserin blocked the anxiolytic effect strongly, though not completely. Haloperidol blocked the anxiolytic effects completely. These results suggest that the MOA of aniracetam's anxiolytic effect is mediated via its interaction with dopamine, acetylcholine, and serotonin, with interaction with dopamine being the main mechanism, though the total anxiolytic effect is most likely a result of a synergistic effect on all three systems. To this day there are no clinical studies proving anxiolytic effects in humans, though many people who have taken aniracetam have reported experiencing a non-drowsy anxiolysis. ANTIDEPRESSANT EFFECTS Users have anecdotally reported antidepressant effects after taking aniracetam. The antidepressant effect of aniracetam has been clinically proven in an animal model⁽²⁰⁾. A study in 2001 has shown statistically significant antidepressant effects in aged rats, though the study failed to show antidepressant effects in young rats. The authors attributed the antidepressant effects in aged rats to aniracetam's enhancement of cholinergic and dopaminergic nerurotransmission. The authors also suggested that the antidepressant effect was not due to aniracetam alone, but also to two of its active metabolites, N-anisoyl-GABA and 2-pyrrolidinone. The results of the study suggest that aniracetam could be a viable treatment option for treating depression in the elderly. EFFECTS ON SLEEP DEPRIVATION There are times when one may be forced to function on little or no sleep. Those that have experienced sleep deprivation can attest , that the longer they go without sleep, the more their cognitive abilities suffer. There are most likely a number of neurotransmitter and neuromodulator systems taking part in this effect, but for now, to keep things on topic, let us examine the effects of glutamate and AMPA receptors on sleep deprivation. It Is believed, during periods of sleep deprivation, AMPA receptors become less sensitive to glutamate⁽⁶⁾. A study that put rats through 96 hour periods of sleep deprivation, had them complete complex tests and then ultimately removed their brains to perform a more intimate experiment, noticed a significant decrease of glutamate binding to AMPA receptors. This was noticed in a few parts of the brain, but most noticeably in the hippocampus. Rats in the group that had been pre-treated with 100mg/kg of aniracetam did not receive the cognitive disabilities experienced by rats in the in the groups that received 50mg/kg or 25mg/kg or aniracetam, nor did they experience the cognitive disabilities seen in rats in the control group as well as rats in the group that received the negative allosteric AMPA modulator GYKI 52466⁽⁶⁾. The results of this study indicate that decreased binding of glutamate to AMPA receptors in the hippocampus is a possible mechanism for the cognitive decline experienced after sleep deprivation. It is interesting to point out though that the dose of aniracetam necessary to prevent sleep deprivation induced cognitive decline in incredibly high. Considering the average person weighs roughly in the range of 70-80kg, one would be looking at an aniracetam dose in the range of 7000mg-8000mg which is way above the recommended daily dose. One would have to keep in mind, though, that due to differences in the way that rats and humans metabolize drugs, the doses wouldn't actually be that high, but they would definitely be higher than normal recommended doses. Let us just say it would be a dose this author would not feel comfortable recommending. Despite aniracetam's safety record, there are times when one must pull in the reins and error on the side of precaution. ANIRACETAM'S EFFECTS ON ALCOHOL TOLERANCE May users of aniracetam have, for a long time, noted a self reported increase in alcohol tolerance while taking aniracetam. Basically, they could drink much more before achieving intoxication. At this point, one might take this as nothing more than some anecdotal reports used as an excuse to drink more, but in 2009 a study was done that determined that pretreatment with aniracetam at either 10mg/kg, 15mg/kg, or 22.5mg/kg resulted in rats developing a rapid tolerance to ethanol⁽²⁶⁾. It is currently unknown why this happens, but one can suggest perhaps tolerance to ethanol is, at least partially, a learned process. If learning involves long-term potentiation, then one can draw the logical conclusion that aniracetam may may increase the rate and sensitivity at which long-term potentiation creates the neuronal circuits responsible for the learned process of ethanol tolerance. As a precaution, this writer highly recommends not taking a large dose of aniracetam for the purpose of going out to drink. One may not feel as drunk, but they still may be causing neuronal damage, as well as possible liver damage, and most likely setting themselves up for a bad hangover. PHYSICAL PROPERTIES AND DOSING Aniracetam differs from piracetam not only in its subjective effects, but also in its physical properties. While piracetam is water soluble, aniracetam is fat soluble⁽¹²⁾. Taking aniracetam along with a source of fat may help its absorption. If the reader also takes fish oil capsules, they may want to take them together. A larger implication of aniracetam's fat solubility, or lipophilicity, is that it is able to conveniently cross the blood brain barrier allowing more of the drug to reach the brain. This is a possible reason for aniracetam's increased potency compared to piracetam. The average dose of aniracetam as a supplement is 750mg twice daily⁽¹⁾; for comparison, the average dose of piracetam is 800mg three times daily or 1200mg twice daily⁽²⁾, though many individuals take doses much higher. The manufacture of Ampamet™ recommends that patients with kidney failure (creatinine clearance <10 mL/min) cut the daily dose in half⁽¹⁾. This author tends to be more conservative and would recommend patients with kidney failure not take aniracetam. The half-life of aniracetam, the time it takes the body to get rid of half the dose, is 35 minutes⁽¹²⁾. Normally with a half-life this short, dosing more than twice daily is required, though aniracetam seems to have active metabolites, 2-pyrrolidinone, p-anisic acid and N-anisoyl-GABA, that provide continued effects after the parent drug has already been eliminated⁽¹²⁾. POSSIBLE SIDE EFFECTS Giurgea's original definition of the word “nootropic” specified that the drug must exhibit few side effects and low toxicity. Aniracetam fits Giurgea's definition as it does exhibit few side effects. Some users anecdotally report a mild headache that goes away with choline supplementation. For subjects who do experience headache, 500mg of choline a day seems to be sufficient for prevention. The choline can either be sourced through supplementation or diet; eating a few eggs every morning is a good way to get a head start on staying on top of one's daily choline requirement. Some users report agitation, anxiety, restlessness, and insomnia⁽¹⁾. Taking one 1500mg dose in the morning as opposed to two 750mg doses throughout the day may help prevent this⁽¹⁾. Though no studies have ever shown aniracetam to be teratogenic, it is still advised to avoid use during pregnancy and breast feeding⁽¹⁾. NON-RESPONDERS There exists a minority of aniracetam users who report no beneficial effects. These users are typically referred to as non-responders. When one attempts to come up with a possible reason why some individuals respond positively while others do not, they may be left baffled. With so many possible variables, it seems the simplest answer is that “everybody is different.” It is true that everybody is different, but to satisfy the curiosity as to what exactly results in whether an individual is a responder or a non-responder involves looking a little deeper. While there are most likely a variety of differences in play, there have been two studies that point to two specific differences that may determine whether an individual is a responder or a non-responder. In 1992, a study revealed that elevated levels of the steroid cortisol blocked the memory enhancing effects of aniracetam⁽¹⁸⁾. This is an important consideration. There are many reasons why a person may have an elevated cortisol level. High levels of stress, chronic inflammation, Cushing's syndrome, certain medications, are all among the many reasons a person may experience elevated cortisol level and thus be more likely to be a non-responder. In 1990, another study revealed that low levels of the steroid aldosterone blocked the memory enhancing effects of aniracetam⁽¹⁷⁾. Certain drugs that act on the kidneys such as ACE inhibitors which are used to lower blood pressure, NSAIDS which are used to relieve pain and swelling, and diuretics which are usually used to control blood pressure, all have the ability to lower aldosterone levels. Patients with Addison's disease have markedly low levels of aldosterone. One can see that between the many ways that either cortisol can be elevated and aldosterone can be lowered, there exists a possible explanation as to why certain individuals are non-responders. CONCLUSION This author feels that aniracetam is a safe and effective supplement that offers many benefits. The reader has to take the information presented, process it, possibly conduct some of their own additional research, and ultimately come to a decision on whether they think aniracetam is right for them. Aniracetam is just one of many available nootropics. This author would advise the reader to view as many articles as possible, decide what is right for them, and consult their physician as well as their pharmacist to make sure there are no drug interactions. Aniracetam, nor any other nootropic will make a person “Limitless” but they just might find their quality of life increased even if only subtly. Author Available for Correspondence Dr. Ludwig would be happy to answer any question one may have. Please, do not hesitate to contact Dr. Ludwig. He can be reached at [email protected] Thank you for reading. Works Cited 1. Ampamet Package Insert 2. Aschwanden W, Kyburz E (7/14/82). European PCT Patent #EP300051143 worldwide.espacenet.com/publicationDetails/biblio?CC=EP&FT=D&NR=0005143B1&KC=B1 3. Aschwanden W, Kyburz E (1/18/83). USPTO Patent #4369139 http://patft.uspto.gov/netacgi/nph-Parser?d=PALL&p=1&u=%2Fnethatml%2FPTO %2Fsrchnum.htm&r=1&f=G&l=50&s1=4369139.PN.&OS=PN/4369139&RS=PN/4369139 4. Bliss T, Collingridge G (January 1993). “A synaptic model of memory: long-term potentiation in the hippocampus”. Nature 361(6407): 31-39 5. Cumin R, Bandle E, Gamzu E, Haefely W (1982). “Effects of the novel compound aniracetam(Ro13-5057) upon impaired learning and memory in rodents”. Psychopharmacology 78(2): 104-111 6. Dubliea F, Queiriz C, Moreira K, Nobrega J, Sita L, Tufik S, Hipolide D (Sep 2013). “AMPA receptors mediated passive avoidance deficits induced by sleep deprivation”. Behavioral Brain Research (257): 189-196 7. Giurgea C, Greindl M, Preat S (1983). “Nootropic drugs and aging”. Acta Pshychiatr Belg 83(4): 349- 358 8. Ito I, Tanabe S, Khoda A, Sugiyama H (1990). “Allosteric potentiation of quisqualate receptors by a nootropic drug aniracetam”. Journal of Physiology (424): 533-543 9. Jin R, Clark S, Weeks A, Dudman J, Gouaux E, Partin K (1/28/2005). “Mechanism of positive allosteric modulators acting on AMPA receptors”. The Journal of Neuroscience 25(39): 9027- 9036 10. Kertesz S, Kapus G, Levay G (Oct 2004). “Interactions of allosteric modulators at AMPA/kianate receptors on spreading depression in the chicken brain”. Brain Research 1025(1-2): 123-9 11. Koliaki C, Messini C, Tsolaki M (January 2011). “Clinical efficacy of aniracetam, either as monotherapy or combined with cholinesterase inhibitors, in patients with cognitive impairment: a comparative open study”. CNS Neurosciences and Therapeutics 18(2012): 302-312 12. Lee C, Benfield P (1994). “Aniracetam: an overview an overview of its pharmacodynamic and pharmacokinetic properties, and a review of its therapeutic potential in senile cognitive disorders”. Drugs & Aging 4(3): 257-273 13. Lomo T (2003). “The discovery of long-term potentiation”. Philos R Soc Lond Biol Sci 358(1432): 617-20 14. Manev H, Favaron M, Guidotti A, Costa E (July 1989). “Delayed increase of calcium influx elicited by glutamate: role in neuronal death”. Molecular Pharmacology 36(1): 106-112 15. Mirriam-webster.com/dictionary/nootropic 16. Moldavan MG, Allen CN (May 2001). “Retinohypthalmic tract synapses in the rat superchiasmic nucleus demonstrate short-term synaptic plasticity”. Journal of Neurophysiology (103)5: 2390- 2399 17. Mondadori C, Bhatnagar A, Borkowski J, Hausler A (1990). “Involvement of a steroidal component in the mechanism of action of piracetam-like nootropics”. Brain Research 506(1): 101-108 18. Mondadori C, Ducret T, Hausler A (1992). “Elevated corticosteroid levels block the memoryimproving effects of nootropics and cholinomimetics”. Psychopharmacology 108(1-2): 11-15 19. Nakamura K, Kurasawa M (May 2001). “Anxiolytic effects of aniracetam in three different mouse models of anxiety and the underlying mechanism”. European Journal of Pharmacology 420(1):33-43 20. Nakamura K, Tanaka Y (April 2001). “Antidepressant-like effects in aged rats and its mode of action”. Psychopharmacology (158): 205-212 21. Nootropil Package Insert 22. Otomo E, Harai S, Terashi A, Hasegawa K, Tazaki Y, Araki G, Itoh E, Nishimura T, Furukawa T (1991). “Clinical usefullness of aniracetam for psychiatric symptoms in patients with cerebrovascular disorders: placebo controlled double blind trial”. J.Clin. Exp. Med. (156): 143-187 23. pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=2196 24. pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=2196#x393 25. pubchem.ncbi.nlm.nih.gov/summary/summary.cgi?cid=5284583 26. Rial D, Takashi R, Morato G (2009). “Aniracetam and DNQX affect the acquisition of rapid tolerance to ethanol in mice”. Pharmacology, Biochemistry and Behavior (92): 32-38 27. Shorvon S (2004). “Piracetam”. In Shorvon S, Fish D, Perucca E, Dodson W. “The treatment of epilepsy”. Wiley-Blackwell 489-495 28. Wang Y, Li C, Cai J (September 2006). “Aniracetam attenuates H2O2-induced deficiency of neuron viability, mitochondrial potential and hippocampal long-term potentiation of mice in vitro”. Neuroscience Bulletin 22(5): 274-280 29. Nishizaki T, & Matsumura T. (2002). The aniracetam metabolite 2-pyrrolidinone induces a longterm enhancement in AMPA receptor responses via a CaMKII pathway. Brain Research. Molecular Brain Research. 98(1-2), 130-4. 30. Shirane M, & Nakamura K. (2000). Group II metabotropic glutamate receptors are a common target of N-anisoyl-GABA and 1S,3R-ACPD in enhancing ACh release in the prefrontal cortex of freely moving SHRSP. Neuropharmacology. 39(5), 866-72. 31. Shirane M, & Nakamura K. (2001). Aniracetam enhances cortical dopamine and serotonin release via cholinergic and glutamatergic mechanisms in SHRSP. Brain Research. 916(1-2), 211-21. \