Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Clinical neurochemistry wikipedia , lookup
Proprioception wikipedia , lookup
Synaptic gating wikipedia , lookup
Development of the nervous system wikipedia , lookup
Central pattern generator wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Evoked potential wikipedia , lookup
Neural correlates of consciousness wikipedia , lookup
Neuroregeneration wikipedia , lookup
Hypothalamus wikipedia , lookup
Synaptogenesis wikipedia , lookup
Microneurography wikipedia , lookup
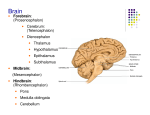
BRAINSTEM BRAINSTEM In general, the brainstem is made up of a mixture of long fiber pathways, wellorganized nuclei, and a network of cells which forms the brainstem reticular formation. Most of the nuclei are related directly either to cranial nerve functions or to motor control pathways. 10 of 12 cranial nerves enter and leave through the brainstem. Brainstem Components Medulla Pons Midbrain Medulla Ascending Tracts Medial lemniscus Spinothalamic tract Spinoreticular tract Spinocerebellar tract Cuneocerebellar tract Medulla Descending Tracts Corticospinal Spinal tract V Medial longitudinal fasciculus Tectospinal Rubrospinal Medulla Components Cranial nerve nuclei: VIII – XII Inferior cerebellar peduncle Medullary Pyramids (Anterior) Location of lateral corticospinal tracts. 85 percent of fibers decussate in the pyramidal decussation at the inferior border of the medulla. Fibers then enter lateral columns of spinal cord. These tracts help with initiating and modulating movement. Brainstem: Ventral Medullary Olives (Anterior) Inferior olivary nuclei receive input from most motor areas of the brain and spinal cord. Axons project to the contralateral cerebellar hemisphere via the olivocerebellar tract. These axons signal the cerebellum when a movement deviates from the planned movement. Medullary Olives (Anterior) Inferior olivary nuclei: Balance Coordination Sound impulse modulation Brainstem: Ventral Medulla Sends many fibers to the cerebellum via the inferior cerebellar peduncles: Spinocerebellar Olivocerebellar Vestibulocerebellar Reticulocerebellar Cerebellovestibular tract: Sends information from cerebellum to medulla Medullary Nuclei Cranial nerve nuclei: VIII, IX, X, XI, XII Vestibular nuclear complex Medullary Vital Reflex Centers Cardiac center: Inhibitory via CN X. Excitatory via T1-T5. Medullary rhythmicity center. Vasomotor center. Coordination of head movement and swallowing. Nonvital Reflex Centers Swallowing Vomiting Coughing Sneezing Hiccupping Dorsal Medullary Nuclei Nucleus cuneatus: Point of synapse for ascending fibers of the fasciculus cuneatus. Nucleus gracilis: Point of synapse for ascending fibers of the fasciculus gracilis. Portions of reticular formation: Associated with consciousness and arousal. Brainstem: Dorsal Medullary Roof Cranial portion = superior medullary velum. Caudal portion = inferior medullary velum. Very thin. Foramen (aperture) of Magendie. Posterior choroid plexus. Lateral Medullary Syndrome Wallenberg’s syndrome effects: Spinothalamic tract Spinal trigeminal tract and nucleus Fibers and nuclei of the glossopharyngeal nerve, vagus nerve, and part of the reticular formation. Portions of the vestibular nuclei and/or Portions of the inferior cerebellar peduncle. Lateral Medullary Syndrome Results in: Loss of pain and temperature on the contralateral side (spinothalamic tract) Loss of pain and temperature on the same side of the face and nasal and oral cavities (uncrossed spinal trigeminal tract) Difficulty swallowing and a hoarse, weak voice. Due to damage to nucleus ambiguus Loss of gag reflex on the same side and absence of sensation of the same side due to damage to Glossopharyngeal nerve Pons Fiber Tracts Transverse: Travel through middle cerebellar peduncles. Connect pons to cerebellum. Longitudinal: Both sensory and motor. Connect spinal cord to upper brain stem: Most pass through pons without synapsing Pons Fiber Tracts Two longitudinal tracts synapse in pons: Corticopontine tracts synapse on pontine nuclei. Corticobulbar tracts (some) synapse with neurons in the trigeminal (CN V) motor nucleus and the facial (CN VII) nucleus. Nuclei in the Pons Cranial nerve nuclei: V, VI, VII, VIII (part) Pontine: Relay information from cerebrum to cerebellum. Other centers: Sleep Respiratory Pneumotaxic Apneustic Lesions in the Pons Lesion to lateral half of the pons would affect: Trigeminal nerve, resulting in: Loss of general sensation to the face on the same side. Paralysis to the muscles of mastication – with the chin deviating to the side of the lesion. Medial lemniscus Resulting in a loss of position, muscle, and joint sense on the opposite side Lesions in the Pons Lesion to lateral half of the pons would affect: Pontocerebellar fibers, resulting in: Hypotonia Coarse intention tremor Tendency to fall to the same side as the lesion. Lesions in the Pons Damage to the midpons: Extensive bilateral lesions involving the pons and the midbrain reticular formation are associated with “COMA”: State of sustained unconsciousness and unresponsiveness. Lesions in the Pons Bilateral lesions to the ventral pons: Caused by occlusion to the basilar artery that spares the reticular formation. Interrupts the corticospinal and some corticobulbar tracts. Results in a patient who is quadriplegic and unable to speak or have tongue or facial movements. Lesions in the Pons Bilateral lesions to the ventral pons: Patients are conscious. Patients can communicate with eye movements if the corticobulbar fibers to the oculomotor nuclei are intact. Midbrain Nuclei CN nuclei III and IV. Red nucleus (nucleus ruber): Involved in unconscious regulation and coordination of motor activities. Midbrain Tectum Superior colliculi: Visual reflexes. Receive input from eyes, inferior colliculi, skin, cerebrum. Fibers project to cranial nerve nuclei and to superior cervical portion of spinal cord. Stimulate motor neurons involved in turning eyes and head. Involved in visual tracking of moving objects. Midbrain Tectum Inferior colliculi: Auditory and olfactory reflexes. Midbrain Tegmentum Tracts Red nucleus: Receives information from the cerebellum and cerebral cortex. Projects to the cerebellum, spinal cord, and reticular formation: Rubrospinal tract: Neurons contribute to upper limb flexion. Midbrain Tegmentum Cerebral peduncles Interpeduncular fossa Substantia nigra: Interconnected with basal ganglia. Involved in coordinating movement and in muscle tone. Midbrain Tegmentum Oculomotor complex: Nucleus of CN III Edinger-Westphal nucleus: Parasympathetic control of pupillary sphincter and ciliary muscle. Nucleus of CN IV Periaquaductal Gray of Midbrain Gray matter surrounding the cerebral aquaduct. Involved in pain suppression. Coordinates somatic and autonomic reactions to pain, threats, and emotions. Activity results in flight-or-flight reactions and in vocalization during laughing and crying. Decerebrate rigidity Transection of the midbrain at the midcollicular level causes decerebration (disconnection) of cerebral control. Vestibular system drives the rigidity which is released from control by higher centers. Patient is comatose. Decerebrate Rigidity Characteristics: Opisthotonus (arched back) Upper extremity extension Forearm pronation Flexed wrists Lower extremity extension Plantar flexion