Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Pharmaceutical industry wikipedia , lookup
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Serotonin syndrome wikipedia , lookup
Pharmacognosy wikipedia , lookup
Toxicodynamics wikipedia , lookup
NMDA receptor wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Chlorpromazine wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Neuropharmacology wikipedia , lookup
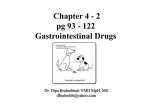
3 CE CREDITS CE Article 1 Vomiting ❯❯ H éctor J. Encarnación, DVM Gulf Coast Veterinary Specialists Houston, Texas ❯❯ J oshua Parra, DVM Florida Veterinary Referral Center and 24-Hour Emergency and Critical Care Hospital Estero, Florida ❯❯ E rick Mears, DVM, DACVIM Valerie Sadler, DVM, DACVR Florida Veterinary Specialists and Cancer Treatment Center Tampa, Florida At a Glance The Vomiting Reflex Page 122 Antiemetics Page 124 Vomiting Reflex Components, Receptors, and Controlling Neurotransmitters and Medications Page 125 Most Common Antiemetics Used in Small Animal Medicine Page 127 Treatment of Common Vomiting Conditions Page 128 Most Common Causes of Vomiting in Dogs and Cats Page 129 122 Abstract: Vomiting is the forceful expulsion of stomach contents through the mouth, caused by humoral stimulation of the chemoreceptor trigger zone (CRTZ) or neural stimulation of the emetic center. The CRTZ is activated and controlled by neurotransmitter manipulation at the receptor level. Clinical signs preceding vomiting may include ptyalism, tachycardia, depression, hiding, and yawning. Gastritis, gastrointestinal ulceration, pancreatitis, motion sickness, uremia, chemotherapy, and drug administration are common initiating causes of vomiting. This article reviews the anatomic and physiologic aspects of the vomiting reflex and its neurotransmitters, associated receptors, and rational management. E mesis, or vomiting, is one of the most common reasons dogs and cats present for medical evaluation.1 Vomiting is often associated with mild, self-limiting diseases that resolve with minimal diagnostic tests and therapy. However, it can be related to debilitating conditions that have life-threatening consequences. The history obtained from the client should be as detailed as possible because historical details are often helpful in selecting the appropriate treatment and diagnostic plan. Questions to ask during the history should include onset of vomiting, duration of clinical signs, type and frequency of vomiting, relation to food ingestion, characteristics of the vomited contents, diet history, and environment. Questions about known medical conditions and current therapies are also pertinent because these factors may play an active role in the inciting cause. The Vomiting Reflex Pathophysiology Vomiting is a reflex act that is mediated neurologically by the activation of the bilateral nucleus tractus solitarii, or emetic center, situated in the parvicellular reticular formation in the lateral region of the medulla oblongata. This is the area that initiates, controls, regulates, and organizes the vomiting reflex.2–5 Vomiting can be triggered by both neural and humoral pathways.2 The neural pathway comprises six fundamental Compendium: Continuing Education for Veterinarians® | March 2009 | CompendiumVet.com components. The emetic center (1)2,6–12 receives input from (2) the gastrointestinal tract (afferent neurons),2,7–11,13 (3) the higher centers of the brain,2,7–9,13 (4) the vestibular apparatus,2,6–13 and (5) the CRTZ.2,6–13 Finally, to coordinate the vomiting reflex, the vomiting center sends signals through (6) the efferent motor neurons.7,8,10 The vagal and sympathetic afferent neurons originate from the gastrointestinal tract, particularly the duodenum, as well as other areas, including the urinary and reproductive system, liver, pancreas, peritoneum, and cardiac vessels. Stimulation of these neurons initiates the impulse that travels directly to the emetic center. The higher centers of the brain, including the cerebral cortex and the limbic system, can trigger emesis through three mechanisms: direct stimulation of the vomiting center by inflammatory diseases, hydrocephalus, or neoplasia; psychogenic stimulation caused by fear, stress, excitement, or pain; and traumatic stimulation related to head injuries and increased intracranial pressure.7,9 The CRTZ is a bilateral set of centers in the brainstem, located on the floor of the fourth ventricle. It possesses free nerve endings that maintain direct contact with the cerebrospinal fluid via ependymal pores or the sheath surrounding fenestrated capillaries.9,14 These free nerve endings are activated by the vestibular system or through the humoral pathway by conditions affecting the blood or cerebrospinal fluid (e.g., drug administration, infection, osmolar FREE CE Vomiting and acid–base disorders, electrolyte derangements, metabolic diseases).15 Finally, to initiate the vomiting reflex, efferent motor signals must be transmitted to the upper gastrointestinal tract through the sensory aspect of cranial nerves V, VII, IX, X, and XII and to the diaphragm and abdominal muscles via the spinal nerves.8 Anatomy negative intrathoracic pressure and positive intraabdominal pressure, facilitating the movement of gastric contents into the esophagus. Before expulsion, the respiratory center is inhibited and the nasopharynx and glottis close to prevent pulmonary aspiration and nasal regurgitation of the gastric contents. The third and last phase of vomiting is the expulsion of stomach contents through the mouth. The act of vomiting is composed of three phases: nausea, retching, and Antiemetics expulsion of proximal duodenal Antiemetics are drugs that block the and gastric contents.6,7,16 Nausea is vomiting reflex 9,23,24 by impeding the conscious recognition of sub- neurotransmission at central (CRTZ, conscious excitation in an area of emetic center) and peripheral (gasthe medulla that is closely associ- trointestinal epithelium) recepated with the vomiting center. This tor sites. These drugs are classified excitation is caused by irritative based on the type of receptor they impulses coming from the gastroin- block (Table 1). However, antiemettestinal tract, lower brain, or cerebral ics have the potential to prolong gascortex.15,17–19 Ptyalism, tachycardia, trointestinal infections, predispose nervousness, hiding or seeking patients to such infections, and preattention, shivering, and yawning vent toxin elimination by decreasare all characteristic signs of nau- ing gastrointestinal motility. The use sea triggered by general activation of most of these drugs in animals of the sympathetic and parasympa- is off-label, and some dosages are thetic branches of the autonomic extrapolated from the human medinervous system. Hypersalivation cal literature (Table 2). stimulates swallowing, which stimulates relaxation of the gastroesopha- Phenothiazines geal sphincter. The bicarbonate-rich Phenothiazines are broad-specsaliva secreted by the salivary glands trum antiemetics that have antidoin the mouth lubricates the esopha- paminergic and antihistaminergic gus and helps neutralize the stom- properties at low doses in the ach’s acidic environment before CRTZ and anticholinergic effects at vomiting.8,13 Before retching, abo- higher doses at other central sites, ral gastric and esophageal motility including the emetic center.9 These diminishes and the lower esopha- drugs also block norepinephrine at peripheral α-adrenergic recepgeal and pyloric sphincters relax. Retching is the second phase of tors. Drugs in this group include vomiting and begins with the onset chlorpromazine, prochlorperazine, of a retrograde giant contraction.20,21 and acetylpromazine. Common This contraction is a single-phase, ret- adverse effects in small animals, rograde, peristaltic motion that emp- especially dogs, include ataxia, ties the proximal duodenal contents hypotension, and excessive sedainto the stomach.20–22 It is followed by tion. Generalized central nervous deep inspiratory movements, force- system (CNS) stimulation, aggresful contractions of the abdominal siveness, violent behavior, extrapymuscles and diaphragm, and closure ramidal effects, and seizures are of the glottis. These actions produce rare. Fluid therapy is indicated in 124 Compendium: Continuing Education for Veterinarians® | March 2009 | CompendiumVet.com FREE Vomiting CE patients undergoing phenothiazine therapy because of the vasodilatory properties of these drugs. Anticholinergics Anticholinergic drugs block cholinergic afferent pathway transmission from the gastrointestinal tract (peripheral action) and the vestibular system to the emetic center (central action).9 Scopolamine and isopropamide are centrally acting anticholinergics that cross the blood–brain table 1 barrier. They have a short duration of action and can cause excitement in cats. Peripherally acting anticholinergics include propantheline and methscopolamine. Isopropamide and propantheline are the drugs in this group that are most commonly used in small animals for vomiting related to motion sickness.25 Side effects reported in humans and small animals include xerostomia (dry mouth), sedation, visual disturbances, drowsiness, dysphoria, confusion, gastrointestinal ileus, and disorientation.9,26 Vomiting Reflex Components, Receptors, and Controlling Neurotransmitters and Medications Receptor Receptor Agonists Receptor Antagonists Chemoreceptor trigger zone D2-Dopaminergic Dopamine etoclopramide M rochlorperazine P Trimethobenzamide Acetylpromazine Chlorpromazine aloperidol H Droperidol M1-Cholinergic Acetylcholine ropantheline P hlorpromazine C Isopropamide Scopolamine Prochlorperazine ethscopolamine M Acetylpromazine H1-Histaminergic Histamine iphenhydramine D rochlorperazine P Dimenhydrinate Chlorpromazine Meclizine Acetylpromazine Promethazine α2-Adrenergic Norepinephrine rochlorperazine P Chlorpromazine ohimbine Y Acetylpromazine 5-HT3-Serotonergic Serotonin ndansetron O Dolasetron irtazapine M Propofol etoclopramide M Granisetron ENKµ,δ-Enkephalinergic Met-enkephalin Leu-enkephalin Butorphanol Neurokinin-1 antagonist Substance P Maropitant 5-HT1A-Serotonergic Serotonin Diphenhydramine Dimenhydrinate Meclizine α2-Adrenergic Norepinephrine Prochlorperazine Chlorpromazine Yohimbine Glucocorticoid receptors Dexamethasone Cyproterone Mifepristone Neurokinin-1 antagonist Substance P Maropitant M1-Cholinergic Acetylcholine ropantheline P hlorpromazine C Isopropamide Scopolamine Prochlorperazine Methscopolamine Acetylpromazine H1-Histaminergic Histamine iphenhydramine D Dimenhydrinate Meclizine rochlorperazine P Chlorpromazine Diazepam yclizine C Promethazine 5-HT3-Serotonergic Serotonin ndansetron O Dolasetron irtazapine M Metoclopramide Granisetron Neurokinin-1 antagonist Substance P Maropitant D2-Dopaminergic Dopamine etoclopramide M rochlorperazine P Trimethobenzamide Acetylpromazine Chlorpromazine aloperidol H Droperidol 5-HT4-Serotonergic Cisapride Metoclopramide Serotonin Piboserod M2-Cholinergic Acetylcholine ropantheline P Isopropamide Prochlorperazine Motilin Erythromycin Motilin QuickNotes Emetic center Vomiting is a neurologically mediated reflex that depends on neural or humoral activation of the emetic center. Vestibular apparatus Vagal afferents Vagal efferents hlorpromazine C Scopolamine ethscopolamine M Acetylpromazine — CompendiumVet.com | March 2009 | Compendium: Continuing Education for Veterinarians® 125 FREE CE Vomiting Antihistamines Antihistamines can intercept cholinergic and histaminic nerve transmission responsible for vestibular stimulation of the vomiting center.25 Drugs in this classification include diphenhydramine, dimenhydrinate, and meclizine. These drugs display H 1-antihistaminergic properties and are mainly used to control the clinical signs of motion sickness. Mild sedation, xerostomia, and drowsiness are some of the adverse effects. Meclizine can be teratogenic if administered at high doses.25 Cats do not have histamine receptors in the CRTZ, and antihistaminic drugs do not control their vomiting.27 Serotonin Antagonists QuickNotes Antiemetics are drugs that block specific superficial cell receptor sites, consequently disrupting the vomiting reflex. Serotonin antagonists are specific inhibitors of 5-HT-serotonergic receptors. They control vomiting by acting on receptors located on the periphery of vagal nerve terminals and centrally on the CRTZ.25,26 These receptors are normally stimulated by serotonin released from the enterochromaffin cells of the small intestine in response to damage to the gastrointestinal mucosa. Ondansetron, a member of this class of antiemetic drugs, has been shown to control vomiting in dogs28,29 and is used in dogs receiving radiation and chemotherapy when metoclopramide and other antiemetics fail to control vomiting.28,29 Dolasetron, another member of this group, acts on receptors in the CRTZ.25 Both of these drugs are used extensively in human medicine, and they seem to be safe antiemetic alternatives in veterinary medicine.30,31 However, they are not effective in controlling vomiting caused by motion sickness.25,26 Side effects of these drugs that have been reported in people include electrocardiographic changes, including PR and QT prolongation and QRS widening, that are believed to be caused by sodium channel blockage by dolasetron metabolites. Diarrhea, headache, dizziness, and musculoskeletal pain have been reported as well. These medications can be expensive. Substituted Benzamides Substituted benzamides exert antiemetic effects through different mechanisms. Some, such as metoclopramide and trimethobenzamide, antagonize dopamine receptors in the CNS and block 5-HT3-serotonergic receptors when administered 126 at high concentrations.9,25 Metoclopramide is known for its potent dopaminergic antagonism, but trimethobenzamide, which is also a weak antihistamine, has not been a very effective antidopaminergic agent clinically. Metoclopramide has more action on D2-dopaminergic receptors than trimethobenzamide and is 20 times more potent than phenothiazines.7 As a result, metoclopramide should not be used in patients receiving dopamine.12 Cisapride, another substituted benzamide, activates neuronal 5-HT4 receptors, which facilitates gastric emptying. Metoclopramide also activates neuronal 5-HT4 receptors and blocks 5-HT3 -serotonergic receptors, increases the lower esophageal sphincter tone, and enhances aboral gastrointestinal motility; therefore, these drugs are classified as prokinetics as well.9 Adverse effects of these drugs include CNS excitement and behavioral changes, especially during rapid intravenous administration or if given at high doses. Metoclopramide controls peripherally induced and humorally mediated vomiting due to numerous conditions, but it should be avoided if gastrointestinal obstruction is suspected because its prokinetic properties could predispose these patients to gastric or intestinal perforation. This contraindication also applies to cisapride. Butyrophenone and Benzimidazole Derivatives Butyrophenone derivatives (e.g., haloperidol, droperidol) are potent dopamine antagonists in the CRTZ and are used as tranquilizers.9 Their side effects are very similar to those of phenothiazines. The benzimidazole derivatives antagonize dopamine receptors in the gastrointestinal smooth muscle and display prokinetic properties like those of metoclo pramide,32 but their use in veterinary medicine is minimal if any. Opioids Enkephalins—endogenous opiates belonging to the endorphin family—are believed to have antiemetic properties. Neurons containing enkephalins have been identified near the CRTZ and the emetic center.33 Evidence suggests that opioid κ and/or μ receptors are present in the vomiting center and are involved in inhibition of emesis in dogs and cats.34 Butorphanol, a pri- Compendium: Continuing Education for Veterinarians® | March 2009 | CompendiumVet.com FREE Vomiting CE table 2 Most Common Antiemetics Used in Small Animal Medicine Drugs Site of Action Dosage Side Effects Prochlorperazinea,13 CRTZ and emetic center Dogs and cats: 0.1–0.5 mg/kg SC or IM q6–8h Hypotension, sedation Chlorpromazinea,2,13 CRTZ and emetic center Dogs: 0.1–0.5 mg/kg SC, IM, or IV q6–8h Cats: 0.2–0.5 mg/kg SC, IM, or IV q6–8h Hypotension, sedation Yohimbinea,2 CRTZ and emetic center Dogs: 0.25–0.5 mg/kg SC or IM q12h Hypotension, sedation Metoclopramidea,2,13 CRTZ, GI smooth muscle Dogs: 0.1–0.4 mg/kg PO, SC, or IM q6h Cats: 0.2–0.4 mg/kg PO, or SC q6–8h CRI: 1–2 mg/kg/day Extrapyramidal signs, constipation Trimethobenzamide2,13 CRTZ Dogs: 3 mg/kg IM q8–12h Allergic reactions Diphenhydraminea,2,13 CRTZ Dogs and cats: 2–4 mg/kg PO or IM q8h Sedation, GI effects Dimenhydrinate CRTZ Dogs and cats: 4–8 mg/kg PO q8h Sedation, GI effects CRTZ Dogs and cats: 4 mg/kg PO q24h Sedation, xerostomia, tachycardia Propanthelinea Parasympathetic nervous system Dogs and cats: 0.25 mg/kg PO q8h Gastric retention, ileus, tachycardia Isopropamideb Parasympathetic nervous system Dogs and cats: 0.2–0.4 mg/kg PO q8–12h Gastric retention, ileus, tachycardia Ondansetrona,2 CRTZ and vagal afferent neurons Dogs: 0.11–0.176 mg/kg slow IV push q24h Cats: 0.1–0.15 mg/kg slow IV push q24h Sedation Dolasetrona CRTZ Dogs: 0.6 mg/kg IV q24h or 0.5 mg/kg PO, SC, or IV q24h Cats: 0.6 mg/kg IV q12h or 0.6–1 mg/kg PO q12h Electrocardiogram changes Mirtazapinea CRTZ and vagal afferent neurons Dogs: 0.6 mg/kg PO q24h, not to exceed 30 mg/day Cats: 3–4 mg/cat PO q72h Sedation, ataxia, depression, vocalization CRTZ and emetic center Dogs: 1 mg/kg SC q24h up to 5 days or 2 mg/kg PO q24h up to 5 days Injection site soreness, ataxia, anorexia, diarrhea Myenteric neurons Dogs: 0.1–0.5 mg/kg PO q8h Cats: 0.1–1.0 mg/kg or 5 mg (total dose) PO q8–12h None GI smooth muscle Dogs and cats: 0.5–1.0 mg/kg IV q8h, up to 5.0 mg/kg PO q8h Vomiting at antimicrobial doses (15 mg/ kg tid) Emetic center Dogs: 0.2–0.4 mg/kg IM 30 min before cisplatin infusion Sedation, ataxia, anorexia, diarrhea CRTZ None reported in veterinary medicine Apnea, hypotension, seizurelike signs Emetic center, medulla Dogs: 0.1 mg/kg SC or IV before chemotherapy GI ulceration Vestibular system suppression 0.1–0.2 mg/kg PO q6h Sedation α2-Adrenergic antagonists D2-Dopaminergic antagonists H1-Histaminergic antagonists Meclizine a,2,13 a M1-Cholinergic antagonists 5-HT3-Serotonergic antagonists NK1-Neurokinin antagonist Maropitant40 5-HT4-Serotonergic antagonist Cisapridea,2 Motilin agonist Erythromycina,2 Opioid Butorphanola,13 Others Propofola Dexamethasone Diazepam a 13 Plumb DC. Veterinarian Drug Handbook. 6th ed. Ames, IA: Wiley-Blackwell; 2008. b Richter KP. Treating acute vomiting in dogs and cats. Vet Med 1992;87(8):814-818. a CompendiumVet.com | March 2009 | Compendium: Continuing Education for Veterinarians® 127 FREE CE Vomiting marily κ and σ agonist, is used to prevent vomiting related to cisplatin therapy in dogs.35,36 Neurokinin Antagonists QuickNotes Phenothiazines are broad-spectrum antiemetics that have antidopaminergic and antihistaminergic properties in the CRTZ and anticholinergic effects in the emetic center. 128 Neurokinin (NK1) antagonists are a new group of antiemetics that includes maropitant, an agent developed for dogs that acts as a ligand for the substance P receptors located in many areas of the brain, including the emetic center and CRTZ.37 It is believed that the substance P–NK1 receptor complex is in the final common pathway of the neural and humoral pathways of the vomiting reflex.38 Studies in dogs have showed that maropitant prevents vomiting caused by peripheral and central emetogens, including apomorphine, cisplatin, and syrup of ipecac,39 and clinical conditions such as pancreatitis and gastroenteritis.39 Maropitant is also effective against vomiting caused by motion sickness.39 Adverse effects reported with this drug include ataxia, anorexia, diarrhea, and injection site soreness.40 This drug should not be used in dogs younger than 16 weeks because bone marrow hypoplasia has been reported.40 Other Drugs Other drugs used to control vomiting centrally include yohimbine, diazepam, dexamethasone, propofol, and mirtazapine. Yohimbine, a pure α2-adrenergic antagonist, is a very potent antiemetic used in dogs and cats. It may cause CNS excitement, excessive sedation, muscle tremors, tachypnea, ptyalism, and hyperemic mucous membranes.36 Diazepam relieves nausea and vomiting in people.41 Studies with animal models and clinical trials in human medicine suggest that this drug suppresses the vestibular system.41–43 The antiemetic properties of corticosteroids are incompletely understood, but their mechanism involves the activation of glucocorticoid receptors in the medulla, especially the emetic center in cats.44 Dexamethasone has been shown to be useful in controlling chemotherapy-associated nausea and vomiting in human patients45 and dogs.45,46 Propofol, an alkylphenol derivative, is used as an antiemetic in people with chemotherapy-associated nausea and vomiting that is unresponsive to serotonin antagonists or dexamethasone.47,48 It has been proposed that its antiemetic mechanism involves reduction of the serotonin concentration in the CRTZ via γ-aminobutyric acid activity and 5-HT3 serotonin receptor antagonism.49 Mirtazapine is a piperazinoazepine drug used as an antidepressant in people. It antagonizes central presynaptic α2-receptors and blocks serotonin receptors.50 It is a weak 5-HT1 serotonin receptor antagonist, a potent 5-HT2 and 5-HT3 serotonin receptor antagonist, and an H1-histamine antagonist.50 It is used to control chemotherapy-associated nausea and vomiting in humans50,51 and, more recently, in small animals. Treatment of Common Vomiting Conditions Box 1 lists several conditions and diseases that commonly cause vomiting. Gastritis or Gastric Ulceration Treatment to manage vomiting caused by gastritis or gastric ulceration must include proper fluid therapy and gastric mucosal protection. Many clinicians use broad-spectrum antiemetics because they cover local and peripheral receptors. Chlorpromazine, serotonin antagonists, and metoclopramide are good options. Maropitant seems to work extremely well in dogs. If vomiting is associated with gastrointestinal ulceration due to NSAID administration, therapy with misoprostol, a prostaglandin E1 (PGE) analog, may be effective in controlling both the ulcerative lesion and vomiting as a secondary problem.52 Proton pump inhibitors and H2-histamine antagonists provide more complete inhibition of gastric acid secretion in severe cases of ulceration.12,25,53 If Helicobacter spp are the underlying cause of ulceration, appropriate antibiotic therapy and antacids should relieve the clinical signs of the infection. Patients with neoplastic diseases often have gastrointestinal ulceration. Mast cell tumors of any stage, grade, and size can cause vomiting in dogs by increasing the plasma histamine concentration.16,54 Histamine acts on the CRTZ and the gastric mucosa. Mast cell tumor ulceration and its effects are treated with H2-histamine antagonists. Tumor size and histamine release in dogs are controlled with the administration of corticosteroids.12,55 Pancreatitis Pancreatitis causes ileus due to intestinal inflammation, resulting in direct afferent input to the vomiting center.12 Metoclopramide is the most common antiemetic used in these patients because it acts centrally and peripherally. In dogs, phenothiazines, 5-HT 3 -serotonergic Compendium: Continuing Education for Veterinarians® | March 2009 | CompendiumVet.com FREE Vomiting CE antagonists, and maropitant can be useful if metoclopramide fails to control vomiting. Emesis caused by cancer chemotherapy and other drugs (e.g., digitalis) is mediated by 5-HT3-serotonergic receptors.2,12,25 In humans, the chemotherapeutic drugs most commonly associated with vomiting include cisplatin, cyclophosphamide, dacarbazine, and doxorubicin.56 Drugs with 5-HT3-serotonergic antagonist properties, especially the serotonin antagonists ondansetron, granisetron, dolasetron, block these receptors in the CRTZ in cats and in the vagal afferent neurons in dogs.25,26,28,29,57 Metoclopramide is widely used to control chemotherapy-induced vomiting.6,58 The new agent maropitant is also effective in controlling cisplatin-induced vomiting in dogs, and even though there is coexpression of substance P with 5-HT receptors in the primate brain,37 this has not been documented in dogs or cats. ing inputs from the two vestibular systems (the semicircular canals and the otolith organs); or (3) comparison of input from these systems with the individual’s expectations derived from previous experiences.59 Vomiting caused by motion sickness involves M1-cholinergic and H1-histaminergic receptors,2,11 and treatment should antagonize both receptors. Phenothiazines like chlorpromazine and prochlorperazine can antagonize both receptors at the same time, but diphenhydramine, dimenhydrinate, cyclizine, meclizine, and promethazine are H1-histamine blocking agents only, and they should be combined with a M1-cholinergic receptor blocker for effective control of emetic signals originating from the vestibular apparatus. Maropitant prevents kinetosis in dogs by blocking the final common pathways of the vomiting reflex, including signals from the vestibular system.40 Scopolamine is a muscarinic M1-cholinergic antagonist used to treat motion sickness, but results are not consistent. Motion Sickness Uremia Motion sickness, or kinetosis, is generated from the vestibular apparatus.2,9,11 Studies in humans have revealed that motion sickness is caused by three mechanisms: (1) conflicting inputs from the visual and vestibular systems; (2) conflict- Uremic toxins cause decreased gastrin clearance and irritate the gastrointestinal mucosa, resulting in ulcerative lesions and gastritis. When these toxins cross the blood–brain barrier, they stimulate central and peripheral receptors and activate D2-dopaminergic receptors in the CRTZ.2,11 Dopamine antagonists like metoclopramide and chlorpromazine effectively block these receptors. Diuresis with appropriate fluid therapy and a proton pump inhibitor or H2-histaminergic antagonist helps relieve uremia by diminishing the secretion of hydrogen ions into the stomach, providing protection and promoting mucosal healing. Chemotherapy and Other Drugs Box 1 Most Common Causes of Vomiting in Dogs and Cats bdominal disorders A Dietary factors Disorders of the small and large intestines Disorders of the stomach Drugsa Endocrine disorders ❯ Hypoadrenocorticism ❯ Hypoparathyroidism Neurologic disorders Parasitism ❯ Ollulanus tricuspis in cats ❯ Physaloptera ❯ Salmon poisoning (Neorickettsia helminthoeca) Systemic diseases Toxins, chemicals, and poisons a Almost any drug can cause vomiting, especially if given orally. QuickNotes Vomiting caused by motion sickness involves M1-cholinergic and H1-histaminergic receptors, and treatment should antagonize both receptors. Gastrointestinal Motility Disorders Prokinetics—cisapride, metoclopramide, and erythromycin—should be used to control vomiting due to nonobstructive delayed gastric emptying. These drugs exert their effects on different receptors. Cisapride, the most effective prokinetic agent available,11 lacks direct antiemetic effects but stimulates 5-HT4-serotonergic receptors.60 Metoclopramide’s antagonism of D2-dopaminergic receptors enables it to stimulate motility in areas where these receptors are present (the higher gastrointestinal tract, lower esophageal sphincter, stomach, and duode- CompendiumVet.com | March 2009 | Compendium: Continuing Education for Veterinarians® 129 FREE CE Vomiting QuickNotes Patients with vomiting of undetermined etiology must be treated with the safest approach possible once systemic diseases have been ruled out. 130 num).2,11 Erythromycin, a macrolide used for its antimicrobial properties, is useful as a prokinetic at low doses.2,11 In dogs, it stimulates the release of motilin, which initiates phase III of the migrating myoelectric complex,61,62 the sequence of motor activity during the interdigestive period in the small bowel.63 This cyclic pattern originates in the gastric antrum and extends over the entire length of the small intestine.62,63 The third and final phase of this pattern is generally associated with the propulsion of ingesta.64,65 It is unknown whether cats can benefit from this effect. Dogs that vomit bile in the morning before eating may have bilious vomiting syndrome. This is a condition characterized by grass ingestion, vomiting, and lack of other definitive clinical signs. It mostly occurs in the morning and is believed to be commonly associated with gastritis, inflammatory bowel disease, and bile and gastroesophageal reflux. Affected patients usually respond to a single evening dose of cisapride, metoclopramide, or erythromycin. References 1. Tams TT. A diagnostic approach to vomiting in dogs and cats. Vet Med 1992;87(8):785-792. 2. Washabau RJ, Elie S. Antiemetic therapy. In: Kirk RW, Bonagura JD, eds. Kirk’s Current Veterinary Therapy XII Small Animal Practice. Philadelphia: WB Saunders; 1995:679-684. 3. Andrews PLR, Rapeport WG, Sanger GJ. Neuropharmacology of emesis induced by anti-cancer therapy. Trends Pharmacol Sci 1988;9:334341. 4. Johnson SE. Clinical pharmacology of antiemetics and antidiarrheals. Proc of the Kal Kan Waltham Symp Treat Small Anim Dis 1984;8:7-15. 5. Merrifield KR, Chaffee BJ. Recent advances in the management of nausea and vomiting caused by antineoplastic agents. Clin Pharm 1989;8:187-199. 6. Leib MS. Acute vomiting: a diagnostic approach and symptomatic management. In: Kirk RW, Bonagura JD, eds. Kirk’s Current Veterinary Therapy XI Small Animal Practice. Philadelphia: WB Saunders; 1995:583587. 7. Burrows CF. Vomiting and Regurgitation in the Dog: A Clinical Perspective. Lehigh, Pennsylvania. ALPO Pet Center; 1990:18-38. Viewpoints in Veterinary Medicine. 8. Guyton AC, Hall JE. Textbook of Medical Physiology. 9th ed. Philadelphia: WB Saunders; 1996. 9. Adams HR. Veterinary Pharmacology and Therapeutics. 8th ed. Ames: Iowa State University Press; 2001. 10. Cunningham JG. Textbook of Veterinary Physiology. 3rd ed. Philadelphia: WB Saunders; 1997. 11. Richter K. Approach to acute vomiting. Proc WVC 2004. Accessed January 2009 at vin.com/Members/Proceedings/Proceedings.plx?CID=wv c2004&PID=pr05345&O=VIN. 12. Simpson KW. Managing persistent vomiting. Proc ACVIM 2003. Accessed January 2009 at vin.com/Members/Proceedings/Proceedings.plx? CID=acvim2003&PID=pr03873&O=VIN. 13. Strombeck DA, Guilford WG. Vomiting: pathophysiology and pharmacology control. In: Strombeck DA, Guilford WG, Center SA, et al, eds. Strombeck’s Small Animal Gastroenterology. 3rd ed. Philadelphia: WB Saunders; 1996:256-260. 14. Willard MD. Some new approaches to the treatment of vomiting. JAVMA 1984;184:590. 15. Miller AD, Leslie RA. The area postrema and vomiting. Front Neuroendocrinol 1994;15(4):301-320. 16. Twedt DC. Vomiting. In: Ettinger SJ, Feldman EC, eds. Textbook of Veterinary Internal Medicine. 6th ed. Philadelphia: WB Saunders; 2005:132136. Undetermined Etiology Patients with vomiting of undetermined etiology must be treated with the safest approach possible once systemic diseases (e.g., liver disease, renal disease, endocrine disease) have been ruled out. Patients that are uncomfortable from excessive vomiting or are at high risk for aspiration pneumonia and have not been exposed to a toxic agent should be treated with antiemetics when available. α2-Adrenergic antagonists and D2-dopaminergic receptors are first-line antiemetics. Maropitant is a good alternative not only because it seems to block impulses in the final common pathways of the vomiting reflex but also because it is administered once daily, dogs seem to tolerate it fairly well, and, so far, adverse effects are minimal. 5-HT3-serotonergic antagonists have become very popular over the past few years and have good results. The addition of other drugs to antiemetic therapy should be considered if vomiting becomes refractory in these patients. 17. Miller AD. Central mechanisms of vomiting. Dig Dis Sci 1999; 44(8 suppl):31S-43S. 18. Miller AD, Nonaka S, Jakus J, et al. Modulation of vomiting by the medullary midline. Brain Res 1996;737(1-2):51-58. 19. Miller AD, Nonaka S, Jakus J. Brain areas essential or non-essential for emesis. Brain Res 1994;647(2):255-264. 20. Lang IM, Dana N, Medda BK, et al. Mechanisms of airway protection during retching, vomiting, and swallowing. Am J Physiol Gastrointest Liver Physiol 2002;283(3):G529-G536. 21. Sarna SK, Otterson MF. Small intestinal physiology and pathophysiology. Gastroenterol Clin North Am 1989;18(2):375-404. 22. Furukawa N, Hatano M. An acute experiment on retrograde intestinal peristalsis with emesis using decerebrated dogs. J Auton Nerv Syst 1998;70(1-2):56-65. 23. Peroutka SJ, Snyder SH. Antiemetics: neurotransmitter receptor binding predicts therapeutic actions. Lancet 1982;1(8273):658-659. 24. Costall B, Naylor RJ. Neuropharmacology of emesis in relation to clinical response. Br J Cancer Suppl 1992;19:S2-S8. 25. Dowling PM. GI therapy: when what goes in won’t stay down. Proc WVC 2003. Accessed January 2009 at vin.com/Members/Proceedings/ Proceedings.plx?CID=wvc2003&PID=pr03480&O=VIN. 26. Flake ZA, Scalley RD, Bailey AG. Practical selection of antiemetics. Am Fam Phys 2004;69:1169-1174,1176. 27. King GL. Animal models in the study of vomiting. Can J Physiol Pharmacol 1990;68:260. 28. Martirosov KS, Grigor’ev IuG, Borovkov MV, Zorin VV. Experimental study of the role of blocking 5-HT3-receptors of serotonin and D2-receptors of dopamine in the mechanism of early radiation vomiting in dogs. Radiats Biol Radioecol 2002;42(1):75-79. 29. Martirosov KS, Grigor’ev IuG, Borovkov MV, Zorin VV. Comparative experimental study of antiemetic action of lantranum in radiation-induced vomiting and vomiting caused by apomorphine. Radiats Biol Radioecol 2003;43(1):60-64. 30. Product information: Zofran. Research Triangle Park, NC: GlaxoSmithKline; 2006. 31. Andrews PLR, Naylor RJ, Joss RA. Neuropharmacology of emesis and its relevance to anti-emetic therapy: consensus and controversies. Support Care Cancer 1998;6:197-203. 32. Takahashi T, Kurosawa S, Wiley JW, et al. Mechanism for the gastrokinetic actions of domperidone. Gastroenterology 1991;101:703-710. 33. Kolh RL, MacDonald S. New pharmacologic approaches to the prevention of space/motion sickness. J Clin Pharmacol 1991; 31(10):934-946. Compendium: Continuing Education for Veterinarians® | March 2009 | CompendiumVet.com FREE Vomiting CE 34. Kobrinsky NL. Regulation of nausea and vomiting in cancer chemotherapy. A review with emphasis on opiate mediators. Am J Pediatr Hematol Oncol 1988;10(3):209-213. 35. Schurig JE, Florczyk AP, Rose WC, et al. Antiemetic activity of butorphanol against cisplatininduced emesis in ferrets and dogs. Cancer Treat Rep 1982;66(10):1831-1835. 36. Plumb DC. Veterinary Drug Handbook. 4th ed. Ames: Iowa State Press-Blackwell; 2002. 37. Davis KL, Charney D, Coyle JT, Nemeroff C. Neuropsychopharmacology: The Fifth Generation of Progress. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2002;169-177. 38. Hornby PJ. Central neurocircuitry associated with emesis. Am J Med 2001;111(suppl 8A):106S-112S. 39. Benchaoui HA, Cox SR, Schneider RP, et al. The pharmacokinetics of maropitant, a novel neurokinin type-1 receptor antagonist in dogs. J Vet Pharmacol Ther 2007;30(4):336-344. 40. Product information: Cerenia. New York: Pfizer Animal Health: 2006. 41. McClure JA, Lycett P, Baskerville JC. Diazepam as an anti-motion sickness drug. J Otolaryngol 1982;11(4):253-259. 42. Sekitani T, McCabe BF, Ryu JH. Drug effects on the medical vestibular nucleus. Arch Otolaryngol 1971;93:581-589. 43. Zanjoc TP, Roland PS. Vertigo and motion sickness. Part II: pharmacologic treatment. Ear Nose Throat J 2006;85(1):25-35. 44. Ho GM, Ho ST, Wang JJ, et al. Dexamethasone has a central antiemetic mechanism in decerebrated cats. Anesth Analg 2004;99(3):734-739. 45. Dexamethasone alone or in combination with ondansetron for the prevention of delayed nausea and vomiting induced by chemotherapy. The Italian Group for Antiemetic Research. N Engl J Med 2000;342(21):1554-1559. 46. Fukui H, Yamamoto M. Methotrexate produces delayed emesis in dog: a potential model of delayed emesis induced by chemotherapy. Eur J Pharmacol 1999;372:261-267. 47. Borgeat A, Wilder-Smith OH, Saiah M, et al. Subhypnotic doses of propofol possess direct antiemetic properties. Anesth Analg 1992;74:539-541. 48. Gan TJ, El-Molem H, Ray J, et al. Patient-controlled antiemesis: a randomized, double-blind comparison of two doses of propofol versus placebo. Anesthesiology 1999;90:1564-1570. 49. Cechetto DF, Daib T, Gibson CJ, Gelb AW. The effect of propofol in the area postrema in rats. Anesth Analg 2001;92:934-942. 50. Pae C. Low-dose mirtazapine may be successful treatment option for severe nausea vomiting. Prog Neuropsychopharmacol Biol Psychiatry 2006;30:1143-1145. 51. Kang H, Kim S, Kim J, et al. Mirtazapine for severe gastroparesis unresponsive to conventional prokinetic treatment. Psychosomatics 2006;47:5. 52. Murtaugh RJ, Matz ME, Labata MA, et al. Use of synthetic prostaglandin E1 (misoprostol) for prevention of aspirin-induced gastroduodenal ulceration in arthritic dogs. JAVMA 1993;202(2):251256. 53. Bersenas AME, Mathews KA, Allen DG, et al. Effects of ranitidine, famotidine, pantoprazole, and omeprazole on intragastric pH in dogs. Am J Vet Res 2005;66(3):425-431. 54. Fox LE, Rosenthal RC, Twedt DC, et al. Plasma histamine and gastrin concentrations in 17 dogs with mast cell tumors. J Vet Intern Med 1990;4:242. 55. Ogilvie GK. Mast cell tumors: hot new diagnostics and treatment! Proc WSAVA 2002. Accessed January 2009 at vin.com/Members/Proceedings/Proceedings.plx?CID=wsava2002&PID =pr02637&O=VIN. 56. American Cancer Society. Nausea and vomiting. Accessed January 2009 at cancer.org/docroot/MBC/content/MBC_2X_Nausea_and_Vomiting.asp?sitearea=MBC. 57. Tucker ML, Jackson MR, Scales MDC, et al. Ondansetron: pre-clinical safety evaluation. Eur J Cancer Clin Oncol 1989;25:S79. 58. Ogilvie GK, Moore AS, Curtis CR. Evaluation of cisplatin-induced emesis in dogs with malignant neoplasia: 115 cases (1984-1987). JAVMA 1989;195:1399. 59. Eyeson-Annan M, Peterken C, Brown B, et al. Visual and vestibular components of motion sickness. Aviat Space Environ Med 1996;67(10):955-962. 60. Gullikson GW, Loeffler RF, Viriña AM. Relationship of serotonin-3 receptor antagonist activity to gastric emptying and motor-stimulating actions of prokinetic drugs in dogs. J Pharmacol Exp Ther 1991;258:103. 61. Itoh Z. Erythromycin mimics exogenous motilin in gastrointestinal contractile activity in the dog. Am J Physiol 1984;247:G688. 62. Granger DN, Barrowman JA, Kvietys PR. Clinical Gastrointestinal Physiology: A Saunders Monograph in Physiology. Philadelphia: WB Saunders; 1985. 63. Thomas EA, Sjovall H, Borstein JC. Computational model of the migrating motor complex of the small intestine. Am J Physiol Gastrointest Liver Physiol 2004;286(4):G564-G572. 64. Kruis W, Azpiroz F, Phillips SF. Contractile patterns and transit of fluid in canine terminal ileum. Am J Physiol 1985;249(2 Pt 1):G264-G270. 65. v Schönfeld J, Evans DF, Goebell H, et al. Comparison of the small bowel motor response to solid and liquid meals in man. Digestion 1997;58(4):402-406. 3 CE CREDITS This article qualifies for 3 contact hours of continuing education credit from the Auburn University College of Veterinary Medicine. Subscribers may take individual CE tests online and get real-time scores at CompendiumVet.com. Those who wish to apply this credit to fulfill state relicensure requirements should consult their respective state authorities regarding the applicability of this program. CE Test 1 1.Emesis is initiated, controlled, regulated, and organized by the a.higher centers of the brain. b.CRTZ. c.vestibular apparatus. d.emetic center. 2. The vomiting pathways are controlled by a.neurotransmitter–receptor interactions. b.the higher centers of the brain. c.the peripheral nervous system. d.vestibular neurons. 3.___________ are considered broadspectrum antiemetics because of their effect on multiple receptors. a.Anticholinergics b.Phenothiazines c.Serotonin antagonists d.Opioids 4.Emesis caused by cancer chemotherapy and other drugs is mediated by ___________ receptors. a.D2-dopaminergic b.M1-cholinergic c.H2-histaminergic d.5-HT3-serotonergic 5.Which antiemetic is also classified as a prokinetic? a.ranitidine b maropitant c.metoclopramide d.propofol 6.Which condition or pathogen is the least likely to cause gastric ulceration? a.Helicobacter spp b.mast cell tumor c.gastrinoma d.kinetosis 7.Mirtazapine does not antagonize ___________ receptors. a.H1-histaminergic b.5-HT3-serotonergic c.central presynaptic α2 d.D2-dopaminergic 8.___________ can be used for chemotherapy-associated nausea and/or vomiting, especially when patients do not respond to the newer serotonin antagonists and when multiple medication therapy fails. a.Propofol b.Diazepam c.Mirtazapine d.Dexamethasone 9.Which antiemetic antagonizes neurokinin receptors in many areas of the brain? a.mirtazapine b.maropitant c.dolasetron d.prochlorperazine 10. S elect the correct antiemetic–adverse effect pair. a.ondansetron; renal toxicity b.chlorpromazine; hypotension c.metoclopramide; sedation d.meclizine; gastrointestinal perforation CompendiumVet.com | March 2009 | Compendium: Continuing Education for Veterinarians® 131