Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Discovery and development of antiandrogens wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Toxicodynamics wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
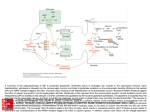
Dr. P.M. van Zyl Department of Pharmacology 2010 A major cause of disability and death worldwide. Economists: treatment of dementia will consume the entire gross national product of western countries by 2050. Alzheimer’s disease: leading cause of dementia, fourth in mortality in the US. Cholinergic hypothesis Glutamate hypothesis ?Combination: Glutamate an executor of neurodegenerative processes, and cholinergic neurones one of the victims. Olney and coworkers (1998): two phases: 1. over activation of NMDA receptors damage of neurones bearing this receptor subtype - in particular GABAergic neurones 2. secondary hypofunctional state of NMDA receptors ( due to cell loss). Loss of inhibitory (GABA) neurones in brain further neurotoxicity due to disinhibition. Main excitatory neurotransmitter Rapidly convey sensory information, motor commands Thoughts and memories Most neurons and glia contain high [glutamate]. Released for milliseconds to communicate with other neurons via synaptic endings 3 classes of ionotropic channels: AMPA receptors, kainate receptors and NMDA receptors. NMDARs most permeable to Ca2+. Schematic presentation of the glutamatergic synapse and major ionotropic glutamate receptors – AMPA and NMDA. NMDA channel activated for only brief periods due to relief of Mg2+ blockade, which occurs after cation influx into the neuron via AMPAsensitive glutamate receptor channels Synaptic plasticity in CNS : detection of relevant signal over existing background noise long lasting alteration in synaptic strength. NMDA receptors plays central role in such alterations and an endogenous “noise suppressant” is magnesium. Powerful: ◦ Too much, too long excite cells to death ◦ Excessive activation of NMDAR free radicals and activation of proteolytic processes cell injury/death. ◦ Cleared by glutamate transporters Ionic homeostasis energy dependent ◦ Energy compromised neurons become depolarized (more positively charged) relieves normal block of NMDARcoupled channels by Mg2+. Glutamate-related neuronal cell injury and death ◦ occurs in part because of overactivation of Nmethyl-d-aspartate (NMDA)-sensitive glutamate receptors, permitting excessive Ca2+ influx through the receptor’s associated ion channel. Alzheimer’s disease Parkinson’s disease Huntington’s disease HIV-associated dementia Multiple sclerosis Amyotrophic lateral sclerosis (ALS) Neuropathic pain Glaucoma Stroke, CNS trauma and seizures Glutamate and glycine bind cell is depolarized to remove Mg2+ block NMDAR channel opens influx of Ca2+ and Na+. Potential therapeutic benefit in range of neurological disorders. Must leave normal NMDAR function relatively intact ◦ LTP in hippocampus: cellular–electrophysiological correlate of learning and memory formation. ◦ Reticular activating system in brainstem: if compromised: drowsiness, even coma. Competitive antagonists of glutamate or glycine block normal function, not pathological function. Displaced from receptor by the high local concentrations of glutamate or glycine that can exist under excitotoxic conditions. ◦ Neuroprotective dose of MK-801: coma ◦ Phencyclidine “Angel Dust” hallucinations ◦ Ketamine: narcosis Theoretic solution: ‘uncompetitive’ antagonist. (An inhibitor whose action is contingent on prior activation of the receptor by the agonist.): blocks higher concentrations of agonist to a greater degree than lower concentrations of agonist. Relatively low-affinity, open-channel blocker — only enter channel when it is opened by agonist. Relatively fast off-rate: prevents accumulation in ion channels and interfering with subsequent normal synaptic transmission. Neuroprotection with minimal adverse effects. Reported SE: ◦ occasional akathesia, ◦ rare slight dizziness at higher dosages. – At high doses: block 5-HT3 receptor-channels (? cognition) and nicotinic receptor channels (? glutamate release). Observed in cultures and animal models Example: Rat model of stroke, memantine brain damage by approximately 50%. Proving neuroprotection in humans Minimal adverse effects. Rare: dizziness, restlessness/ agitation (@ higher doses: 40– 60 mg/ day). Memantine work better for severe conditions. ◦ Neuropathic pain ◦ Alzheimer’s disease: FDA approval for moderateto-severe disease. Initial stage: disease progression + symptom improvement Later: NMDA receptors on functional neurones fully preserved ( moderate affinity antagonist). Zajaczkowski et al., 1997: in tonic activation of NMDA receptors, memantine can reverse deficits in synaptic plasticity, both at neuronal (LTP) and behavioural (learning) level Significant improvement in: cognitive processes, daily activities and self care (Ditzler, 1991; Görtelmeyer and Erbler, 1992; Winblad and Poritis, 1999). Agents such as memantine which mimic some of the features of the endogenous antagonist magnesium may be an optimal treatment combining both neuroprotective activity with symptomatological improvement. Memantine, an “un-competitive” NMDA antagonist. Rationale for use: excitotoxicity as a pathomechanism of neurodegenerative disorders. Memantine acts as a neuroprotective agent Promising for treatment of dementias, particularly Alzheimer’s disease. Combined with acetylcholinesterase inhibitors(mainstay of current symptomatic treatment of Alzheimer’s disease). Therapeutic potential in other CNS disorders: stroke, CNS trauma, Parkinson’s disease (PD), amyotrophic lateral sclerosis (ALS), epilepsy, drug dependence and chronic pain. Stuart A. Lipton. 2006. Paradigm shift in neuroprotection by NMDA receptor blockade: Memantine and beyond Nature Reviews Drug Discovery | AOP, 20. W. Danysz, C.G. Parsons, H-J Möbius, A.Stöffler and G.Quack. 2000. Neuroprotective and Symptomatological Action of Memantine Relevant for Alzheimer’s Disease – A Unified Glutamatergic Hypothesis on the Mechanism of Action. Neurotoxicity Research, Vol. 2. pp. 85-97.