Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Synaptogenesis wikipedia , lookup
Optogenetics wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Embodied language processing wikipedia , lookup
Microneurography wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Development of the nervous system wikipedia , lookup
Neuroregeneration wikipedia , lookup
Synaptic gating wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Central pattern generator wikipedia , lookup
Hypothalamus wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Proprioception wikipedia , lookup
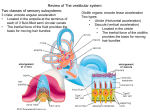
Neuroanatomy: Vestibular System (Pan) VESTIBULAR SYSTEM (GENERAL): Description: detects head motion and position and generates reflexes for maintaining head and body posture and balance and stabilizing the visual gaze; also provides us with a sense of movement and orientation in space General Properties: part of the somatosensory system that deals with unconscious proprioception o Has its own set of receptors: the vestibular apparatus (in the inner ear) o Has its own motor system that acts at the spinal cord and brainstem levels o Primarily acts as a reflex system; converts sensory information directly into motor activities under a strong influence from certain parts of the cerebellum o One of the systems that the cerebral cortex is NOT involved in Functions: o Helps orient us in 3-D space through integration with other systems (vision and conscious proprioception) o 3 major functions of the motor system: Maintain muscle tone in extensors via descending motor tracts (fight gravity) Maintain equilibrium via descending motor tracts Produce compensatory eye movements in response to head movements via ascending motor connections VESTIBULAR APPARATUS AND RECEPTORS: Description: non-auditory part of the inner ear; consists of 2 fluid-filled sacs (saccule and utricle) and 3 semicircular ducts o Inside bony structure is a membrane labyrinth filled with endolymph (high K+) o Space between membrane and bone is filled with perilymph (high Na+) Utricle and Saccule (Otolith Organ): Each have a macula (patch of sensory epithelium containing neuroepithelium hair cells) o Macula of the utricle: oriented horizontally o Macula of the saccule: oriented vertically Processes of the hair cells (kinocilia) are in contact with the overlying gelatinous mass, which contains otoliths (statoconia) The maculae are concerned primarily with static equilibrium and respond to changes in: o Gravitational forces o Linear acceleration Macular impulses convey information regarding position of the head in space (tilting of the head) o Hair cells stimulated by the otolithic particles- position of these particles vary under the influence of gravity Semicircular Ducts: Structure: o Connected to the utricle o Arranged at right angles to each other and represent 3 planes of space Horizontal/lateral (not completely horizontal; tilted ~30 degrees upward) Anterior Posterior o Each duct has a dilation at the end connected to the utricle called the ampulla o Crista ampullaris (composed of neuroepithelial hair cells) located in the ampulla, oriented transversely to the duct Covered by a gelatinous cupula Concerned primarily with kinetic equilibrium, and displacement of the endolymphatic fluid/movement of the cupula is caused by angular acceleration Movement of the cupula stimulates the hair cells Movement of the crista ampullaris toward the utricle= excitation Movement of the crista ampullaris away from the utricle= inhibition Function: o Corresponding ducts on opposite sides of the head function in pairs Horizontal ducts are in the same plane Anterior duct on one side is in the same plane as the posterior duct of the opposite side o Endolymphatic flow is greatest in the pair of ducts most nearly perpendicular to the axis of rotation VESTIBULAR NUCLEAR COMPLEX: Vestibular Nerve: Peripheral processes of Scarpa’s (vestibular) ganglion: to the hair cells Central processes of Scarpa’s (vestribular) ganglion: vestibular nerve (part of CNVIII); enters at the cerebellopontine angle to distribute to the vestibular nuclei and to the cerebellum Vestibular Nuclear Complex: Located at the boundary between the rostral medulla and caudal pons; lateral to the 4th ventricle Composed of 4 nuclei: superior, lateral (Deiter’s), medial and inferior (spinal) Vestibular nerve distributes to the nuclei in a differential fashion Vestibular Nerve Projections to the Vestibular Nuclear Complex: Projects to all four nuclei ipsilaterally o Projections from semicircular canals terminate more in the superior nucleus and the rostral portion of the medial nucleus o Projections from the utricle and saccule maculae terminate more in the lateral nucleus CEREBELLUM AND RECIPROCAL CONNECTIONS WITH VESTIBULAR NUCLEAR COMPLEX: Cerebellum: Vestibular portions of the cerebellar cortex: flocculus, nodulus and uvula (form the vestibulocerebellum) Fastigial nucleus: most medial of the deep cerebellar nuclei; also part of the cerebellum involved in vestibular activities Vestibular Nuclear Complex and Vestibular Nerve Project to the Cerebellum: VCN: projects ipsilaterally to vestibulocerebellum and fastigial nucleus Vestibular nerve: projects directly to the ipsilateral vestibulocerebellum (in the juxtarestiform body) but NOT to the fastigial nucleus Cerebellum Outputs to Vestibular Nuclear Complex (from 3 regions): 1. Vestibulocerebellum: sends ipsilateral input from the flocculus, nodulus and uvula to the VCN (inhibitory) 2. Spinocerebellum: sends ipsilateral input from the anterior vermis to the VCN (inhibitory) 3. Fastigial nucleus: sends bilateral input from deep cerebellar nucleus to the VCN; also receives inhibitory feedback from the vestibulocerebellum and anterior vermis All of these inputs travel in the juxtarestiform body (part of the ICP) Note: reticular formation also provides input into the VCN (excitatory) VESTIBULAR EFFERENTS: Spinal Cord: Lateral Vestibulospinal Tract (LVST): mainly from the lateral nucleus of the VCN to all levels of the ipsilateral spinal cord; runs in the anterior funiculus o Facilitates alpha motor neurons projecting to extensors and to gamma motor neurons regulating extensor muscle tone o Acts primarily on motoneurons in the medial/anterior parts of the ventral horn Axial muscles and proximal muscles of the extremeties; therefore, adjusts the contraction of muscles that oppose the force of gravity Medial Vestibulospinal Tract (MVST): arises from the caudal half of the VCN (especially medial nucleus); may have bilateral distribution in the caudal medulla but is mostly (if not entirely) ipsilateral in the spinal cord; terminates at T1-T2; also runs in the anterior funiculus o Distributes to cervical and upper thoracic segments (T1 and T2) o Primarily of importance for mediation of reflex head and neck movements in response to vestibular stimuli Eye Muscle Nuclei: Abducens, Trochlear and Oculomotor Main projection is from the rostral half of the VCN (mainly under control of semicircular canals) Projections are contralateral to the abducens nucleus and bilateral to the trochlear and oculomotor nuclei Major Effect: o Horizontal rotation of the head (ie. to the right) causes : Excitatory drive to the contralateral abducens nucleus (lateral rectus) Excitatory drive to the ipsilateral oculomotor nucleus (medial rectus) Other Fibers Arise from VCN and Project to the Following Areas: Reticular Formation: influence neurons in reticular formation, giving rise to the reticulospinal tracts; reticular formation also sends projections to the VCN (excitatory) Vestibular Periphery: cells lying between abducens nucleus and VCN project to the receptor cells in cristae and maculae (excitatory) Thalamus: project from VCN to the VPL bilaterally INTEGRATION: Maintains body position with respect to gravity. Accomplished by combining inputs from 3 major sensory sources: 1. Vestibular periphery- maculae of saccule and utricle 2. Proprioceptors from spinal levels- via cerebellum 3. Visual input- pathway unclear (probably via cerebellum and/or reticular formation) Reciprocal connections with reticular formation and cerebellum (vestibulocerebellum and spinocerebellum) to form feedback loops Descending pathways: mostly lateral vestibulospinal tract (LVST) Maintains direction of gaze during sudden angular acceleration. Vestibular Periphery: semicircular ducts signal angular acceleration Reciprocal connections with cerebellum (especially vestibulocerebellum) and perhaps reticular formation to form feedback loops Vestibular pathways to eye muscles: via MLF; give signals for compensatory rotation of eyes CLINICAL ASPECTS: Vestibular Disease: Clinical Signs: dizziness, vertigo, nausea, vomiting and abnormal nystagmus Nystagmus: involuntary rhythmic movements of the eye; consists of a slow movement in one direction followed by a rapid movement in the opposite direction (fast reset) o Named for the direction of its fast phase o Can be elicited on clinical examinations, but when it occurs spontaneously, it is a sign of a disease process (imbalance of synchronized impulses from vestibular sources) o Knock out VCN (ie. destroyed by a tumor) results in nystagmus towards the contralateral side Clinical Tests: Rotation Test: head tilted forward 30 degrees (horizontal canals parallel to the ground); rotated 10-12 times in the chair and then stopped o Normal: nystagmus occurs in the direction of the spin during rotation; occurs in the opposite direction when rotation abruptly stopped (post-rotary nystagmus) Carloric or Thermal Test: head tilted backward 60 degrees (horizontal canal in vertical plane); warm or cold water (7 degrees above or below body temperature) is infused into one ear to induce endolymphatic flow due to convection o Normal: warm water induces nystagmus to testing side; cold water to the opposite side