Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Drug discovery wikipedia , lookup
Toxicodynamics wikipedia , lookup
NMDA receptor wikipedia , lookup
Psychedelic therapy wikipedia , lookup
Specialty drugs in the United States wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Serotonin syndrome wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Atypical antipsychotic wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Polysubstance dependence wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Orphan drug wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Pharmacognosy wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropharmacology wikipedia , lookup
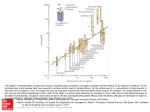
神经系统药理3 1、抗癫痫药 2、抗帕金森病药及抗老年性痴呆药 3、抗精神病药和抗抑郁药 4、局部麻醉药 张纬萍 [email protected] 药理学系 2014.10.13 Antiepileptic and Anticonvulsant Drugs 抗癫痫及抗惊厥药 Local excitatory Abnormal high frequency discharging 发病率高; Abnormal spreading 突发性,不可预测; 不可根治,需终身服药 Brain malfunction Accompanied with abnormal EEG Classification of epilepsy International Classification of Epileptic Seizures: Partial Onset Seizures(局限性发作) Simple Partial(单纯局限性) Complex Partial (复合性局 • Partial seizures with dyscognitive features Partial Seizures with secondary generalization • Partial seizures without dyscognitive features 限性) (局限性发作继发全身强直阵挛性发 作) International Classification of Epileptic Seizures: Primary Generalized Seizures Absence (Petit Mal) (失神性发作/小发作) Myoclonic (肌阵挛性发作) Generalized Tonic+Clonic (全身强直阵挛性发作) http://www.uwo.ca/cns/resident/pocketbook/pictures/3-hz-s-w.jpg The pathways for seizure propagation in partial seizures and primary generalized seizures Origin of a surface epileptic discharge 强直性发作 表面脑电图 阵挛性发作 发作后抑制 细胞外记录 细胞内记录 PDS:paroxysmal depolarization shift 阵发性去极化漂移 Seizures are generated by groups of neurons which depolarizing synchronously Epileptic neurons generate Paroxysmal Depolarizing Shift (阵发性去极化飘移, PDS) During a PDS, there is the repetitive activation of key ion channels. These ion channels represent opportunities to prevent or terminate seizures. Surface Spike PDS Sodium Influx Calcium Influx Chloride Influx K efflux Mechanisms of antiepileptic drugs Electrophysiological Inhibiting excessive discharges Inhibiting spread of discharges Molecular Potentiating GABA neuronal functions Inhibiting excitatory neuronal functions Modulating Na+, Ca2+, K+, Cl- channel fuctions 兴奋性 Molecular targets for anti-seizure drugs at the excitatory, glutamatergic synapse. 抑制性 Molecular targets for antiseizure drugs at the inhibitory, GABAergic synapse. Imbalance of excitation and inhibitory Na+、Ca2+、NMDA 、K+ 、Cl-、GABA Antiepileptic drugs Focus formation and epileptic attack Focus shift Spreading Refractory epilepsy A. Antiepileptic drugs Phenytoin Sodium 苯妥英钠, 大仑丁 1. Pharmacological effects and the mechanism (1) Effects — Inhibiting spread of abnormal discharges — Not on the happening of abnormal discharge 苯妥英钠 A. Antiepileptic drugs 1. Pharmacological effects and the mechanism (2) Mechanism — Blocking Na+ channel in inactive state — Inhibiting L- and N-type Ca2+ channel (but not T-type Ca2+ channel,失神发作无效) — Calmodulin kinase activity Neurotransmitter release (NE, 5-HT, DA etc.) — Block post-tetanic potentiation (PTP) formation A. Antiepileptic drugs 2. Clinical uses (1) Anti-epilepsy Grand mal, status epilepticus; Partial seizures (simple and complex); Ineffective for petit mal (absence seizures) 失神小发作 (2) Trigeminal (三叉神经疼) and related neuralgia (神经疼) (3) Anti-arrhythmia A. Antiepileptic drugs 3. ADME Larger doses: non-linear kinetics(> 10 g/ml) Half life = 24 hours Therapeutic range = 10-20 ug/ml Levels above 20 cause ataxia (共济失调) and nystagmus(眼球震颤) Hepatic metabolism CYP3A enzyme pathway CYP3A antagonists will raise phenytoin levels Necessary to monitor plasma concentrations Initially linear Psuedo first order A. Antiepileptic drugs 4. Adverse effects (1) Local reactions GI reactions; gingival hyperplasia (2) CNS reactions Particularly in the cerebellum and vestibular systems: nystagmus (眼球震颤), ataxia (共济失调), etc. Behavioral changes: confusion, hallucination, coma (3) Hemological reactions Megaloblastic anemia (affect the metabolism of folic acid) A. Antiepileptic drugs (4) Allergic reactions Skin reactions; blood cell abnormality (including thrombocytopenia, agranulocytosis); hepatic toxicity; ect. (5) Skeletal reactions Osteomalacia (骨质疏松) by increase vitamin D metabolism and calcium absorption (inducer) (6) Others Birth defects, hirsutism(多毛), etc A. Antiepileptic drugs 5. Drug interactions(蛋白结合、代谢) (1) Increases plasma concentrations of drugs by displacement of plasma protein binding (salicylates) (2) Drug metabolizing enzyme inhibitor decrease the metabolism of phenytoin (isoniazid异烟肼, chloramphenicol氯霉素) (3) Drug metabolizing enzyme inducer increase the metabolism of phenytoin (phenobarbital, carbamazepine) (4) Phenytoin enhances the metabolism of corticosteroids and vitamin D A. Antiepileptic drugs Phenobarbital NH O CO C C2H5 C NH 苯巴比妥 CO C6H5 Sedative and hypnotic effect Inhibiting both formation and spread of discharges. Postsynaptic Cl- influx Presynaptic Ca2+ influx neurotransmitter release (NE, ACh, Glu, etc.) Effective for grand mal , status epilepticus, partial simple seizures. A. Antiepileptic drugs Drugs acting at the chloride channel Benzodiazepines 苯二氮卓类 Binds to specific receptors Phenobarbital 苯巴比妥 Binds to barbiturate specific receptor Valproate 丙戊酸钠 Decreases GABA degradation in presynaptic terminal A. Antiepileptic drugs Ethosuximide 乙琥胺 Block T-type Ca2+ channel Block Na+-K+-ATPase Inhibit cerebral metabolism and GABA transaminase Effective for peptit mal(小发作) Combined with phenobarbital A. Antiepileptic drugs Valproate sodium 丙戊酸钠 Broad spectrum Inhibiting spread of discharges but not formation Increases GABA levels via inhibiting GABA transaminase, GABA transport, Glutamate decarboxylase Inhibit Na+ and L-type Ca2+ Enhance K+ ? GI side effects Tremor Hepatitis Pancreatitis Serious neural tube and cardiac defects in fetus in 1% A. Antiepileptic drugs Carbamazepine Blocks Na+ and Ca2+ channels Enhance GABA Effective against psychomotor seizures, and grand mal Effective for mania, depression, and neuralgia Like phenytoin, metabolized by CYP3A pathway (an inducer) Need titration up! 卡马西平 N CONH 2 Safety and Toxicity Dose dependence-double vision, ataxia(共济失调) rash 5-10% rare marrow suppression rare hepatitis frequent hyponatremia/Water intoxication (Dose dependence) fetal malformations A. Antiepileptic drugs Other antiepileptic drugs(略) Primidone 扑米酮:analogues of phenobarbital, used for phenobarbital- and phenytoin-ineffective patients Mephenytoin 美芬妥英, Ethotoin 乙苯妥英: analogues of phenytoin Diazepam 地西泮: status epilepticus (i.v.) Nitrozepam 硝西泮, Clonazepam 氯硝西泮:peptit mal Lamotrigine 拉莫三嗪 A. Antiepileptic drugs Other antiepileptic drugs(略) Oxarbazepine(奥卡西平):similar as carbamazepine but weaker Antiepilepsirine(抗痫灵): broad spectrum, esp. grand mal Lamotrigine 拉莫三嗪: Na+ channel antagonist. Effective against both partial and generalized epilepsy Flunarizine 氟桂利嗪: Inhibit L- and T-type Ca2+ channel. broad spectrum Topiramate托吡酯: Blocks AMPA+kainate receptors Also blocks Na+ and Ca2+ channels 卡马西平 苯妥英钠 拉莫三嗪 丙戊酸钠 丙戊酸钠 二甲双酮 乙琥胺 丙戊酸钠 苯二氮卓类 巴比妥类 A. Antiepileptic drugs Common toxicity of antiepileptic drugs: CNS reactions Hemological reactions Hepatic toxicity Teratogenicity(致畸) Teratogenicity All AED's cause fetal malformations in at least 6% of infants. Highest risk with phenytoin, valproate, phenobarbital, and carbamazepine (Class D drugs) Folate supplementation prevents neural tube defects. A. Antiepileptic drugs Principals of antiepileptic drug uses 1. Choice of drugs (1) Grand mal / Partial: Phenytoin, Carbamazepine, Phenobarbital Primidone, Valproate sodium (2) Peptit mal: Ethosuximide Clonazepam, Valproate sodium (3) Psychomotor:Carbamazepine, Phenytoin (4) Status epilepticus:Diazepan (i.v.) Phenytoin (i.v.), Phenobrbital (i.m.) A. Antiepileptic drugs 2. Dosage: small larger doses, titration up; dose individualization; plasma concentration monitoring if necessary 3. Usage: drug combination 4. Withdrawal:gradually and slowly B. Anticonvulsant drugs Magnesium Sulfate 硫酸镁 1. Effects:central depression; vasodilatation, BP ; relaxing skeletal muscles 2. Uses:convulsion;hypertension crisis 3. Adverse effects: depression of respiratory and vasomotor centers, antagonized by calcium preparations (i.v.) B. Anticonvulsant drugs Other anticovulsant drugs Sedative-hypnotic drugs Drugs which primarily affect K+ channel Levetiracetam 左乙拉西坦 Few side effects except: High Potency->75% reduction in seizures in over 20% of refractory patients Fatigue Depression and Psychosis leading to discontinuation in 7%. White et al Neurology 2003 Drugs which affect Kainate and AMPA receptors Topiramate Mechanism -Multiple Blocks AMPA+kainate receptors Also blocks sodium and CA channels Potentiate GABA transmission Effective against both partial and generalized epilepsy Excreted primarily in urine Start at 25 mg/day…titrate to 300-500/day Behavioral /Cognitive problems common Low risk of rash Causes weight loss Relatively safe, Class C in pregnancy High Potency > 75% reductions in over 20% of refractory patients Zonisamide Anti-epileptics (AEDs) Note: All of the following drugs have multiple mechanisms of action (primary mechanisms include blockade of voltage gated Na+ channels, enhancement of GABAergic neurotransmission, and inhibition of glutamatergic neurotransmission) Older AED’s phenytoin voltage gated Na+ channel blocker inhibition is use-dependent; limits ability of neurons to fire at high frequency. . maintains Na+ channel in inactivated state and slows rate of recovery; no change in spontaneous activity or firing at slow rate) carbamazepine voltage gated Na+ channel blocker valproate/valproic acid GABA metabolism inhibitor phenobarbital allosteric GABA A agonist Newer AED’s oxcarbazepine voltage gated Na+ channel blocker lamotrigine voltage gated Na+ channel blocker topiramate glutamate receptor antagonist; voltage gated Na+ channel blocker levetiracetam multiple actions gabapentin Ca2+ channel blocker zonisamide glutamate receptor antagonist; Na+ and T-type Ca+2+ channel blocker lorazepam (I.V.) for status epilepticus allosteric GABA A agonist Anti-Epileptic Drug’s Effective as Monotherapy (Single Agent) Partial (Localization Related) Generalized Older AED’s Phenytoin (苯妥英钠) Carbamazepine (卡马西平) Valproate (丙戊酸钠) Newer AED’s Oxcarbazepine (奥卡西平) Lamotrigine(拉莫三嗪) Topiramate(托吡酯) French et al Neurology 2004 Bold= new generation AED Valproate (丙戊酸钠) Topiramate(托吡酯) (GTC and absence) (GTC) Lamotrigine (拉莫三嗪) (absence) French et al Neurology 2004 New AED’s effective as adjunctive treatment for refractory epilepsy Partial Topiramate Levetiracetam Pregabalin Zonisamide Oxcarbazepine Lamotrigine Gabapentin Tiagabine Above all have level I, randomized clinical trials, or A or B evidence, AAN guidelines 2004 Generalized Topiramate Levetiracetam Lamotrigine Data from randomized placebo controlled trials Drugs in red are generally considered high potency Increased expression of ABC transport in epilepsy Transporters 抗癫痫药敏感大鼠 Control 耐药癫痫大鼠 耐药癫痫大鼠P-gp表达增加 抗癫痫药耐药大鼠 P-gp基因敲除及其抑制剂增加脑内抗癫痫药浓度 P-gp抑制剂增强抗癫痫药Oxarbazepine(OXC, 奥卡 西平)作用及延长癫痫病人入院间隔时间 Contribution of CYPs to drug metabolism CYP Enzymes 底物 抑制剂 诱导剂 (from Guengerich 2003) AEDs and Hepatic CYP450 Interactions Induction – increase in amount of enzyme protein, resulting in an increase in the rate of metabolism of the affected drug Inhibition – competition at the enzyme site that results in a decrease in metabolism of the affected drug Valproic acid CYP2C inhibitor (inhibits phenobarbital, phenytoin metabolism) Phenytoin CYP inducer (3A4 and 2C); metabolized by 2C9 Carbamazepine CYP inducer (CYP inducer (3A4 and 2C); metabolized by 3A4. . . induces its own metabolism Phenobarbital CYP inducer (3A4 and 2C) Drugs Treating Parkinson Disease and Alzheimer Disease Parkinson’s disease (PD) Rigidity Tremor Bradykinesia Postural instability (propulsion, retropulsion). Tremor: one of the common symptoms of PD 黑质-纹状体通路 结节-漏斗通路 中脑-边缘/皮层通路 Substantia nigro striatum dopaminergic pathway is involved in PD pathogenesis Parkinson disease Normal Dopaminergic neuron degeneration in substantia nigro and striatum Normal (-) Parkinson disease relatively potentiated injured (-) Abnormal balance of DA/ACh neuronal functions in extrapyramidal system of Parkinson disease Acetylcholine Muscarinic antagonists Levodopa Dopamine Treatment I: Increase dopamine Tyrosine TH DOPA DA receptors Dopamine Decarboxylase MAO-B Dopamine metabolisms DBH Norepinephrine MAO-A metabolisms What is the desired goal of pharmacological therapies for Parkinson’s disease? Different approaches include: I. increases in dopamine synthesis capacity II. direct activation of post-synaptic receptors III. inhibition of dopamine metabolism IV. alteration of the interaction/balance with other neurotransmitters V. dopamine releasers VI. L-DOPA metabolism inhibitors Note: All therapies treat the symptoms of the disease; none are neuroprotective and none slow the progression of the disease Drugs for treatment of Parkinson disease Levodopa and related drugs OH OH OH Rationale for L-Dopa Precursor Loading: OH L-DOPA decarboxylase B6 O NH2 OH L-Dopa (左旋多巴) NH2 Dopamine (多巴胺) • Striatal dopamine levels are low in PD. • Dopamine does not pass BBB, has no therapeutic effect in PD. • L-Dopa, an amino acid, the immediate precursor to dopamine, is transported across BBB and is an effective drug for PD. Carbidopa (卡比多巴) The combination of L-DOPA & carbidopa, is called Sinemet™. (L-DOPA t1/2 ~ 1.5 h) BBB Periphery 3-O-methylDOPA CNS L-DOPA COMT L-DOPA AAAD OH OH CH3 Pyridoxal 5phosphate dopamine AAAD dopamine NH NH2 HO O Carbidopa MAO Levodopa alone Levodopa + Carbidopa Drugs for treatment of Parkinson disease Levodopa 1. ADME Penetrating into the brain, transformed to DA or NE (less) Distributed in peripheral tissue (most) 2. Effects and uses Parkinson disease: decreases the rigidity, tremors, and other symptoms Drugs for treatment of Parkinson disease Levodopa 3. Adverse effects Early: (1)GI: nausea, vomiting, etc. (2)CVS: hypotension, arrhythmia, etc. (3)CNS: emotional depression/ psychosis; abnormal involuntary; hallucinations; etc. Late : (1) fluctuation of response: end of dose/“wearing off” periods; on/off periods (sudden loss of symptom control, akinesia) . (2) dyskinesia (运动障碍,after years of chronic L-DOPA, up to 80%, Involuntary movements: chorea(舞蹈症), ballismus(投掷症), athetosis(手足徐动症), dystonia(肌张力失 常), myoclonus(肌阵挛), and tremor 一般情况下,对L-dopa制剂的反应可分为3个阶段: ①良好反应阶段(2~5年),为用药的最初阶段,每6~8小时 或更长时间服药1次,可使全部症状得到平稳的缓解或改善。 ②中间反应阶段(2~3年),此阶段中每次服药仅可引起短时 间的症状改善,每个剂量的后期与下一个剂量前,有1个药物 无作用期,称为剂末现象,此外,还可出现开关现象和反常性 运动不能;这种疗效下降与黑质DA能神经元逐渐衰退,DA合 成、贮存进一步下降,及DA受体反应能力降低有关。 ③反应衰退阶段,对L-dopa制剂反应明显下降或根本不起反应; 运动困难与致残程度更为严重;同时治疗中的一些不良反应更 为明显。 Drugs for treatment of Parkinson disease Other drugs 1. DA receptor agonists 1st generation agonists: (ergot derivatives, 麦角衍生物) bromocriptine* (溴隐亭, D2 agonist) (t1/2 ~ 12 h) pergolide* (培高利特, D2/D3 agonist)(t1/2 ~ 24 h) 2nd generation agonists: ropinirole (t1/2 ~ 6 h) (普拉克索, D2/D3 agonist) pramipexole (t1/2 ~ 8 -12 h) (罗平尼咯, D2 agonist) Can be used as monotherapy for mild parkinsonism, or combined with levodopa for advanced disease, permitting the dose of levodopa to be reduced and smoothing out response fluctuations. the major adverse effects of DA receptor agonists • Lower incidence of dyskinesia and response fluctuation • Some individuals develop a troubling sleep disorder, with sudden attacks of sleep (突然昏睡) during ordinary daytime activities • Postural hypotension • Dose-related psychiatric side effects (similar to L-DOPA but may occur more frequently, especially in elderly) • Nausea or vomiting (drugs active at chemotrigger zone (CTZ) ) Drugs for treatment of Parkinson disease 2. MAO-B inhibitors ( Peripheral metabolism of catecholamines (mostly MAO-A) is unaffected.) decreasing DA metabolism in the CNS Selegiline Rasagiline 司来吉兰 雷沙吉兰 3. COMT inhibitors (decreasing DA metabolism) CNS COMT inhibitor: :itecapone 硝替卡朋 peripheral COMT inhibitor: entacapone恩他卡朋 Drugs for treatment of Parkinson disease 4. Amantadine 金刚烷胺 Used for mild Parkinson’s disease, as an early monotherapy Mechanisms of action may include: release of dopamine, block DA reuptake, actions on glutamate receptors (as an NMDA-receptor antagonist) The dose should be reduced with renal impairment. Potential adverse effects: - CNS reactions (dizziness, anxiety, impaired coordination) - hyperkinesias(运动亢进) - nausea, vomiting - others Drugs for treatment of Parkinson disease Muscarinic antagonists Trihexyphenidyl (苯海索,artane, 安坦) Benzatropine (苯扎托品) Decreasing CNS cholinergic functions Adjuvant of Parkison disease treatment DRUG THERAPY - Summary • Main Line Agents: • L-DOPA plus carbidopa (Sinemet®) • Dopamine receptor agonists (ropinirole) • Lower Efficacy/Second Line or Adjuvant Agents: • Anticholinergics • Reuptake Inhibitor or releaser (amantadine) • COMT Inhibitor (entacapone) • MAO B Inhibitors (rasagiline, selegiline) Drug-Induced Parkinsonism • Reserpine, which depletes brain catecholamines, induces Parkinson’s disease symptoms • Antipsychotics (neuroleptics), that block DA receptors, ie, dopamine receptor antagonists. • N-methyl-4-phenyl-l,2,3,6-tetrahydropyridine (MPTP). MPTP first came to medical attention because it produced symptoms similar to Parkinson’s disease. 3、Drugs for treatment of dementia (Alzheimer and related diseases) Anticholinesterase drugs Cholinoceptor agonists Neurotrophic factor-like drugs Pathological characteristics of AD Atrophy of the brain Senile plaques Neurofibrillary tangles Pathophysiologic Hypothesis of AD Glutamate -Amyloid Excitotoxicity Neurofibrillary Tangles Other Factors Cell Damage/ Loss (ACh deficit) Dementia Inflammation Mitochondrial Dysfunction Normal Cholinergic Function Presynaptic neuron Glial cell Acetyl CoA + Choline Choline BuChE ChAT MR ACh NR BuChE Synaptic cleft ACh AChE Postsynaptic neuron Acetate MR NR ACh = acetylcholine; AChE = acetylcholinesterase; BuChE = butyrylcholinesterase; ChAT = choline acetyltransferase; CoA = coenzyme A; MR = muscarinic receptor; NR = nicotinic receptor. Adapted from Adem, 1992. Choline + AChE ACh Drugs for treatment of dementia Anticholinesterase drugs Tarcrine 他克林: Easy to pass BBB; Decrease AChE 70%; activate M and N receptors (especially M receptor); Enhance the release of ACh (throught M receptor). Induce hepatic toxicity. Galantamine 加兰他敏: similar to tarcrine, except without hepatic toxicity and high specific to neuron AChE. Huperzine 哈伯因(石杉碱甲): a high selective AChE inhibitor; improve memory and recognization. Metrifonate 美曲磷脂: the first AChE inhibitor; Increase central DA and NE; Decrease the red blood cell AChE 52%. Drugs for treatment of dementia Cholinoceptor agonists Xanomeline 占诺美林: selective to M1 receptor; high concentration in cortex and striatum; Has GI and CVS side effects. Sabcomedine hydrochloride: selective to M1 receptor; safe. Neurotrophic factor enhancer AIT 082: increase the release of neurotrophins in injured neurons ALCAR(盐酸乙酰L肉碱): protect synapse and increase nurotrophins Propentofylline 丙戊茶碱: inhibit adrenaline reuptake and cAMP metabolize; neuroprotective effects; Pathophysiologic Hypothesis of AD Glutamate -Amyloid Future treatment •K+channel blocker •Glutamate receptor regulator •5-HT receptor blocker Excitotoxicity Cell Damage/ Loss (ACh deficit) Neurofibrillary Tangles Other Factors Inflammation Dementia Mitochondrial Dysfunction 4、抗精神病药和抗抑郁药 Antidepressant and antimanic drugs 抗抑郁和抗躁狂药 Anxiolytics / antianxietics 抗焦虑药 Antipsychotic drugs 抗精神分裂药 Disorders of Mood Disorders of mood (affective disorders 情感障碍) are extremely common in medical practice. The severity of these conditions covers an extraordinarily broad range, from normal grief(悲伤) reactions and dysthymia(心境恶劣) to severe, incapacitating illness that may result in death. Emotion(情绪)refers to transient responses to environmental, internal, and cognitive stimuli, while mood (心境)refers to the predominant emotional state over time. Disorders of Mood The symptoms of depression are intense feelings of sadness, hopelessness, despair, and inability to experience pleasure in usual activity. Mania is characterized by the opposite behavior, that is, enthusiasm, rapid thought and speech patterns, and extreme self-confidence and impaired judgment. Anxiety, a state characterized by arousal, vigilance, physiologic preparedness, and negative subjective states, may share certain critical circuits with fear. Monoamine hypothesis of Depression (单胺假说) 5-HT — genetic basis of depression & mania NE — depression NE — mania Modulation of monoamines in the synaptic space and/or the related post-synaptic receptors is of therapeutic importance Long-term adaptations to antidepressant treatment 支持 不支持 Classes of Antidepressants Tricyclic Antidepressants (TCAs) Monoamine Oxidase Inhibitors (MAOIs) Norepinephrine Reuptake Inhibitors (NARIs) Selective Serotonin Reuptake Inhibitors (SSRIs) Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs) Noradrenergic and specific serotonergic antidepressants (NaSSAs) Model of the neurotrophic hypothesis of antidepressant treatments and stress-related disorders A. Antidepressant Drugs Tricyclic Antidepressants (TCAs) Imipramine 丙米嗪(米帕明) Tricyclic structure N CH 3 CH 2CH 2CH 2N CH 3 临床应用 阿米替林 氯丙咪嗪 多塞平 丙咪嗪 副作用 Imipramine 丙米嗪(米帕明) 1. Pharmacological effects (1) Central effects Inhibiting reuptake of monoamine transmitters Improving patient’s mood after 2 weeks Sedative effects in normal subjects (antihistaminergic or a-adrenergic blocking properties) (2) Autonomic effects Muscarinic blocking effects (3) Cardiovascular effects Hypotension, tachycardia, arrhythmia Imipramine 丙米嗪(米帕明) 2. Clinical uses (1) Depression Endogenous, melancholic, etc. (2) Enuresis (遗尿) (3) Anxiety (焦虑) and panic disorder (惊恐症) Imipramine 丙米嗪(米帕明) 3. Adverse effects (1) Antimuscarinic effects dry mouth, constipation(便秘), intraocular pressure increase, blurred vision, urinary retention, etc. Contraindicated in prostatauxe and glaucoma (2) CNS reactions Confusion or delirium(谵妄), depression-mania (bipolar patients) (3) CVS reactions Postural hypotension, sinus tachycardia, potential of arrhythmia Imipramine 丙米嗪(米帕明) 4. Drug interactions (1) Plasma protein binding displacement by phenytoin, aspirin, scopolamine(东莨菪碱), phenothiazines (吩噻嗪类), etc. (2) MAO inhibitors potentiating the effects of TCA, contraindicated for combination with MAOIs (3) Potentiating the effects of CNS depressant drugs Interaction of TCA with other types of drugs A. Antidepressant Drugs Monoamine oxidase inhibitors (MAOIs) Selective for central MAO-B, less selective for enteric MAO-A; Used in treatments of depression (non-sensitive to TCAs) and Parkinson disease phenelzine (苯乙肼): non-selective selegiline (司来吉兰): also used in Parkinson disease •MAOIs and Dietary Interactions Tyramine(酪胺) is normally metabolized by MAO Tyramine is sympathomimetic (it acutely displaces NE from terminals to activate receptors) Ingesting tyramine during MAO inhibition results in hypertension, headache, palpitations, nausea, vomiting Tyramine is present in a number of foodstuffs, such as aged cheese, red wine, etc. A. Antidepressant Drugs NE reuptake inhibitors (NRIs) Selective norepinephrine reuptake inhibits rapid actions weaker sedative, anticholinergic and hypotensive effects desipramine (地昔帕明) maprotiline (马普替林) nortriptyline (去甲替林) protriptylin (普罗替林) amoxapine (阿莫沙平) A. Antidepressant Drugs Selective 5-HT reuptake inhibitors Selective serotonin reuptake inhibits (SSRIs) weaker sedative effects with anti-anxiety effects fluoxetine (氟西汀,百忧解):抑郁症、神经性贪食症 paroxetine (帕罗西汀) sertraline (舍曲林) A. Antidepressant Drugs 5-HT/NE reuptake inhibitors Mixed serotonin/norepinephrine reuptake inhibits (SNRIs) rapid action less affinity with receptors higher safety venlafaxine (文拉法辛) milnacipram (米那普仑) lofepramine (洛夫帕明) A. Antidepressant Drugs Noradrenergic and specific serotonergic antidepressant (NaSSA) mirtezapine (米氮平) blocking presynaptic (auto- or hetero-) a2 receptor on both norepinephrine and serotonin (5-HT) pre-synaptic axons - increasing NE and 5-HT release; stimulating postsynaptic a1 receptors on serotonergic cell bodies - increasing the firing rate of serotonergic neurons potently blocking postsynaptic 5-HT2A, 5-HT2C and 5-HT3 receptors – attenuating 5-HT2C-mediated anxiety The net outcome of these effects is: increased noradrenergic activity increased serotonergic activity, esp. 5-HT1A receptors B. Antimanic Drugs Lithium carbonate Carbamazepine Chlorpromazine Other related antiepileptic and antipsychotic drugs B. Antimanic Drugs Lithium carbonate 碳酸锂 1. Pharmacological effects and clinical uses Mood-stabilizing agent (1) Inhibiting NE and DA release (2) Interfering phosphatidylinositol (PI) metabolism (3) Substitute for sodium in generating action potentials and in Na+-K+ exchange across the membrane. B. Antimanic Drugs 2. Adverse effects Related to the serum concentration of Li+ 0.8 – 1.5 mmol/L: therapeutic level 1.6 – 2.0 mmol/L: GI reactions > 2.0 mmol/L: CNS toxicity Monitoring serum concentration of Li+ if possible B. Antimanic Drugs (1) Side effects Nausea, vomiting, abdominal pain, diarrhea, sedation, finger tremor, polyuria, etc. (2) Acute intoxication Mental confusion, coma, hyperreflexia(反射亢进), gross tremor, dysarthria(构音困难), seizures, etc. (3) Others Benign thyroid enlargement, renal damage C. Anxiolytic drugs 1. Benzodiazepines see details in Sedative-Hypnotic Drugs 2. Buspirone(丁螺环酮) 5-HT1A receptor selective partial agonist, lowering 5-HT release Fewer sedative, hypnotic, memory-deficient effects No cross tolerance to benzodiazepines, and less potential of dependence Schizophrenia(精神分裂症) • Neurological Disorder - impairs ability to perceive, understand & interpret the environment • Impaired social and occupational function • Behavioral Syndrome – predictable or not • Etiology and biology remain unclear- familial tendency, DA and other neurotransmitters • History – early dementia, unremitting bad course Signs & Symptoms Positive symptoms • Delusions (妄想) - fixed false belief outside cultural norm (bizarre vs. non bizarre) • Hallucinations (幻觉) - perceptual (hearing), have no outside source • “Like my voice” • Not an illusion (a mistaken perception for which there is an actual external stimulus) • Disorganization (思维紊乱) - pattern of speech or behavior, making up words without a meaning (neologisms) Signs & Symptoms Negative symptoms • • • • • • Affective flattening Avolition / Amotivation (decreased motivation) Autistic(孤独) behaviors (social withdrawal ) Anhedonia (inability to experience pleasure ) Ambivalence (coexistence of opposing attitudes or feelings,矛盾心态) Anosognosia (疾病感缺失) (impaired awareness of illness ) D. Antipsychotic drugs Classified according to chemical structures 1. Phenothiazines(吩噻嗪类) Chlorpromazine 氯丙嗪 perphenazine 奋乃静; fluphenazine 氟奋乃静 trifluoperazine 三氟拉嗪;thioridazine 硫利达嗪 • Typical 2. Thioxanthenes (硫杂蒽类) Chlorprothixene 氯普噻吨(泰尔登) 3. Butyrophenones(丁酰苯类) Haloperidol 氟哌啶醇 Droperidol 氟哌利多(氟哌啶) Typical antipsychotic drugs are dopamine D2 receptor antagonists Others Penfluridol Sulpride 五氟利多 舒必利 Longer duration of action, taking once weekly selectively acts on mesolimbic D2 receptors few extrapyramidal reactions Clozapine Risperidone 氯氮平 Blocking D4 and 5-HT receptors 利培酮 Blocking D2 and 5-HT2 receptors • Atypical Actions of some secondary generation drugs D. Antipsychotic drugs High potency Low potency 普马嗪 氟哌利多 三氟哌啶醇 苯哌利多 螺环哌啶酮 D. Antipsychotic drugs • The dopamine hypothesis of schizophrenia • The serotonin hypothesis of schizophrenia • The glutamate hypothesis of schizophrenia D. Antipsychotic drugs Phenothiazines(吩噻嗪类) Chlorpromazine 氯丙嗪 S N (CH 2)3 Cl N(CH3)2 D. Antipsychotic drugs 1. Pharmacological effects (1)Central effects:Blocking central D2 dopamine receptors a) Antipsychotic effects (neuroleptic effects) for treatment of schizophrenia controlling excitation and then hallucinations (weeks to months) b) Antiemetic effects(镇吐作用) inhibiting chemoreceptor trigger zone (CTZ) dopaminergic function c) Poikilothermic effects (体温调节作用) hypothermic anesthesia artificial hibernation (人工冬眠) d) Extrapyramidal effects primary adverse effects e) Potentiating the effects of central depressants sedative-hypnotics, analgesics, general anesthetics, ethanol D. Antipsychotic drugs (2) Autonomic nervous system effects a) Hypotensive effects a receptor blockade, postural hypotension b) Anticholinergic effects dry mouth, constipation, blurred vision, urinary retention, etc. (3) Endocrine effects prolactin ACTH, growth hormone D. Antipsychotic drugs 2. Clinical uses (1) Treatment of schizophrenia (2) Treatments of emesis and hiccough used for emesis (止吐) and hiccough(呃逆) but ineffective on motion sickness (3) Hypothermic anesthesia (combined with lowering room temperature) and artificial hibernation (combined with Pethidine 哌替啶 and promethazine异丙嗪) D. Antipsychotic drugs 3. Adverse effects (1) Side effects Central depression Peripheral effects: postural hypotension, dry mouth, and other effects resulting from muscarinic and a receptor blockade D. Antipsychotic drugs (2) Extrapyramidal effects Due to DA receptor block: a) Parkinsonism b) Akathisia (静坐不能) c) Acute dystonia (急性肌张力障碍) attenuated by central muscarinic antagonists Due to supersensitive to DA: Tardive dyskinesia (迟发性运动障碍) D. Antipsychotic drugs (3) Other central reactions neuroleptic maglinant syndrome (神经阻滞药恶 性综合征) psychotic reactions (药源性精神异常) epilepsy and convulsion: lowering seizure threshold (4) Allergic and hemological reactions skin reactions, leukopenia, obstructive jaundice, liver damage D. Antipsychotic drugs (5) CVS reactions arrhythmia hypotension: treated by a receptor agonists sudden death (elderly with CVS diseases) (6) Endocrine reactions hyperplasia of mammary glands (乳腺增生), galactorrhea (溢乳), amenorrhea (闭经 ), child growth retard(生长抑制) D. Antipsychotic drugs (6) Acute intoxication severe CNS depression, coma, severe hypotension (7) Contraindications epilepsy coma elderly with CVS disorders severe hepatic and renal dysfunction D. Antipsychotic drugs Other phenothiazines perphenazine 奋乃静 fluphenazine 氟奋乃静 trifluoperazine 三氟拉嗪 thioridazine 硫利达嗪 more potent therapeutic effects and extrapyramidal effects D. Antipsychotic drugs Thioxanthenes (硫杂蒽类) Chlorprothixene 氯普噻吨(泰尔登) Used for the patients with symptoms of depression and anxiety D. Antipsychotic drugs Butyrophenones(丁酰苯类) Haloperidol 氟哌啶醇 Droperidol 氟哌利多(氟哌啶) Combined with fentanyl: neuroleptanalgesia(神经 安定 [镇痛] 麻醉术) D. Antipsychotic drugs Others Penfluridol 五氟利多 Longer duration of action, taking once weekly Sulpride 舒必利 selectively acts on mesolimbic D2 receptors few extrapyramidal reactions Clozapine 氯氮平 Blocking D4 and 5-HT receptors Risperidone 利培酮 Blocking D2 and 5-HT2 receptors 局部麻醉药 Local Anesthetics (LAs) Definition: drugs that cause loss of sensation without loss of consciousness Reversibly block nerve conduction Act on every type of nerve fiber Also act on cardiac muscle, skeletal muscle and the brain No structural damage to the nerve cell Structural Classes: Esters (酯类) and Amides(酰胺类) 胺基团 all are weak bases BH+ B + H+ 可卡因 普鲁卡因 丁卡因 苯佐卡因 芳香族环 酯链 芳香族环 利多卡因 甲哌卡因 布比卡因 布比卡因 丙胺卡因 酰胺链 胺基团 神经纤维末梢、神经节、中枢 神经系统的突触较为敏感; 细的比粗的神经纤维敏感; 有髓鞘的比无髓鞘的敏感; 钝痛比锐痛敏感; Use-dependent Blockade Actions of LAs Ionic gradient and resting membrane potential are unchanged Decrease the amplitude of the action potential Slow the rate of depolarization Increase the firing threshold Slow impulse conduction Prolong the refractory period CNS Toxicity Correlation between potency and seizure threshold Bupivacaine • 2 ug/ml Lidocaine • 10 ug/ml Cardiovascular Toxicity Attributable to their direct effect on cardiac muscle Contractility Negative inotropic effect that is dose-related and correlates with potency Interference with calcium signaling mechanisms Automaticity Negative chronotropic effect Rhythmicity and Conductivity Ventricular arrhythmias Pharmacokinetics Absorption (injected or topical) - affected by vascularity (血供) - presence of additional vasoconstrictor (血管收缩剂) - Duration prolonged by vasoconstrictor (epinephrine) - localizes agent to site of action - contraindicated in extremities(末梢部位) - Systemic Toxic Effects: CNS, cardiovascular Pharmacokinetics Distribution - LAs bind in the blood to a1-glycoprotein and albumin Alpha phase (快速吸收相) – rapidly redistributed to well-perfused tissues Beta phase (再分布相) – distribution to less perfused or slowly equilibrating tissues Gamma phase (消除相) – clearance representing metabolism and excretion Uses of local anesthesia / Modes of Administration • • • • • Topical local (surface) anesthesia(表面麻醉): for eye, ear, nose, and throat procedures and for cosmetic surgery Infiltration anesthesia (浸润麻醉): local injection around the region to be operated. Conduction anesthesia (传导麻醉): local injection around the peripheral nerve trunk Epidural anesthesia (硬膜下麻醉): local injection into the epidural space Subarachnoid anesthesia (蛛网膜下腔麻醉): or Spinal anesthesia (脊髓麻醉,腰麻): local injection into the cerebrospinal fluid in subarachnoid cavity 硬膜下 硬膜外 蛛网膜下腔 脊神经阻滞 椎旁阻滞 硬膜外阻滞 骶管阻滞 Adverse reactions Toxicity: CNS, CVS Allergic Reactions Metabolite of “ester” LAs Para-aminobenzoic acid(对氨基苯甲酸) Allergen Allergy to “amide” LAs is extremely rare Lidocaine(利多卡因) One of the most widely used local anesthetics Rapid onset, medium duration Also available in ointment(软膏), jelly(凝胶), and aerosol(喷雾剂) Other uses: anti-arrhythmic 1、抗癫痫药:分类,苯妥英钠 2、抗帕金森病药及抗老年性痴呆药 L-DOPA 3、抗精神病药和抗抑郁药 丙咪嗪、氯丙嗪 4、局部麻醉药:利多卡因 药理作用、作用机制、临床应用、不良反应、体内过程及 药物相互作用