Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
G protein–coupled receptor wikipedia , lookup
Tissue engineering wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Cell culture wikipedia , lookup
Cellular differentiation wikipedia , lookup
Cell encapsulation wikipedia , lookup
List of types of proteins wikipedia , lookup
VLDL receptor wikipedia , lookup
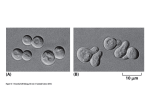
0021-972X/04/$15.00/0 Printed in U.S.A. The Journal of Clinical Endocrinology & Metabolism 89(9):4532– 4537 Copyright © 2004 by The Endocrine Society doi: 10.1210/jc.2003-031781 Pegvisomant, a Growth Hormone-Specific Antagonist, Undergoes Cellular Internalization M. MAAMRA, J. J. KOPCHICK, C. J. STRASBURGER, AND R. J. M. ROSS Division of Clinical Sciences (M.M., R.J.M.R.), Edison Biotechnology Institute (J.J.K.), and Department of Biomedical Sciences, Ohio University, Athens, Ohio 45701; and Division of Clinical Endocrinology, Department of Medicine, Charitè Campus Mitte (C.J.S.), Berlin, Germany GH binding to a receptor (GHR) dimer triggers signaling and internalization of the receptor/ligand complex. Pegvisomant is a specific GH antagonist developed for the treatment of acromegaly, and the basic molecule is GH with an amino acid substitution that blocks the conformational change necessary to generate functional GHR dimerization required for signal transduction. Pegvisomant has additional polyethylene glycol moieties to prolong its half-life in the circulation and improve clinical efficacy through reduced renal clearance. Pegvisomant has a long plasma half-life, and its mode of clear- P EGVISOMANT IS A specific GH antagonist used in the treatment of acromegaly (1, 2). GH initiates intracellular signaling by binding two molecules of its receptor (GHR) at the cell surface through two distinct binding sites. The affinity of GH binding site 1 for GHR is high, whereas the affinity of site 2 is lower. An amino acid substitution at residue G120 in binding site 2 of GH has been shown to inhibit GH-induced signal transduction (3–5). The genetically engineered GH receptor antagonist, B2036, is mutated at GH binding site 2 with G120K. B2036 has eight additional mutations at site 1 that increase the affinity of B2036 for soluble GHR. The pegylated counterpart of B2036, pegvisomant [polyethylene glycol (PEG)], is generated by the conjugation of B2036 with four or five moieties of PEG 5000 (pegylation). The GHR is devoid of intrinsic kinase activity and acts through recruitment of the tyrosine kinase, Janus kinase 2, at the conserved cytokine receptor motif, box 1, leading to the activation of the Janus kinase-signal transducer and activator of transcription and mitogen-activated protein kinase signaling pathways. GH binding occurs sequentially, with the first receptor binding to GH through site 1, and the second GHR binding to GH through binding site 2. Recent evidence suggests that the GHR may exist as a preformed dimer (6, 7), and that GH triggers a conformational change required for signaling similar to that demonstrated for the erythropoietin receptor (8, 9). However, the evidence of a GHR preformed dimer has not been demonstrated with the same rigor as that for the erythropoietin receptor. The antagonist B2036 binds Abbreviations: GHR, GH receptor; PEG, polyethylene glycol. JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the endocrine community. ance has not been established. We have studied pegvisomant internalization and demonstrate that despite its size and prolonged plasma half-life, it is internalized by cells expressing the GHR. As pegvisomant does not activate intracellular signal transduction systems, our results support the concept that the conformational changes required for GHR signaling are not essential for the intracellular trafficking of the ligand and establish one potential contributing mechanism for pegvisomant clearance. (J Clin Endocrinol Metab 89: 4532– 4537, 2004) to a receptor dimer, but does not trigger the essential change in conformation required for signaling (7, 10). Little is known about the biology of pegvisomant, because pegylation makes it difficult to generate specific antibodies and inhibits radiolabeling of the molecule. Renal excretion is considered the major route for GH clearance (11–13), and it has been generally assumed that the prolonged plasma halflife of pegvisomant is due to reduced renal clearance. In this study we developed an immunofluorescence method to examine the internalization of GH, B2036, and pegvisomant. We present evidence that despite being pegylated, pegvisomant is internalized in cells expressing the GHR. Materials and Methods Reagents Recombinant human GH (genotropin) was obtained from Pharmacia Biotech (Uppsala, Sweden). B2036 and pegvisomant were supplied by Sensus Corp. (Austin, TX). The anti-GH 10A7 antibody has cross-reactivity with pegvisomant, although the affinity is 25–50% less than that for GH (13, 14). The avidin-biotin blocking kit and Vectashield mounting solution were purchased from Vector Laboratories, Inc. (Peterborough, UK). The biotin-xx Fab goat antimouse antibody, Alexa488-streptavidin, Alexa488-goat antimouse antibody, and Alexa594-transferrin were purchased from Molecular Probes (Leiden, The Netherlands). Cell culture The HEK293 cell line stably expressing the full-length human GHR (293GHR) has been previously described (15). The cells were maintained in DMEM-Nut F-12, supplemented with 10% fetal calf serum, 100 IU penicillin, 100 g/ml streptomycin, 2 mg/ml fungizone, 2 mm lglutamine, and 400 g/ml geneticin, buffered with HEPES, and routinely grown at 37 C in a 95% humidified atmosphere of 5% CO2. Immunocytochemistry Four-well chambered glass slides (Nunc Labtech, Paisley, UK) were coated with a polylysine/fibronectin (20 g/ml of each) mix in 4532 Maamra et al. • Internalization of Pegvisomant J Clin Endocrinol Metab, September 2004, 89(9):4532– 4537 4533 FIG. 1. Internalization of GH, B2036, and pegvisomant. To study the internalization of GH, B2036, and pegvisomant, cells were incubated with ligand (200, 200, and 5000 ng/ml, respectively) for 30 min and fixed in paraformaldehyde. Immunofluorescence detection of ligand was performed on permeabilized and nonpermeabilized cells. All three ligands show both membrane binding (nonpermeabilized) and internalization (permeabilized), although the percent internalization of GH was greater than those of B2036 and pegvisomant (P ⬍ 0.001). PBS for 2 h before plating cells. 293GHR cells were plated at 3 ⫻ 104 cells/well and allowed to settle for 24 – 48 h before treatment. Cells were exposed to GH, B2036, or pegvisomant in serum-free medium. After ligand exposure, cells were fixed in a nonpermeabilized state (to show cell membrane binding) in 2% paraformaldehyde for 20 min or for an additional 3 min in paraformaldehyde with 0.1% Triton when permeabilization was required to allow immunostaining within the cell (to demonstrate internalized ligand). The buffer used for immunostaining was PBS supplemented with 0.1% BSA. For intracellular staining, the buffer was supplemented with 0.1% saponin to reduce nonspecific staining. After fixing, cells were treated for 1 h with buffer and 5% goat serum to block nonspecific binding sites. Cells were rinsed briefly and incubated for 15 min with avidin- blocking solution, followed by rinsing and incubation for 15 min with biotin-blocking solution to ensure that all endogenous avidin- and biotin-binding sites were blocked [according to the manufacturer’s instructions (Vector Laboratories, Inc.)]. Subsequent antibody incubations were performed in buffer supplemented with 1% goat serum. Ligands were detected with the specific monoclonal anti-GH antibody 10A7 (4 g/ml) that recognizes an epitope independent of the GHR binding domain, a secondary biotinylated goat antimouse antibody (40 g/ml), or the Alexa488-labeled goat antimouse antibody. Fixed cells were incubated with streptavidin-Alexa488 (4 g/ml) in buffer supplemented with 1% goat serum. Five- to 10-min washes were performed between incubations using PBS (nonpermeabilized) or PBS supplemented with 0.1% saponin. 4534 J Clin Endocrinol Metab, September 2004, 89(9):4532– 4537 Maamra et al. • Internalization of Pegvisomant Fluorescence microscopy imaging of slides Fluorescence was visualized by confocal microscopy using a ⫻60 or ⫻40 oil lens with a CLSM2010 confocal fluorescent microscope (Molecular Dynamics, Sunnyvale, CA) equipped with dual fluorescence and transmission detection. Images were file transfer protocoled from the INDY (Silicon Graphics, Mountain View, CA) on the CSLM 2010, converted to MAC 8-bit Tagged Image File Format files (Apple Computer, Cupertino, CA), and analyzed with NIH Image, and the data were exported to EXCEL (Microsoft, Redmond, WA) for further analysis. Image analysis and statistics Image analysis was performed with the NIH Image program (http:// rsb.info.nih.gov/nih.image). For the percent internalization studies, the fluorescence of 10 cells in each permeabilized and nonpermeabilized well was analyzed, and the results were expressed as a percentage of the total fluorescence. Analysis of the internalization rates between GH and pegvisomant was performed using ANOVA. Results Internalization of GH, B2036, and pegvisomant (Fig. 1) To study internalization 293GHR cells were exposed for 30 min to GH, B2036, or pegvisomant at concentrations similar to those found in the treatment of acromegaly (200, 200, and 5000 ng/ml, respectively). After ligand exposure, cells were fixed either in a nonpermeabilized state (to show cell surface binding) or after permeabilization to allow immunostaining within the cell (to demonstrate internalized GH or antagonist). Cells exposed to PBS alone showed no specific fluorescence. GH showed less labeling at the cell surface, and the majority of GH was internalized. In cells exposed to B2036, there was clear plasma membrane binding and internalization. Similar results were seen in cells exposed to pegvisomant (5000 ng/ml). Analysis of at least 10 cells in each condition revealed that the percentage of total intracellular fluorescence was 91.4.0 ⫾ 2.1% for GH, 55.6 ⫾ 3.5% for B2036, and 58.3 ⫾ 6.0% for pegvisomant (P ⬍ 0.001 for B2036 and pegvisomant vs. GH). The mean size of intracellular particles was not significantly different among GH-, B2036-, and pegvisomant-treated cells (47.0 ⫾ 3.0, 42.0 ⫾ 3.2, and 35.0 ⫾ 4.7 pixels, respectively). Dose-dependent intracellular accumulation of pegvisomant (Fig. 2) The above experiment was performed with a single dose of pegvisomant (5000 ng/ml). In this experiment, we investigated whether intracellular accumulation of pegvisomant was influenced by dose. To determine whether pegvisomant would accumulate inside the cell, 293GHR cells were exposed for 30 and 120 min to increasing concentrations of pegvisomant. After exposure, cells were fixed and permeabilized to allow immunostaining of internalized antagonist. Pegvisomant intracellular localization was detected both after 30 and 120 min of treatment (Fig. 2A). Analysis of at least 10 cells at each dose and time point showed that increasing pegvisomant concentrations led to a dose-dependent increase in intracellular mean cell fluorescence (Fig. 2B shows data from 120 min). No uptake of Pegvisomant was observed in parental 293 cells not expressing the GHR (data not shown). FIG. 2. Dose-dependent intracellular staining with pegvisomant. A, To study the intracellular uptake of pegvisomant, 293GHR cells were incubated with increasing concentrations of pegvisomant for 30 min and 2 h. Cells were then fixed in a permeabilized state, and immunostaining was performed. B, 293GHR cells were incubated with increasing concentrations of pegvisomant for 2 h. Ten cells were analyzed for fluorescence intensity (mean ⫾ SEM). There was a dosedependant increase in intracellular staining (P ⬍ 0.001). Maamra et al. • Internalization of Pegvisomant Intracellular colocalization of GH and B2036 with transferrin (Fig. 3) To assess whether mutations in B2036 alter intracellular trafficking in 293GHR, cells were treated with GH or B2036 in the presence of Alexa594-labeled transferrin. Immunostaining was performed immediately after incubation with ligand, and fluorescence was analyzed by superimposing transferrin fluorescence (red) on that of ligand (green; Fig. 3 shows results at 30 min). After 10- and 30-min incubations with ligand, similar colocalization with transferrin was observed for both GH and B2036, suggesting that intracellular compartment trafficking does not differ between GH and the antagonist. Analysis of trafficking after ligand pulse exposure (Fig. 4) In the above experiment, fixation of cells was performed while cells were still being exposed to ligand, that is cells were exposed to ligand throughout the experiment. Thus, at the time of fixation (10 and 30 min), some ligand would still be being internalized while the early internalized ligand would be entering the recycling pathway. To follow the passage of ligand within the cell, we exposed cells to a pulse of ligand, followed by a washing step and then incubation for varying periods before fixation. 293GHR cells were exposed to a 15-min pulse of GH, pegvisomant, or B2036 in the presence of Alexa594 transferrin. After the ligand pulse, cells were rinsed and incubated in starvation medium for 10, 15, 30, 60, 120, and 180 min before fixing and staining. Intracellular fluorescent vesicles were detectable in all GH-, B2036-, and pegvisomant-treated cells. Intracellular localization was similar for all three ligands, with a vesicular pattern and accumulation in the central part of the cells observed 10 min J Clin Endocrinol Metab, September 2004, 89(9):4532– 4537 4535 postpulse. All three ligands showed colocalization with transferrin. Figure 4 shows results at 60 min. There was no difference between the ligands at the other time points (10, 15, 30, and 120 min). Discussion Pegylation increases the plasma half-life of hormones by reducing renal clearance and intravascular proteolysis (16). Pegvisomant has a prolonged plasma half-life, and high levels are achieved after administration to humans (14). Our results demonstrate that pegvisomant is internalized into cells expressing the GHR, thus providing one mechanism for pegvisomant clearance. The dynamics of pegvisomant internalization differed from those of GH; however, intracellular trafficking was similar. The kidney is responsible for clearance of up to 60 –70% of circulating GH, and until recently the GHR was also thought to be a determinant of GH clearance (12, 17). Studies with pegvisomant, however, demonstrate that GHR blockade does not alter the metabolic clearance rate of GH (13). Thus, for GH, GHR-mediated cellular internalization does not appear to contribute to the metabolic clearance rate. In contrast, pegvisomant has a greatly reduced renal clearance rate; thus, minor contributors to clearance may become more relevant. We suggest that GHR-mediated cellular internalization may be one possible mechanism of pegvisomant clearance from the circulation. The percentages of pegvisomant and B2036 internalized were less than that of GH; more than 90% of GH was within the cell after a 30-min incubation. The intensity of binding on the cell surface for B2036 and pegvisomant was greater than that for GH. One needs to be careful in comparing the in- FIG. 3. Transferrin colocalization with GH and B2036. To study the trafficking after internalization of GH and B2036, cells were incubated with ligand (500 ng/ml) for 30 min in the presence of Alexa594-transferrin before fixing and immunostaining. Ligand fluorescence is shown in green, and transferrin in red. In the overlay (ligand⫹transferrin), colocalization is shown in yellow. 4536 J Clin Endocrinol Metab, September 2004, 89(9):4532– 4537 Maamra et al. • Internalization of Pegvisomant FIG. 4. Analysis of trafficking after ligand pulse exposure. 293GHR cells were incubated for 15 min with GH, B2036, and pegvisomant. Cells were then carefully rinsed, and the medium was replaced with ligand-free medium and incubated for 60 min before fixing and staining. Ligand fluorescence is shown in green, and transferrin in red. In the overlay (ligand⫹transferrin), colocalization is shown in yellow. tensity of fluorescence between ligands, because the affinity of the detection antibody differed between the ligands. However, in the calculation of percent internalization, we are comparing the same ligand at the cell surface with that internalized under identical experimental conditions. Therefore, we can be confident that there is a difference among GH, B2036, and pegvisomant. It is perhaps not surprising that B2036 and pegvisomant do have different cell surface binding, because conformation of the antagonist-receptor complex must be different from that of the GH-receptor complex. We know that B2036 binds to a receptor dimer, but does not induce the conformational change required for signal transduction (7), that GH accelerates GHR internalization (18), that internalization is not required for signaling (19), and we now recognize that signaling is not required for internalization. Our results confirm previous observations that although receptor dimerization is required for GHR internalization, the trafficking process is disassociated from receptor signaling (7, 10). The cytoplasmic domain of the receptor is required for GHR internalization, because an amino acid substitution in the rat receptor at box 1 prevents receptor internalization (19). Also, the truncated human GHR lacking the cytoplasmic domain of the receptor fails to internalize (15). The observation that B2036 and pegvisomant show greater fluorescence at the cell surface may relate to a different conformation of the ligand-GHR complex delaying triggering of internalization and increasing residence of antagonist at the cell surface. We accept that all of our data relate to studies in cells overexpressing the GHR. We have attempted studies in primary hepatocytes (data not shown); however, the sensitivity of immunofluorescence was not sufficient to obtain meaningful results. It is possible that overexpression of receptor could lead to a change in intracellular trafficking; however, our observations do demonstrate that pegvisomant is internalized by a GHR-mediated process and that intracellular trafficking is similar to that seen for GH. GH, B2036, and pegvisomant accumulated within the cell during prolonged exposure, and colocalization with transferrin suggests that the majority of ligand enters the recycling pathway associated with the receptor (20), although in previous studies with iodinated GH, only 25% of GH was recycled out of the cell intact (21). It is possible that during the trafficking of ligand there is degradation, with loss of pegy- Maamra et al. • Internalization of Pegvisomant lated moieties; however, our results demonstrate that despite its increased size and reduced binding affinity compared with GH, pegvisomant is internalized into GHR-expressing cells. To our knowledge, this is the first demonstration of internalization of a pegylated hormone and provides one mechanism for pegylated hormone clearance. Acknowledgments Received October 10, 2003. Accepted June 9, 2004. Address all correspondence and requests for reprints to: Dr. Richard J. M. Ross, Sheffield University, Clinical Sciences, Northern General Hospital, Sheffield, United Kingdom S5 7AU. E-mail: [email protected]. This work was supported by an Endocrine Care Prize from Pharmacia (to M.M.). References 1. Trainer PJ, Drake WM, Katznelson L, Freda PU, Herman-Bonert V, van der Lely AJ, Dimaraki EV, Stewart PM, Friend KE, Vance ML, Besser M, Scarlett JAA 2000 Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N Engl J Med 342:1171–1177 2. van der Lely AJ, Hutson RK, Trainer PJ, Besser GM, Barkan AL, Katznelson L, Klibanski A, Herman-Bonert V, Melmed S, Vance ML, Freda PU, Stewart PM, Friend KE, Clemmons DR, Johannsson G, Stavrou S, Cook DM, Phillips LS, Strasburger CJ, Hackett S, Zib KA, Davis RJ, Scarlett JA, Thorner MO 2001 Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. Lancet 358:1754 –1759 3. Chen WY, Wight DC, Wagner TE, Kopchick JJ 1990 Expression of a mutated bovine growth hormone gene suppresses growth of transgenic mice. Proc Natl Acad Sci USA 87:5061–5065 4. Chen WY, Wight DC, Chen NY, Coleman TA, Wagner TE, Kopchick JJ 1991 Mutations in the third ␣-helix of bovine growth hormone dramatically affect its intracellular distribution in vitro and growth enhancement in transgenic mice. J Biol Chem 266:2252–2258 5. Chen WY, Wight DC, Mehta BV, Wagner TE, Kopchick JJ 1991 Glycine 119 of bovine growth hormone is critical for growth-promoting activity. Mol Endocrinol 5:1845–1852 6. Gent J, van Kerkhof P, Roza M, Bu G, Strous GJ 2002 Ligand-independent growth hormone receptor dimerization occurs in the endoplasmic reticulum and is required for ubiquitin system-dependent endocytosis. Proc Natl Acad Sci USA 99:9858 –9863 7. Ross RJM, Leung KC, Maamra M, Bennett W, Doyle n, Waters MJ, Ho KKY 2001 Binding and functional studies with the growth hormone receptor an- J Clin Endocrinol Metab, September 2004, 89(9):4532– 4537 4537 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. tagonist, B2036-PEG (pegvisomant), reveal effects of pegylation and evidence that it binds to a receptor dimer. J Clin Endocrinol Metab 86:1716 –1723 Remy I, Wilson IA, Michnick SW 1999 Erythropoietin receptor activation by a ligand-induced conformation change. Science 283:990 –993 Livnah O, Stura EA, Middleton SA, Johnson DL, Jolliffe LK, Wilson IA 1999 Crystallographic evidence for preformed dimers of erythropoietin receptor before ligand activation. Science 283:987–990 Harding PA, Wang X, Okada S, Chen WY, Wan W, Kopchick JJ 1996 Growth hormone (GH) and a GH antagonist promote GH receptor dimerization and internalization. J Biol Chem 271:6708 – 6712 Johnson V, Maack T 1977 Renal extraction, filtration, absorption, and catabolism of growth hormone. Am J Physiol 233:F185–F196 Haffner D, Schaefer F, Girard J, Ritz E, Mehls O 1994 Metabolic clearance of recombinant human growth hormone in health and chronic renal failure. J Clin Invest 93:1163–1171 Veldhuis JD, Bidlingmaier M, Anderson SM, Evans WS, Wu Z, Strasburger CJ 2002 Impact of experimental blockade of peripheral growth hormone (GH) receptors on the kinetics of endogenous and exogenous GH removal in healthy women and men. J Clin Endocrinol Metab 87:5737–5745 Thorner MO, Strasburger CJ, Wu Z, Straume M, Bidlingmaier M, Pezzoli S, Zib K, Scarlett JC, Bennett WF 1999 Growth hormone (GH) receptor blockade with a PEG-modified GH (B2036-PEG) lowers serum insulin-like growth factor-I but does not acutely stimulate serum GH. J Clin Endocrinol Metab 84:2098 –2103 Maamra M, Finidori J, Von Laue S, Simon S, Justice S, Webster J, Dower S, Ross R 1999 Studies with a growth hormone antagonist and dual-fluorescent confocal microscopy demonstrate that the full-length human growth hormone receptor, but not the truncated isoform, is very rapidly internalized independent of Jak2-Stat5 signaling. J Biol Chem 274:14791–14798 Clark R, Olson K, Fuh G, Marian M, Mortensen D, Teshima G, Chang S, Chu H, Mukku V, Canova-Davis E, Somers T, Cronin M, Winkler M, Wells JA 1996 Long-acting growth hormones produced by conjugation with polyethylene glycol. J Biol Chem 271:21969 –21977 Baumann G 1991 Growth hormone heterogeneity: genes, isohormones, variants, and binding proteins. Endocr Rev 12:424 – 449 Roupas P, Herington AC 1988 Intracellular processing of growth hormone receptors by adipocytes in primary culture. Mol Cell Endocrinol 57:93–99 Allevato G, Billestrup N, Goujon L, Galsgaard ED, Norstedt G, Postel-Vinay MC, Kelly PA, Nielsen JH 1995 Identification of phenylalanine 346 in the rat growth hormone receptor as being critical for ligand-mediated internalization and down-regulation. J Biol Chem 270:17210 –17214 Hopkins CR, Trowbridge IS 1983 Internalization and processing of transferrin and the transferrin receptor in human carcinoma A431 cells. J Cell Biol 97: 508 –521 Roupas P, Herington AC 1987 Receptor-mediated endocytosis and degradative processing of growth hormone by rat adipocytes in primary culture. Endocrinology 120:2158 –2165 JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.