Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CCR5 receptor antagonist wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Pharmacogenomics wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Toxicodynamics wikipedia , lookup
NMDA receptor wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Gastrointestinal tract wikipedia , lookup
Neuropharmacology wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
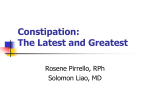
Review Central & Peripheral Nervous Systems Treatment of opioid-induced gut dysfunction Peter Holzer 1. Introduction Research Unit of Translational Neurogastroenterology, Institute of Experimental and Clinical Pharmacology, Medical University of Graz, Universitätsplatz 4, A-8010 Graz, Austria 2. Opioid peptides and opioid receptors in the gastrointestinal 3. Opioid actions in the ly t c gastrointestinal tract 4. Significance of endogenous opioid peptides in gastointestinal physiology 5. Homeostatic roles of dysfunction di receptor stimulants under 7. Adverse effects of opioid receptor agonists on gut function: opioid-induced bowel dysfunction and prolongation of postoperative ileus 8. Treatment of opioid-induced 1. Introduction disturbances of bowel function and related substances contained in the unripe seed capsules of . Morphine Papaver somniferum have been used to treat pain and diarrhoea for thousands of with laxatives and non-opioid d Lt 9. Management of opioid-induced receptor antagonists with a a peripherally restricted site of action rm fo n fI 10. Opioid receptor antagonists with a peripherally restricted o t h site of action as possible ig r y prokinetic drugs 11. Expert opinion p o C ri t s d n Keywords: alvimopan, constipation, a enteric nervous system, intestinal peristalsis, naloxone, N-methylnaltrexone, opioid peptides, opioid-induced bowel dysfunction, peripherally restricted g opioid receptor antagonists, in prokinetic effects t in Drugs (2007) 16(2):181-194 Expert Opin. Investig. r P conditions of gut dysfunction UK pr s 6. Beneficial effects of opioid bowel dysfunction by opioid b tri n tio u endogenous opioids in gut prokinetic drugs b i oh Opioid analgesics are the mainstay in the treatment of moderate-to-severe pain, yet their use is frequently associated with adverse effects, the most common and debilitating being constipation. Opioid-induced motor stasis results from blockade of gastrointestinal peristalsis and fluid secretion, and reflects the action of the endogenous opioid system in the gut. Methylnaltrexone and alvimopan are new investigational drugs that selectively target peripheral µ-opioid receptors because they are poorly absorbed in the intestine and do not enter the brain. Clinical studies have proved the concept that these drugs prevent opioid-induced bowel dysfunction without interfering with analgesia. As reviewed in this article, opioid receptor antagonists with a peripherally restricted site of action also hold therapeutic promise in postoperative ileus and chronic constipation due to the fact that they have been found to stimulate intestinal transit. tract years. At present, opioid analgesics are the mainstay of therapy in many patients with moderate-to-severe pain. Unfortunately, adverse effects can severely compromise the therapeutic benefit offered by these drugs [1]. The gastrointestinal (GI) tract is one of the main targets of their unwanted actions and, in this property, opioid analgesics are similar to other neuroactive drugs, notably adrenoceptor agonists [2-4]. This pharmacological profile reflects the significant role that neurons play in GI function and the fact that many of the transmitters and transmitter receptors present in the brain have also been localised to the gut. This is particularly true for opioid receptors and adrenoceptors whose activation by opiates and catecholamines, respectively, interferes with pathways of the enteric nervous system that regulate motility and secretion [1-9]. To comprehend the adverse actions of opioid analgesics and other neuroactive drugs on the gut, it needs to be considered that the alimentary canal is equipped with the largest collection of neurons outside the CNS. Enteric neurons originating from the myenteric and submucosal plexuses supply all of the layers of the alimentary canal and, therefore, are in a position to regulate virtually every aspect of digestion [10-12]. These neurons not only synthesise and release acetylcholine, substance P, NO, ATP, vasoactive intestinal polypeptide and 5-HT but also opioid peptides as their transmitters. The enteric nervous system is arranged in polarised circuits that are typically composed of intrinsic primary afferent neurons, a variable number of interneurons and excitatory or inhibitory output (motor, secretomotor and vasodilator) neurons to the effector tissues [10-12]. With this organisation, the 10.1517/13543784.16.2.181 © 2007 Informa UK Ltd ISSN 1354-3784 d ite 181 Treatment of opioid-induced gut dysfunction enteric nervous system is capable of regulating GI peristalsis, ion and fluid secretion, circulation, endocrine and immune activity independently of the brain [10-12]. 2. Opioid peptides and opioid receptors in the gastrointestinal tract The adverse influence of opioid analgesics on GI function remained an enigma to scientists until it was realised that both opioid peptides and opioid receptors are expressed in the digestive tract; therefore, it is important to briefly consider the endogenous opioid system in the gut and its physiological and pathophysiological implications (Figure 1) to understand the basis of opioid-induced bowel dysfunction (OBD). Met-enkephalin, leu-enkephalin, β-endorphin and dynorphin are among the endogenous opioids that are present in the GI tract where they have been localised to both neurons and endocrine cells of the mucosa [1,5,13]. Neuroanatomical tracing studies have revealed that opioid peptides are present in distinct classes of enteric neurons in the guinea-pig, notably in myenteric neurons projecting to the circular muscle and in neurons of descending enteric pathways [13-15]. The presence of endogenous opioids in the alimentary canal is matched by the expression of opioid receptors that mediate the effect of both endogenous and exogenous opioid receptor ligands on bowel function. By using mRNA quantification and immunocytochemistry, opioid receptors of the µ-, κ- and δ-subtype have been localised to the GI tract of rats, guinea-pigs and humans [13,16-18]. In the rat and guinea-pig, all three subtypes of opioid receptors are found on neurons of the myenteric and submucosal plexuses and on nerve fibres supplying muscularis and mucosa; however, their relative distribution varies with GI layer, GI region and species [13]. In the human gut, µ-opioid receptors are present on myenteric and submucosal neurons and on immune cells of the lamina propria [13]. animals; however, analysis of the cellular mechanisms of opiate action has shown that opioid receptor agonists can interrupt both excitatory and inhibitory neural inputs to the GI muscle in both human and animal models [21]. Inhibition of excitatory neural inputs is associated with inhibition of the release of excitatory transmitters such as acetylcholine and blockade of distension-induced peristaltic contractions, whereas blockade of inhibitory neural inputs results in depression of NO release from inhibitory motor neurons, disinhibition of GI muscle activity, elevation of resting muscle tone and non-propulsive motility patterns [6,8,13,21,23,24]. A direct activation of the interstitial cell–muscle network has also been envisaged [25,26]. In the canine gut, µ-opioid receptor agonists have a biphasic excitatory and inhibitory influence on the migrating myoelectrical complex [27], and transit in the human colon is retarded by activation of µ-opioid (but not κ-opioid) receptors [28,29]. Other studies have shown that activation of µ-opioid receptors in the human gut can increase pyloric tone, induce pyloric (as well as duodenojejunal phasic) pressure activity and elevate the resting anal sphincter pressure [30,31]. The relative contribution of these multiple effects to opioid-induced constipation is not clear [7]. Apart from affecting GI motor activity, opioids also influence GI ion and fluid transport (Figure 1). Blunted peristalsis delays GI transit and, thereby, prolongs the contact of the intestinal contents with the mucosa [1]. As a result, absorption of fluid is increased, whereas the secretion of electrolytes and water is decreased in the small and large intestines [6,21,32,33]. The antisecretory effect of opiates is mediated by opioid receptors on enteric neurons, whose activation results in the interruption of prosecretory enteric reflexes [6,21]. The actions of endogenous opioids on the GI tract are mediated by multiple opioid receptors. Studies with isolated tissues from the human intestine suggest that δ-, κ- and µ-opioid receptors contribute to opiate-induced inhibition of muscle activity [34,35]. Propulsion in the rat intestine is blocked by δ- and µ- (but not κ-) opioid receptor agonists [6], whereas peristalsis in the guinea-pig intestine is suppressed by activation of κ- and µ- (but not δ-) opioid receptors [20]. Opiate-induced inhibition of cholinergic transmission in the guinea-pig gut is similarly mediated by µ- and κ-opioid receptors [36]. Opioid receptors belong to the family of metabotropic membrane receptors that couple via the Gi/Go subtypes of G proteins to cellular transduction processes. Once activated by an agonist, µ-opioid receptors undergo endocytosis in a concentration-dependent manner [13,16,21]. The cellular effects of myenteric µ-opioid receptor activation are instigated by a multiplicity of signalling pathways including activation of K+ channels, membrane hyperpolarisation, inhibition of Ca2+ channels and reduced production of cAMP [21,36]. Taken together, opioid-induced constipation results from multiple effects, such as suppression of enteric neuron excitability, inhibition of excitatory and inhibitory neural ly t c u in r P . UK d Lt a m 3. Opioid actions in the or gastrointestinal tract f n When released fromI enteric neurons, it is likely that opioid f peptides play a o mediator role in the regulation of propulsion and secretiont . This conjecture is reflected by the h actions iof exogenous opioid receptor agonists and antagonists g on y GIr function (Figure 1). The inhibitory effect of opioid receptor p agonists on peristalsis in the guinea-pig small inteso tine is thought to arise primarily from the interruption of C [2,5,6,8,9,19-21] transmission within enteric nerve pathways governing muscle activity [13,21,22]. Transmission can be blocked both via presynaptic and postsynaptic sites of action on enteric neurons, whereby the release of acetylcholine and other transmitters is attenuated [6,21]. It has previously been believed that opiates inhibit GI propulsion in some species such as the guinea-pig by suppression of peristaltic contractions, whereas GI propulsion is interrupted through induction of non-propulsive contractions in the intestine of humans and non-rodent 182 g tin d n a Expert Opin. Investig. Drugs (2007) 16(2) di s b tri n tio ri t s b pr i oh d ite Holzer Gastrointestinal actions Cellular sources Met-enkephalin Leu-enkephalin β-Endorphin Dynorphin Enteric neurons • Neurons of the myenteric plexus with projections within the plexus to the circular muscle and to the mucosal plexus • Neurons of the submucosal plexus Endocrine cells Inhibition of enteric nerve activity • Suppression of enteric nerve excitability • Pre- and postsynaptic inhibition of transmission in excitatory and inhibitory motor as well as secretomotor pathways • Inhibition of the release of acetylcholine, substance P and NO Inhibition of propulsive motor activity • Inhibition of distension-induced peristalsis • Elevation of muscle tone • Induction of non-propulsive motility patterns • Disturbance of migrating myoelectrical complex • Inhibition of gastric emptying • Delay of gastrointestinal transit • Constipation b ly t c Molecular/cellular targets µ-Opioid receptors κ-Opioid receptors δ-Opioid receptors n Inhibition of secretory activity • Inhibition of ion and fluid secretion • Constipation Enteric neurons (somata and axons) Immune cells u tio b tri i oh pr ri t s Immune activity • Alteration of immune cell function s di d n a gastrointestinal tract. Figure 1. Schematic summary of the endogenous opioid system in the g in t inputs to the GI muscle and mucosa, inhibition of propulin It follows that the endogenous opioid peptides that are r in the course of propulsive motility sion, induction of non-propulsive motility patterns participate P and inreleased depression of secretory activity (Figure 1) . Although there the neural control of peristalsis as they dampen peri[37] [21] are species differences in the GI distribution of opioid receptors in the gut and the GI effect profile of opiates, emerging evidence indicates that the principal opioid actions on the enteric nervous system are seen in all mammalian species, although to a different degree depending on the experimental conditions. As a systematic comparison of opioid peptide occurrence, opioid receptor distribution and opioid effect profile in the gut of various species has not been performed, the true extent of species differences and the most appropriate animal model for OBD remain uncovered. d. a rm UK Lt fo n fI o t h 4. Significance of endogenous opioid peptides in gastointestinal physiology p o C ig r y There is evidence for a role of endogenous opioid peptides in the fine-tuning of gut functions. This concept is primarily based on the ability of opioid receptor antagonists to influence GI physiology and pathophysiology; for example, distension-evoked peristalsis can be facilitated by the pan-opioid receptor antagonist naloxone in various preparations of the guinea-pig, rabbit, cat and rat isolated small intestine [6,8,19,20]. In the guinea-pig small intestine, the effect of naloxone is mimicked by selective antagonists at µ- (cyprodime) and κ- (norbinaltorphimine) opioid receptors, but not by antagonism at δ-opioid receptors [20]. staltic performance via activation of µ- and κ-opioid receptors [20]. This inference is further supported by the ability of µ- and κ-opioid receptor antagonists to enhance the release of acetylcholine from the guinea-pig myenteric plexus [38]; by the ability of methylnaltrexone to enhance neurogenic contractions in the isolated human small intestine [39]; and by the ability of naloxone to increase the release of substance P from the peristaltically active guinea-pig ileum [37]. Naloxone has been found to accelerate transit in the colon but not the small intestine of healthy human volunteers [28,40]. This prokinetic effect is shared by the µ-opioid receptor-preferring antagonists methylnaltrexone [41] and alvimopan [42]. 5. Homeostatic roles of endogenous opioids in gut dysfunction Schaumann [43] interpreted the pharmacological effects of exogenous opiates on pain and bowel function as indicative of an endogenous protective system a long time before endogenous opioid peptides were identified [44]. Backed by increasing experimental support, it is now thought that endogenous opioids in the GI tract represent a system that defends the intestine against functional derangements created by inappropriate or adverse conditions such as prolonged Expert Opin. Investig. Drugs (2007) 16(2) d ite 183 Treatment of opioid-induced gut dysfunction intestinal distension, inflammation, stress and trauma [8,9]; for example, prolonged intraluminal distension of the guinea-pig ileum causes peristaltic activity that is interrupted by periods of inactivity during which the release of met-enkephalin is significantly enhanced [45]. This observation is consistent with the ability of naloxone to reduce the intermittent periods of peristaltic inactivity observed during prolonged periods of distension [46-48]. Studies of the effects of naloxone in rats suggest that endogenous opioids contribute to the ileal brake of the stomach-to-caecum transit caused by ileal infusion of lipids [49]. Disruption of the migrating myoelectrical complex caused by the administration of Escherichia coli endotoxin to fasted rats is reduced by naloxone [50]. This opioid receptor antagonist has no effect on the delay in rat GI transit (measured with a liquid dye marker) that is caused by abdominal skin incision or abdominal laparotomy but inhibits the delay in transit measured after abdominal laparotomy plus manipulation of the small and large intestines [51]. Furthermore, naloxone and methylnaloxone minimise the increase in rat colonic epithelial ion secretion and permeability that was observed after prolonged periods of stress [52]. There is increasing evidence that GI pathophysiology leading to gut motor inhibition is associated with upregulation and/or overactivity of the opioid system in the alimentary canal; for example, experimental inflammation enhances the potency of µ-opioid receptor agonists to inhibit GI transit and to increase the transcription and expression of µ-opioid receptors in the intestine of mice [53,54]. Abdominal surgery leads to an increase in the circulating levels of endomorphin in humans [55] and causes a profound internalisation of µ-opioid receptors in the myenteric plexus of the guinea-pig intestine [13], observations that may reflect a role of endogenous opioids in the pathophysiology of postoperative motor disturbances; therefore, it is emerging that endogenous opioids play a more important role in the pathological than in the physiological inhibition of gut motility [2,8]. Consistent with this concept is a limited number of small studies showing that naloxone can reverse idiopathic chronic constipation [56] and can have beneficial activity in patients with intestinal pseudo-obstruction [57] and constipation-predominant irritable bowel syndrome [58]; however, these studies need to be confirmed by larger controlled trials involving opioid receptor antagonists that have a more favourable pharmacokinetic profile than the short-lived naloxone to prove the concept. The effect of naloxone to normalise pathologically deranged GI motor activity is consistent with its ability to rescue peristalsis from experimentally induced inhibition. Thus, opioid receptor antagonism does not affect propulsion in the guinea-pig isolated colon under normal conditions but attenuates the inhibition of faecal pellet transport caused by granisetron, morphine or clonidine [59]. Similarly, naloxone is capable of reversing the inhibition of peristalsis in the guinea-pig small intestine caused by purinoceptor ligands, haloperidol, noradrenaline, atropine or hexamethonium [19,46,60,61]. With all of these findings together, it follows that endogenous opioids contribute to GI homeostasis, particularly under conditions of disturbed gut function. 6. Beneficial effects of opioid receptor stimulants under conditions of gut dysfunction ly t c u in r P . a fo rm n fI o t h ig r y p o C 184 UK d Lt g tin d n a b tri n tio pr ri t s s di 7. Adverse effects of opioid receptor agonists on gut function: opioid-induced bowel dysfunction and prolongation of postoperative ileus There are two key GI syndromes associated with the use of opioid analgesics: OBD and postoperative ileus in which opiates are one of many factors contributing to prolonged GI motor stasis [1,7]. A delay in GI transit and constipation are the most common and often disabling side effects of opioid analgesics, which result from their spectrum of pharmacological actions to block propulsive peristalsis, inhibit intestinal ion and fluid secretion, and increase intestinal fluid absorption [6]; however, constipation is just one symptom of OBD, whose manifestations comprise incomplete evacuation, abdominal distension, bloating, abdominal discomfort and increased gastro- oesophageal reflux. In addition, OBD may lead to secondary complications such as pseudo-obstruction of the bowel, anorexia, nausea and vomiting as well as interference with oral drug administration and absorption [1,7,67]. The symptoms associated with OBD can profoundly impair the quality of life and (in some patients) can be so severe that they prefer to discontinue analgesic therapy rather than Expert Opin. Investig. Drugs (2007) 16(2) b i oh The actions of opioid receptor agonists to inhibit GI secretory activity and transit are therapeutically used in acute and chronic diarrhoea as well as in irritable bowel syndrome associated with diarrhoea [7]. Inhibition of diarrhoea is achieved by two strategies. The first strategy is to target opioid receptors in the gut, a possibility that has long been accomplished by the development of loperamide. The antidiarrhoeal action of this compound is predominantly mediated by µ-opioid receptors and is restricted to the gut because loperamide is poorly absorbed and fails to cross the blood–brain barrier at concentrations needed to produce analgesia [6,30,62]. The second strategy is to inhibit enkephalinases that degrade endogenous opioids once they have been released from neurons or other cells in the GI tract. Inhibition of GI enkephalinases by racecadotril (acetorphan, a compound that does not enter the brain) prolongs the presence – and increases the concentration – of endogenous opioid peptides at opioid receptors in the alimentary canal [63,64]. In this way, the antisecretory and antitransit effects of endogenous opioid peptides are enforced, a result that is therapeutically used for the treatment of diarrhoea [65,66]. d ite Holzer experience the discomfort arising from OBD [1,67]. Unlike other adverse effects of chronic opioid therapy such as sedation, nausea and vomiting, which often resolve with continued use, OBD generally persists throughout treatment [1,68]; however, tolerance to the effects of morphine on enteric neurons has been found to occur in animal experiments in vitro [21]. Although centrally mediated effects of opiates to slow GI transit have been implicated in the pathophysiology of OBD [62], opiate-induced blockade of gut motility correlates better with opiate concentrations in the gut than with opiate concentrations in the brain [67,69]. In addition, the N-methyl quaternary analogues of naloxone and naltrexone (which do not cross the blood–brain barrier) have been found to fully antagonise the effects of morphine on opioid-induced effects in the canine and rat intestines [70,71]; therefore, it would seem that the adverse effects of opiates on GI function result primarily from interaction with opioid receptors in the gut [1,62]. Postoperative ileus occurs most commonly following abdominal or pelvic surgery and is characterised by bowel distension, lack of bowel sounds, accumulation of GI gas and fluid, nausea, vomiting and delayed passage of flatus and stool [1,4,7]. Motor stasis involves all segments of the digestive tract, the colon being most severely affected because the average paralytic state in this part of the intestine persists for 48 – 72 h [1]. Opioid analgesics have a profound inhibitory effect on postoperative GI motility and their use for postoperative analgesia delays recovery from postoperative ileus. There is a significant relationship between the amount of morphine administered and time required for resolution of ileus following colectomy [72]. The inhibitory effects of opioid analgesics on postoperative GI motility are observed during systemic opioid administration with patient-controlled analgesia and conventional intramuscular as well as epidural opioid administration [1]. As the pathophysiology of prolonged postoperative ileus involves inflammatory, immunological and neurogenic mechanisms [73,74], it should not be neglected that the effects of opioid analgesics on the immune system may be of relevance to their adverse influence on postoperative ileus [7]. postoperative ileus include metoclopramide, domperidone and erythromycin to stimulate primarily foregut motility; the cholecystokinin (CCK) analogue caerulein to stimulate small intestinal motility; acetylcholinesterase inhibitors such as neostigmine to enforce small and large intestinal tone; and the 5-HT4 receptor agonist tegaserod to stimulate colonic transit [1,4,76]. Erythromycin-related motilides, ghrelin analogues, the mixed 5-HT4 receptor agonist/5-HT3 receptor antagonist renzapride and the CCK1 receptor antagonist dexloxiglumide represent further prokinetic drug candidates that are in clinical development [4,76]; however, the therapeutic value of prokinetic drugs in the relief of postoperative ileus with or without opiate use remains unsubstantiated [1]. It seems that epidural local anaesthesia (among all of the available pharmacological treatment options) is the most effective method for relieving pain and shortening the duration of ileus [1]. Similarly, prokinetic drugs are used to ameliorate OBD, although laxatives are most commonly used in this situation [1,67,75]; however, these regimens often do not provide satisfactory relief from the GI manifestations of opioid-induced analgesia [1]. b ly t c u . a rm UK d Lt fo n fI o t h p o C 8. of opioid-induced disturbances of igTreatment r bowel function with laxatives and non-opioid y prokinetic drugs The pharmacological treatment of OBD and postoperative ileus associated with opiate use involves two approaches: non-specific treatment with laxatives and prokinetic drugs; and specific treatment with opioid receptor antagonists. As this review focuses on the second approach, the first approach involving non-opioid drugs is only briefly addressed. Laxative drugs (including softening, stimulant and osmotic laxatives) have long been used to ameliorate OBD [1,67,75]. The prokinetic treatment options for pr ri t s s di 9. Management of opioid-induced bowel dysfunction by opioid receptor antagonists with a peripherally restricted site of action g tin in r P d n a b tri n tio i oh The primary objective in the management of OBD (whether or not associated with postoperative ileus) is to prevent GI symptoms rather than treat established motor stasis due to opioid use [1]. For this reason, many opioid-sparing regimens (e.g., NSAIDs and tramadol) have been tested to circumvent the adverse GI sequelae of opioid use [1]; however, these regimens may lack efficacy in severe pain states or may themselves have adverse effects on the gut. Although transdermal administration of opiates such as fentanyl causes less constipation and results in a better quality-of-life rating than oral administration of morphine [1,77,78], this approach also represents only a partial solution of the problem. Given that opioid-induced analgesia is primarily mediated by µ-opioid receptors in the CNS, the rational approach to prevent OBD would be to combine opioid analgesics with opioid receptor antagonists that cannot penetrate the blood–brain barrier. As a result, the adverse effects of opioid analgesics on the GI system would be avoided, whereas their central analgesic action would remain unaltered. This approach has been validated by the use of opioid receptor antagonists with limited systemic absorption and by the development of peripherally restricted opioid receptor antagonists (PRORAs) such as methylnaltrexone and alvimopan. The latter two compounds are presently in clinical trials for the management of OBD and postoperative ileus (Table 1) and may also turn out to become prokinetic drugs to relieve intestinal stasis unrelated to opiate use. Expert Opin. Investig. Drugs (2007) 16(2) d ite 185 Treatment of opioid-induced gut dysfunction Table 1. Overview of fully published clinical trials of methylnaltrexone and alvimopan in OBD and postoperative ileus. Ref. Compound and dose Trial type Major outcome [41] Methylnaltrexone 0.3 mg/kg i.v. every 6 h Phase I Safety, pharmacokinetics and efficacy of methylnaltrexone to stimulate GI transit [85] Methylnaltrexone 0.64, 0.7, 2.1, 6.4 or 19.2 mg/kg p.o. Phase I Safety and efficacy of methylnaltrexone to prevent OBD [86] Methylnaltrexone 0.45 mg/kg i.v. Phase I Safety and efficacy of methylnaltrexone to prevent OBD [88] Methylnaltrexone 0.04, 0.08, 0.16, 0.32, 0.64 or 1.25 mg/kg i.v. Phase I Safety and pharmacokinetics of methylnaltrexone [89] Methylnaltrexone 0.3 mg/kg i.v. Phase I Efficacy of methylnaltrexone to ameliorate morphine-induced delay of gastric emptying [90] Methylnaltrexone 0.1 or 0.3 mg/kg s.c. Phase I [91] Methylnaltrexone 3.2 or 6.4 mg/kg p.o. Phase I [92] Methylnaltrexone 0.1 mg/kg/day i.v. Phase II [93] Methylnaltrexone 0.3 or 1 mg/kg p.o. Phase II [42] Alvimopan 12 mg b.i.d. p.o. Phase I [99] Alvimopan 4 mg p.o. Phase I [100] Alvimopan 0.5 or 1 mg q.d. p.o. Phase II [101] Alvimopan 1 or 6 mg b.i.d. p.o.* Phase II [102] Alvimopan 6 or 12 mg b.i.d. p.o.* Phase III [103] Alvimopan 6 or 12 mg b.i.d. p.o.* Phase III [104] Alvimopan 12 mg b.i.d. p.o.* Phase III [105] Alvimopan 6 or 12 mg b.i.d. p.o.* Phase III *The initial dose of alvimopan was given 2 h before surgery. GI: Gastrointestinal; OBD: Opioid-induced bowel dysfunction. UK a . d Lt The first attempt to selectively target opioid receptors in the periphery was made with naloxone and related tertiary opioid receptor antagonists such as nalmefene [1]. Naloxone is a pan-opioid receptor antagonist [79] whose systemic bioavailability following oral administration is as low as 2% because of extensive first-pass metabolism. For this reason, oral naloxone has been found to improve OBD without inhibiting opiate-induced analgesia [80-82]. However, it needs to be realised that naloxone can easily cross the blood–brain barrier; therefore, naloxone can reverse analgesia if given in sufficient dosage despite its low bioavailability [1]. Consequently, the therapeutic index of naloxone has turned out to be very narrow and its use limited because of the need to titrate active doses peripherally versus centrally [81]. Nalmefene is a µ-opioid receptor antagonist and its metabolite (nalmefene glucuronide) has been observed to selectively antagonise the GI effects of opioid analgesics in rodents; however, nalmefene glucuronide does not seem to be sufficiently selective for the gut to be clinically useful in humans [83]. fo n fI o t h ig r y p o C 186 pr ly t Pharmacokinetics and efficacy of methylnaltrexone to ameliorate ic OBD r t Pharmacokinetics and efficacy of methylnaltrexone to ameliorate OBD s Safety and efficacy of methylnaltrexone to ameliorate OBD due to n chronic methadone it o Safety and efficacy of methylnaltrexone to uameliorate OBD due to b chronic methadone i trstimulate GI transit and prevent OBD Safety and efficacy of alvimopansto Efficacy of alvimopan to prevent di OBD d to ameliorate OBD Safety and efficacy of alvimopan n a to shorten postoperative ileus Efficacy of alvimopan g Safety and efficacy n of alvimopan to shorten postoperative ileus i t Safety and n efficacy of alvimopan to shorten postoperative ileus i r Safety and efficacy of alvimopan to shorten postoperative ileus P Safety and efficacy of alvimopan to shorten postoperative ileus 9.1 Opioid receptor antagonists with limited systemic absorption rm b i oh 9.2 Methylnaltrexone An important advance in the search for PRORAs was the development of quarternary opioid receptor antagonists such as methylnaltrexone. Attaching a methyl group to the amine configuration in naltrexone results in methylnaltrexone (Figure 2), a drug that has greater polarity and lower lipid solubility than its parent compound [84]. Due to its quaternary structure, methylnaltrexone exhibits low oral bioavailability due to limited absorption and does not cross the blood–brain barrier [67,84,85]. As a result, this µ-opioid receptor-preferring antagonist (MIC = 70 nM) offers the therapeutic potential of preventing or reversing the undesired side effects of opioids in the gut without compromising analgesia or precipitating the opioid withdrawal symptoms that are predominantly mediated by opioid receptors in the brain [84]. Early studies have revealed that the adverse effect of the opiate on GI function is prevented without attenuation of analgesia following subcutaneous or intravenous administration of methylnaltrexone together with a centrally active opiate to dogs and humans [67,86], whereas analgesia is appreciably compromised in rats [70]. This species dependence of the peripheral selectivity of Expert Opin. Investig. Drugs (2007) 16(2) d ite Holzer + N N HO Methylnaltrexone Intravenous administration in healthy volunteers No adverse effects of clinical importance with methylnaltrexone ≤ 0.45 mg/kg [41,86] Orthostatic hypotension and lightheadedness following administration of methylnaltrexone 0.64 or 1.25 mg/kg at plasma levels in excess of 1.4 µg/ml [88] HO O HO Box 1. Significant adverse effects of methylnaltrexone and alvimopan relative to placebo. O Naltrexone Figure 2. Chemical methylnaltrexone. O HO O Methylnaltrexone structures of naltrexone ly t c . a n fo i r y p o C t h g I f o rm UK d Lt n tio ri t s Subcutaneous administration in healthy volunteers No adverse effects of clinical importance with methylnaltrexone ≤ 0.3 mg/kg [90] u b tri s di Oral administration in healthy volunteers No adverse effects of clinical importance with methylnaltrexone ≤ 19.2 mg/kg [85] g tin in r P pr Intravenous administration in methadone-maintained subjects Mild-to-moderate abdominal cramping following administration of methylnaltrexone 0.1 mg/kg [92] and methylnaltrexone arises from its demethylation to naltrexone, which readily penetrates the blood–brain barrier: demethylation occurs in mice and rats but is negligible in dogs and humans [87]. A substantial series of Phase I and II studies conducted by the group of Yuan [84] has established the pharmacodynamic, pharmacokinetic, therapeutic and safety profiles of methylnaltrexone [84]. The drug has been formulated as a solution for intravenous or subcutaneous administration as well as capsules/tablets for oral administration [84]. Both the parenteral and oral formulations as well as single- and repeated-dose regimens have been found to be effective in preventing the morphine-induced prolongation of gastric emptying and oral-to-caecal transit time without significantly attenuating morphine-induced analgesia (Table 1) [41,85-90]. Following injection of methylnaltrexone 0.3 – 0.45 mg/kg i.v., the time to maximum plasma concentration is ∼ 20 min, the elimination half-life in plasma is ∼ 1.5 – 3 h and the terminal half-life is ∼ 6 – 9 h [84]. Repeated administration of 0.3 mg/kg i.v. at 6-h intervals does not result in an accumulation of the drug [41] and the available data indicate that the metabolism of methylnaltrexone does not play a major role in its predominantly renal route of elimination [84]. Although readily bioavailable following parenteral administration, methylnaltrexone is absorbed from the GI tract only to a limited extent [85]. The plasma levels of methylnaltrexone are even lower when the drug is administered orally as an enteric-coated formulation, yet enteric-coated methylnaltrexone is more efficient in preventing morphine-induced retardation of oral-to-caecal transit time than the uncoated preparation [91]. Thus reduced oral bioavailability is associated with enhanced efficacy, which suggests that oral methylnaltrexone acts locally in the gut to reverse morphine-induced GI motor stasis. Methylnaltrexone is well tolerated at therapeutic doses (0.3 – 0.45 mg/kg i.v. and ≤ 19.2 mg/kg p.o.) with no significant adverse reactions, an outcome that is also true when methylnaltrexone 0.3 mg/kg i.v. is repeatedly administered every 6 h [41]. The only adverse reaction of note seen at supra-therapeutic doses (≤ 1.25 mg/kg i.v.) is transient orthostatic hypotension (Box 1) [88]. b i oh d n aOral administration in methadone-maintained subjects No adverse effects of clinical importance with methylnaltrexone 0.3 or 1 mg/kg [93] Alvimopan Oral administration in healthy volunteers No significant adverse effects with alvimopan 4 or 12 mg [42,99] Oral administration in patients receiving chronic opioid therapy Bowel-related adverse effects (abdominal cramping, nausea, vomiting and diarrhoea) with alvimopan 1 mg [100] Oral administration in patients undergoing surgery that is likely to result in postoperative ileus No significant adverse effects and no significant exacerbation of treatment-emergent adverse effects postoperatively with alvimopan 1, 6 or 12 mg [101-105] Nominal enhancement in the proportion of patients experiencing postoperative nausea and/or vomiting by alvimopan 12 mg during the inpatient period in 1 study [104] as opposed to a significant reduction in the incidence of post-operative nausea and vomiting by alvimopan 6 and 12 mg, respectively, in 2 other studies [101,103] Phase II studies have established that methylnaltrexone is capable of relieving constipation in methadone-maintained, opioid-dependent volunteers (Table 1). In a double-blind, randomised and placebo-controlled trial, it has been found that intravenous methylnaltrexone shortens the oral-to-caecal transit time and causes laxation associated with mild Expert Opin. Investig. Drugs (2007) 16(2) d ite 187 Treatment of opioid-induced gut dysfunction abdominal cramping but does not elicit any signs of opioid withdrawal [92]. Compared with placebo, oral methylnaltrexone is also capable of provoking laxation in methadone-maintained patients without precipitating opioid withdrawal in any subject [93]; however, the latency to the first bowel movement is significantly longer following oral intake of the drug than after intravenous administration. The doses of methylnaltrexone required to induce bowel movements in subjects on chronic methadone were lower than those required in subjects who were not opioid dependent (Table 1). The usefulness of methylnaltrexone to selectively counteract opiate-induced stasis in the GI tract has also been proven in Phase II and III studies of patients with advanced medical illness requiring high doses of opiates for pain control [84]. Similarly, patients with postoperative ileus following open segmental colonic resection have been reported to benefit from treatment with methylnaltrexone. Thus upper and lower bowel function recovers ∼ 1 day earlier in patients receiving intravenous methylnaltrexone than in placebo-treated patients, whereas no difference in opioid use or mean pain scores is observed [84]. This report of clinical efficacy is contrasted by an experimental study in rats in which intragastric methylnaltrexone (100 mg/kg) was found to be inactive in reversing postoperative inhibition of GI transit in the absence and presence of postoperative morphine treatment [94]. Following the proof-of-concept with methylnaltrexone, a µ-opioid receptor-preferring antagonist was developed with a peripherally restricted site of action and a potency (MIC = 0.77 nM) ∼ 100-fold higher than that of methylnaltrexone. This compound, alvimopan (ADL 8-2698, formerly known as LY-246736), exhibits both low systemic absorption (oral bioavailability of 0.03% in dogs and 6% in humans) and a limited ability to enter the brain due to its polar structure (Figure 3) [95-97]. Following intravenous administration, the half-life of alvimopan in the systemic circulation of dogs and rabbits is as short as 10 min. For this reason, alvimopan is intended primarily for oral administration, in which case it potently blocks µ-opioid receptors in the gut with a prolonged duration of action. Due to its pharmacokinetic properties, orally administered alvimopan mainly stays in the GI tract [95] and the main route of its excretion is via the faecal route, either in unchanged form or in the form of metabolites generated by microfloral activity [7,97]. There is no evidence of drug accumulation following chronic dosing of alvimopan [7]. Studies addressing the acute safety of alvimopan in animals and humans have shown that the drug is well tolerated; the only adverse effects of note include nausea, vomiting and abdominal discomfort [7]. The selectivity of the action of alvimopan for peripheral opioid receptors was first demonstrated by its ability to elicit diarrhoea in morphine-dependent mice without reversing morphine-induced analgesia [98]. In this study, alvimopan was found to have a prompt onset of action, which lasted for . a rm fo n fI o t h p o C 188 ly t c UK d Lt g tin d n a Expert Opin. Investig. Drugs (2007) 16(2) di s b tri n tio u in r P 9.3 Alvimopan ig r y ≥ 8 h [98]. Early Phase I studies established the clinical efficacy and safety of oral alvimopan [95]. In a double-blind cross-over study (Table 1), it was found that alvimopan 4 mg was capable of preventing morphine from delaying GI transit in healthy subjects as measured by the lactulose hydrogen breath test, without antagonising central morphine effects such as analgesia and pupillary constriction [95,99]. Similar results were obtained in a double-blind, randomised and placebo-controlled trial involving 74 healthy volunteers in which gastric emptying, and small bowel and colonic transit were assessed by scintigraphy [42]. Alvimopan 12 mg b.i.d. reversed the effect of codeine to delay small bowel, proximal and overall colonic transit but failed to antagonise the effect of codeine to slow gastric emptying [42]. The clinical testing of alvimopan was subsequently expanded to explore its usefulness in preventing or treating OBD and postoperative ileus [7,95-97]. In a randomised and placebo-controlled study involving 168 patients with OBD due to chronic opioid therapy for non-malignant pain or opioid addiction (Table 1), alvimopan 0.5 or 1 mg q.d. for 21 days showed significant efficacy in ameliorating constipation without compromising opioid analgesia [100]. The adverse effects that were associated with alvimopan were primarily bowel related, occurred during the first week of treatment and were of mild-to-moderate severity [100]. Compared with healthy subjects or patients with postoperative ileus, it seems that patients receiving chronic opioid treatment are particularly sensitive to alvimopan [7]. Given that OBD is thought to contribute to postoperative ileus, several studies have addressed the ability of alvimopan to shorten postoperative bowel dysfunction (Table 1). An experimental study in rats has shown that intragastric alvimopan 1 or 3 mg/kg is capable of reversing postoperative inhibition of GI transit in the absence and presence of postoperative morphine treatment; the effect of alvimopan being most pronounced when it is administered before surgery [94]. Similar results have been reported in patients with postoperative ileus, although with somewhat varying results, which may partly have been due to the rather wide range of doses (1 – 12 mg) tested. In these studies, the initial dose of alvimopan was usually administered ∼ 2 h before surgery and the drug subsequently dosed twice daily. Postoperatively, patient-controlled analgesia with intravenous opioids was instituted. In a first Phase II trial carried out with 78 patients who underwent partial colectomy or total abdominal hysterectomy, alvimopan 6 mg (but not 1 mg) shortened the time to achieve normal bowel function after the operation and the duration of hospitalisation by a median of 1 day [101]. In addition, the overall incidence of GI side effects including postoperative nausea and vomiting was also reduced by alvimopan, whereas analgesia was not compromised [101]. Following this promising outcome, several Phase III trials were initiated, four of which have been published so far (Table 1). In a placebo-controlled trial involving 469 patients undergoing bowel resection or radical hysterectomy, it was ri t s b pr i oh d ite Holzer 2H2O O HO H N N OH O volunteers, in which methylnaltrexone can stimulate GI transit as measured by the lactulose hydrogen breath test [41] and alvimopan is capable of accelerating colonic transit as measured by scintigraphy [42]. In view of this prokinetic activity, it has been hypothesised that PRORAs may ameliorate pathological states of GI motor stasis unrelated to opiate use, such as chronic idiopathic constipation and intestinal pseudo-obstruction [7,84]. Opioid receptor antagonists are expected to normalise pathological inhibition of gut function that arises from an upregulation and/or overactivity of the opioid system in the GI tract [2]. There is indeed preliminary evidence that naloxone has beneficial effects in idiopathic chronic constipation [57], intestinal pseudo-obstruction [57] and constipation-predominant irritable bowel syndrome [58]. In addition, preliminary data indicate that alvimopan is also capable of shortening bowel transit time in patients with chronic constipation [107]. b Figure 3. Chemical structure of alvimopan. confirmed that alvimopan 6 and 12 mg accelerated the time to recovery of GI function by a mean of 15 and 22 h, respectively [102]. The time to writing the hospital discharge order was shortened on average by 20 h in the group receiving alvimopan 12 mg [102]. In a similar Phase III study involving 451 patients subjected to partial colectomy or radical hysterectomy, alvimopan 6 mg was found to significantly accelerate the time to recovery of GI function by a mean of 14 h, whereas alvimopan 12 mg failed to significantly shorten recovery of bowel function [103]. In another double-blind, randomised and placebo-controlled Phase III trial involving 519 women scheduled for simple total abdominal hysterectomy, alvimopan 12 mg was observed to hasten the time to the first bowel movement by an average of 22 h and to increase the frequency of bowel movements [104]. Similar results were found in a study in 615 patients undergoing laparotomy for bowel resection or hysterectomy, in which both alvimopan 6 and 12 mg significantly accelerated GI recovery in terms of toleration of solid food, first bowel movement and writing of hospital discharge order [105]. In all of these trials, the incidence of adverse events was similar among the placebo and alvimopan treatment groups (Box 1) [106]. Postoperatively, the main treatment-emergent adverse effects were bowel related and included nausea, vomiting and abdominal discomfort. The incidence of postoperative nausea and vomiting was significantly reduced by alvimopan 6 and 12 mg, respectively, in 2 studies [101,103], whereas the proportion of patients who experienced nausea and/or vomiting was nominally enhanced by alvimopan 12 mg in another study [104]. The failure of alvimopan to antagonise opioid-induced analgesia was confirmed in all of the studies [100-105]. ly t c n tio i oh pr ri t s u b i tr the mainstay in the treatment of moderOpiates will remain s ate-to-severe pain di in the foreseeable future because the introduction of analgesic drugs with equal efficacy but a more d safety profile is not yet in sight. Consequently, any favourable n a that improves the tolerability of opioid analgesics measure g represents a progress in the treatment of pain. As outlined in tinthis review, the GI tract is one of the main sites of the unde- in r P . a rm UK d Lt fo n fI o t h p o C ig r y 10. Opioid receptor antagonists with a peripherally restricted site of action as possible prokinetic drugs As outlined in Section 5, PRORAs may have potential to alleviate intestinal motor stasis unrelated to opiate use. Thus naloxone is capable of stimulating peristalsis in the guinea-pig isolated small intestine [20], which suggests that peripheral opioid receptor antagonists may have a prokinetic action on the GI tract [2]. This prediction has been validated in healthy 11. Expert opinion sired effects of opiates because the enteric nervous system expresses all of the key subtypes of opioid receptors that (when activated) compromise GI function. This may be physiologically meaningful under conditions where the endogenous opioid system is activated but represents a nuisance when exogenous opiates are administered for therapeutic purposes. The potential of opiates to cause constipation and other bowel-related adverse reactions is (in fact) a serious drawback to the patients’ satisfaction with opioid analgesics. In addition, the use of opioids for postoperative pain control prolongs hospitalisation because of their potential to enforce and prolong postoperative ileus. As a result, many opioid-sparing approaches have been explored but the outcome has generally been unsatisfactory and has at best resulted in a partial solution of the problem. The development of opioid receptor antagonists with restricted access to the CNS has opened up a new approach to selectively control the adverse actions of opioid analgesics in the gut. This concept has been validated in an impressive manner by the clinical evaluation of methylnaltrexone and alvimopan, which are capable of preventing the undesired opioid effects on gut function at the same time as preserving the desired analgesic action of opiates on central pain control. This conclusion has been validated by a recent meta-analysis of the effect of alvimopan in the treatment of postoperative ileus [106]. Therefore, it is evident that analgesia and OBD can be dissociated in a pharmacological manner, which will theoretically allow for a more aggressive use of Expert Opin. Investig. Drugs (2007) 16(2) d ite 189 Treatment of opioid-induced gut dysfunction opioid analgesics with better pain relief but fewer side effects [67]; however, this claim has not yet been substantiated. Although methylnaltrexone and alvimopan display an excellent safety profile, they have bowel-related adverse effects of mild-to-moderate severity. It may by speculated that part of the undesired actions of PRORAs reflect a withdrawal reaction, especially in patients who have a history of long-term use of opiates. The concept of pharmacological dissociation of analgesia and OBD has been proven not only in healthy volunteers but also in patients with chronic opioid use for pain relief or substitution therapy for addiction. Both methylnaltrexone and alvimopan have been found to alleviate the symptoms of OBD without antagonising analgesia or precipitating signs of opioid withdrawal. Further studies defining optimal dosage and dosing regimen as well as long-term efficacy and safety are needed. To date, only 1 study in which alvimopan was given to patients with OBD due to chronic opioid therapy or opioid addiction for 21 days has been published [100]. In this trial, alvimopan 1 mg was found to induce a bowel movement in ∼ 50% of the patients, the effect being most prominent during the first 2 weeks [100]. Several Phase II and III trials have addressed the efficacy of methylnaltrexone and particularly of alvimopan to hasten the resolution of postoperative ileus under patient-controlled opioid analgesia. In assessing these trials, it has to be borne in mind that there is currently no consensus for defining postoperative ileus in terms of onset, duration and resolution of symptoms. Alvimopan and methylnaltrexone were reported to shorten the time to recovery of GI function (tolerance of solid food, and passage of flatus or stool) and to writing the hospital discharge order by variable degrees ≤ 1 day. As no approved treatment schedule for postoperative ileus exists as yet, these findings herald a significant advance in the clinical management of postoperative ileus and are encouraging to address a number of questions that remain unanswered: • How does the efficacy of alvimopan and methylnaltrexone, administered at optimal dosage, in preventing postoperative ileus compare with the efficacy of epidural anaesthesia/analgesia? • What are the optimal routes of administration of alvimopan and methylnaltrexone relative to the conditions to be treated? As oral alvimopan does not prevent the effect of codeine to delay gastric emptying [42], it could be argued that the benefit of alvimopan in postoperative ileus is limited by the delay of gastric emptying and consequently by the delay of its delivery to the intestine. Should this drug be administered by a postpyloric tube to ensure optimal prokinetic activity? • Is the therapeutic benefit gained by alvimopan and methylnaltrexone cost-effective? • Which group of patients undergoing a particular type of abdominal surgery benefit most from the ability of PRORAs to shorten postoperative ileus? • Does the reported variability in the therapeutic efficacy of alvimopan reflect different degrees of endogenous opioid involvement in postoperative ileus? • As parenteral methylnaltrexone is mostly eliminated by the renal route, does its dose need to be adjusted in patients with impaired renal function? ly t c u . a rm UK • Are the effects of alvimopan and methylnaltrexone relevant for the patient and do they represent a clinically relevant improvement in terms of shortening the hospital stay for the patient and reducing ileus-related complications? • Which dose of alvimopan and methylnaltrexone has the optimal efficacy/safety profile? • What is the optimal dosage of alvimopan and methylnaltrexone in the long-term management of OBD? fo n fI o t h ig r y p o C Bibliography 2. Papers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers. 1. •• 190 KURZ A, SESSLER DI: Opioid-induced bowel dysfunction: pathophysiology and potential new therapies. Drugs (2003) 63:649-671. A comprehensive review of OBD. • 3. pr ri t s s di Another important discovery emanating from the clinical evaluation of methylnaltrexone and alvimopan is their potential to stimulate bowel activity in healthy volunteers. This attests to the concept that endogenous opioid peptides play a role in reducing bowel function under physiological conditions. As there is evidence that the endogenous opioid system in the gut may be overactive under certain pathological conditions, PRORAs may turn out to be prokinetic drugs in their own right. Preliminary findings of a therapeutic effect in patients with chronic constipation support this contention. It is now important to determine which GI motor disorders will benefit most from the prokinetic potential of methylnaltrexone and alvimopan. in r P d Lt g tin d n a b tri n tio Acknowledgements Work in the author’s laboratory is supported by the Austrian Research Funds, the Austrian Federal Ministry of Education, Science and Culture, the Jubilee Funds of the Austrian National Bank and the Zukunftsfonds Steiermark. HOLZER P: Opioids and opioid receptors in the enteric nervous system: from a problem in opioid analgesia to a possible new prokinetic therapy in humans. Neurosci. Lett. (2004) 361:192-195. Review of the prokinetic potential of opioid receptor antagonists in the gut. DE PONTI F, GIARONI C, COSENTINO M, LECCHINI S, Expert Opin. Investig. Drugs (2007) 16(2) FRIGO G: Adrenergic mechanisms in the control of gastrointestinal motility: from basic science to clinical applications. Pharmacol. Ther. (1996) 69:59-78. 4. FRUHWALD S, HOLZER P, METZLER H: Intestinal motility disturbances in intensive care patients: pathogenesis and clinical impact. Intensive Care Med. (2006) (In Press). b i oh d ite Holzer 5. KROMER W: Endogenous and exogenous opioids in the control of gastrointestinal motility and secretion. Pharmacol. Rev. (1988) 40:121-162. 6. DE LUCA A, COUPAR IM: Insights into opioid action in the intestinal tract. Pharmacol. Ther. (1996) 69:103-115. 7. •• 8. • 9. 10. CAMILLERI M: Alvimopan, a selective peripherally acting µ-opioid antagonist. Neurogastroenterol. Motil. (2004) 17:157-165. Comprehensive review of the clinical potential of alvimopan. rm UK . d Lt STERNINI C, PATIERNO S, SELMER IS, KIRCHGESSNER A: The opioid system in the gastrointestinal tract. Neurogastroenterol. Motil. (2004) 16(Suppl. 2):3-16. Comprehensive review of the distribution of endogenous opioids and opioid receptors in the gut. to h g i r 15. • g COSTA M, BROOKES SJH, STEELE PA, GIBBINS I, BURCHER E, KANDIAH CJ: Neurochemical classification of myenteric neurons in the guinea-pig ileum. Neuroscience (1996) 75:949-967. FURNESS JB: Types of neurons in the enteric nervous system. J. Auton. Nerv. Syst. (2000) 81:87-96. d n a 22. TONINI M, WATERMAN SA, CANDURA SM, COCCINI T, COSTA M: Sites of action of morphine on the ascending excitatory reflex in the guinea-pig small intestine. Neurosci. Lett. (1992) 144:195-198. 24. 25. 27. SARNA SK, LANG IM: Dose- and time-dependent biphasic response to morphine on intestinal migrating myoelectric complex. J. Pharmacol. Exp. Ther. (1985) 234:814-820. CALIGNANO A, MONCADA S, DI ROSA M: Endogenous nitric oxide modulates morphine-induced constipation. Biochem. Biophys. Res. Commun. (1991) 181:889-893. LENARD L, HALMAI V, BARTHO L: Morphine contracts the guinea pig ileal circular muscle by interfering with a nitric oxide mediated tonic inhibition. Digestion (1999) 60:562-566. HIRNING LD, PORRECA F, BURKS TF: µ, but not κ, opioid agonists induce contractions of the canine small intestine ex vivo. Eur. J. Pharmacol. (1985) 109:49-54. Expert Opin. Investig. Drugs (2007) 16(2) ly t c b i oh n tio d ite pr KAUFMAN PN, KREVSKY B, MALMUD LS et al.: Role of opiate receptors in the regulation of colonic transit. Gastroenterology (1988) 94:1351-1356. u b tri ri t s DELGADO-AROS S, CHIAL HJ, CAMILLERI M et al.: Effects of a κ-opioid agonist, asimadoline, on satiation and GI motor and sensory functions in humans. Am. J. Physiol. (2003) 284:G558-G566. 30. STACHER G, STEINRINGER H, SCHNEIDER C et al.: Effects of the prodrug loperamide oxide, loperamide, and placebo on jejunal motor activity. Dig. Dis. Sci. (1992) 37:198-204. 31. SUN WM, READ NW, VERLINDEN M: Effects of loperamide oxide on gastrointestinal transit time and anorectal function in patients with chronic diarrhoea and faecal incontinence. Scand. J. Gastroenterol. (1997) 32:34-38. 32. BEUBLER E, LEMBECK F: Inhibition of stimulated fluid secretion in the rat small and large intestine by opiate agonists. Naunyn-Schmiedeberg’s Arch. Pharmacol. (1979) 306:113-118. 33. TURNBERG LA: Antisecretory activity of opiates in vitro and in vivo in man. Scand. J. Gastroenterol. (1983) 84:79-83. 34. BAUER AJ, SARR MG, SZURSZEWSKI JH: Opioids inhibit neuromuscular transmission in circular muscle of human and baboon jejunum. Gastroenterology (1991) 101:970-976. 35. CHAMOUARD P, KLEIN A, MARTIN E, ADLOFF M, ANGEL F: Regulatory role of enteric κ opioid receptors in human colonic motility. Life Sci. (1993) 53:1149-1156. 36. KOJIMA Y, TAKAHASHI T, FUJINA M, OWYANG C: Inhibition of cholinergic transmission by opiates in ileal myenteric plexus is mediated by κ receptor. Involvement of regulatory inhibitory G protein and calcium N-channels. P WOOD JD, GALLIGAN JJ: Function of opioids in the enteric nervous system. Neurogastroenterol. Motil. (2004) 16(Suppl. 2):17-28. 23. POONYACHOTI S, PORTOGHESE PS, BROWN DR: Characterization of opioid receptors modulating neurogenic contractions of circular muscle from porcine ileum and evidence that δ- and κ-opioid receptors are coexpressed in myenteric neurons. J. Pharmacol. Exp. Ther. (2001) 297:69-77. 29. s di 26. 28. SHAHBAZIAN A, HEINEMANN A, SCHMIDHAMMER H, BEUBLER E, HOLZER-PETSCHE U, HOLZER P: Involvement of µ- and κ-, but not δ-, opioid receptors in the peristaltic motor depression caused by endogenous and exogenous opioids in the guinea-pig intestine. Br. J. Pharmacol. (2002) 135:741-750. Experimental study characterising the role of opioid receptors in the control of peristalsis in the guinea-pig small intestine. 21. fo n fI HOLZER P, LIPPE IT, HEINEMANN A, BARTHO L: Tachykinin NK1 and NK2 receptor-mediated control of peristaltic propulsion in the guinea-pig small intestine in vitro. Neuropharmacology (1998) 37:131-138. rin FURNESS JB: The enteric nervous system. Blackwell Science, Oxford, UK (2006). Comprehensive monography of the organisation, physiology and pathophysiology of the enteric nervous system. 14. 20. FICKEL J, BAGNOL D, WATSON SJ, AKIL H: Opioid receptor expression in the rat gastrointestinal tract: a quantitative study with comparison to the brain. Mol. Brain. Res. (1997) 46:1-8. tin 12. •• BAGNOL D, MANSOUR A, AKIL H, WATSON SJ: Cellular localization and distribution of the cloned µ and κ opioid receptors in rat gastrointestinal tract. Neuroscience (1997) 81:579-591. HOLZER P, SCHICHO R, HOLZER-PETSCHE U, LIPPE IT: The gut as a neurological organ. Wiener Klin. Wochenschr. (2001) 113:647-660. a y p Co 17. 19. SANGER GJ, HOLZER P: Endogenous opioids and the gastrointestinal tract. Semin. Colon Rectal Surg. (2005) 16:197-199. BROOKES SJH: Classes of enteric nerve cells in the guinea-pig small intestine. Anat. Rec. (2001) 262:58-70. 13. STERNINI C, SPANN M, ANTON B et al.: Agonist-selective endocytosis of µ opioid receptor by neurons in vivo. Proc. Natl. Acad. Sci. USA (1996) 93:9241-9246. 18. SANGER GJ, TULADHAR BR: The role of endogenous opiates in the control of gastrointestinal motility: predictions from in vitro modelling. Neurogastroenterol. Motil. (2004) 16(Suppl. 2):38-45. Review of the functional implications of endogenous opioids in the gut. 11. •• 16. 191 Treatment of opioid-induced gut dysfunction J. Pharmacol. Exp. Ther. (1994) 268:965-970. DONNERER J, HOLZER P, LEMBECK F: Release of dynorphin, somatostatin and substance P from the vascularly perfused small intestine of the guinea-pig during peristalsis. Br. J. Pharmacol. (1984) 83:919-925. 37. COSENTINO M, MARINO F, DE PONTI F et al.: Tonic modulation of neurotransmitter release in the guinea-pig myenteric plexus: effect of µ and κ opioid receptor blockade and of chronic sympathetic denervation. Neurosci. Lett. (1995) 194:185-188. 38. 39. 40. 41. •• 45. 192 KROMER W, PRETZLAFF W: In vitro evidence for the participation of intestinal opioids in the control of peristalsis in the guinea-pig small intestine. Naunyn-Schmiedeberg’s Arch. Pharmacol. (1979) 309:153-157. 57. SCHANG JC, DEVROEDE G: Beneficial effects of naloxone in a patient with intestinal pseudoobstruction. Am. J. Gastroenterol. (1985) 80:407-411. 58. HAWKES ND, RHODES J, EVANS BK, RHODES P, HAWTHORNE AB, THOMAS GA: Naloxone treatment for irritable bowel syndrome – a randomized controlled trial with an oral formulation. Aliment. Pharmacol. Ther. (2002) 16:1649-1654. 48. YUAN CS, DOSHAN H, CHARNEY MR et al.: Tolerability, gut effects, and pharmacokinetics of methylnaltrexone following repeated intravenous administration in humans. J. Clin. Pharmacol. (2005) 45:538-546. Clinical study of the kinetics and safety of methylnaltrexone and its potential to stimulate GI transit. 51. UK m r o o t h ig r y 44. 47. 50. f p o C KREEK MJ, SCHAEFER RA, HAHN EF, FISHMAN J: Naloxone, a specific opioid antagonist, reverses chronic idiopathic constipation. Lancet (1983) 1:261-262. CAMILLERI M, MALAGELADA JR, STANGHELLINI V, ZINSMEISTER AR, KAO PC, LI CH: Dose-related effects of synthetic human β-endorphin and naloxone on fed gastrointestinal motility. Am. J. Physiol. (1986) 251:147-154. n fI 43. 56. 49. a •• VAN NUETEN JM, JANSSEN PAJ, FONTAINE J: Unexpected reversal effects of naloxone on the guinea-pig ileum. Life Sci. (1976) 18:803-810. YUAN CS, FOSS JF, MOSS J: Effects of methylnaltrexone on morphine-induced inhibition of contraction in isolated guinea-pig ileum and human intestine. Eur. J. Pharmacol. (1995) 276:107-111. GONENNE J, CAMILLERI M, FERBER I et al.: Effect of alvimopan and codeine on gastrointestinal transit: a randomized controlled study. Clin. Gastroenterol. Hepatol. (2005) 3:784-791. Clinical study of the efficacy of alvimopan to stimulate GI transit and prevent OBD. 42. 46. SCHAUMANN O: Pain, the protective system and combinations with morphine-like effect. Wiener Med. Wochenschr. (1959) 109:78-81. HUGHES J, SMITH TW, KOSTERLITZ HW, FOTHERGILL LA, MORGAN BA, MORRIS HR: Identification of two related pentapeptides from the brain with potent opiate agonist activity. Nature (1975) 258:577-580. CLARK SJ, SMITH TW: The release of met-enkephalin from the guinea-pig ileum at rest and during peristaltic activity. Life Sci. (1983) 33(Suppl. 1):465-468. KROMER W, PRETZLAFF W, WOINOFF R: Opioids modulate periodicity rather than efficacy of peristaltic waves in the guinea-pig ileum in vitro. Life Sci. (1980) 26:1857-1865. MILLION M, FIORAMONTI J, ZAJAC JM, BUENO L: Effects of neuropeptide FF on intestinal motility and temperature changes induced by endotoxin and platelet activating factor. Eur. J. Pharmacol. (1997) 334:67-73. 60. s BARTHO L, HOLZER P, LEMBECK F: Is ganglionic transmission through nicotinic receptors essential for the peristaltic reflex in guinea-pig ileum? Neuropharmacology (1987) 26:1663-1666. 61. HEINEMANN A, HOLZER P: Stimulant action of pituitary adenylate cyclase-activating peptide on normal and drug-compromised peristalsis in the guinea-pig intestine. Br. J. Pharmacol. (1999) 127:763-771. 62. MANARA L, BIANCHETTI A: The central and peripheral influences of opioids on gastrointestinal propulsion. Ann. Rev. Pharmacol. Toxicol. (1985) 25:249-273. 63. MATHESON AJ, NOBLE S: Racecadotril. Drugs (2000) 59:829-835. 64. SCHWARTZ JC: Racecadotril: a new approach to the treatment of diarrhoea. Int. J. Antimicrob. Agents (2000) 14:75-79. 65. SALAZAR-LINDO E, SANTISTEBAN-PONCE J, CHEA-WOO E, GUTIERREZ M: Racecadotril in the treatment of acute watery diarrhea in children. N. Engl. J. Med. (2000) 343:463-467. 66. PRADO D, GLOBAL ADULT RACECADOTRIL STUDY GROUP: A multinational comparison of racecadotril and loperamide in the treatment of acute watery diarrhoea in adults. Scand. J. Gastroenterol. (2002) 37:656-661. Clinical trial comparing the efficacy of loperamide and racecadotril in the management of diarrhoea. i ng t n i r d n a DE WINTER BY, BOECKXSTAENS GE, DE MAN JG, MOREELS TG, HERMAN AG, PELCKMANS PA: Effects of µ- and κ-opioid receptors on postoperative ileus in rats. Eur. J. Pharmacol. (1997) 339:63-67. . YATES DA, SANTOS J, SÖDERHOLM JD, PERDUE MH: Adaptation of stress-induced mucosal pathophysiology in rat colon involves opioid pathways. Am. J. Physiol. (2001) 281:G124-G128. 53. PUIG MM, POL O: Peripheral effects of opioids in a model of chronic intestinal inflammation in mice. J. Pharmacol. Exp. Ther. (1998) 287:1068-1075. 54. POL O, ALAMEDA F, PUIG MM: Inflammation enhances µ-opioid receptor transcription and expression in mice intestine. Mol. Pharmacol. (2001) 60:894-899. Experimental study demonstrating upregulation of µ-opioid receptors in the inflamed gut. 55. ri t s 59. YOSHIDA S, OHTA J, YAMASAKI K et al.: Effect of surgical stress on endogenous morphine and cytokine levels in the plasma after laparoscopoic or open cholecystectomy. Surg. Endosc. (2000) 14:137-140. Expert Opin. Investig. Drugs (2007) 16(2) SANGER GJ, WARDLE KA: Constipation evoked by 5-HT3 receptor antagonism: evidence for heterogeneous efficacy among different antagonists in guinea-pigs. J. Pharm. Pharmacol. (1994) 46:666-670. di • n tio u b tri d Lt • pr BROWN NJ, RUMSEY RDE, BOGENTOFT C, READ NW: The effect of an opiate receptor antagonist on the ileal brake mechanism in the rat. Pharmacology (1993) 47:230-236. P 52. ly t c b i oh d ite Holzer YUAN CS, FOSS JF, O’CONNOR M, MOSS J, ROIZEN MF: Gut motility and transit changes in patients receiving long-term methadone maintenance. J. Clin. Pharmacol. (1998) 38:931-935. 68. MANARA L, BIANCHI G, FERRETTI P, TAVANI A: Inhibition of gastrointestinal transit by morphine in rats results primarily from direct drug action on gut opioid sites. J. Pharmacol. Exp. Ther. (1986) 237:945-949. 69. • a 74. BAUER AJ, BOECKXSTAENS GE: Mechanisms of postoperative ileus. Neurogastroenterol. Motil. (2004) 16(Suppl. 2):54-60. Review of the pathophysiological mechanisms underlying postoperative ileus. f • n fI to h rig 75. m r o UK . HERNDON CM, JACKSON KC, HALLIN PA: Management of opioid-induced gastrointestinal effects in patients receiving palliative care. Pharmacotherapy (2002) 22:240-250. 76. GALLIGAN JJ, VANNER S: Basic and clinical pharmacology of new motility promoting agents. Neurogastroenterol. Motil. (2005) 17:643-653. 77. DONNER B, ZENZ M, STRUMPF M, RABER M: Long-term treatment of cancer FOSS JF, O’CONNOR MF, YUAN CS, MURPHY M, MOSS J, ROIZEN MF: Safety and tolerance of methylnaltrexone in healthy humans: a randomized, placebo-controlled, intravenous, ascending-dose, pharmacokinetic study. J. Clin. Pharmacol. (1997) 37:25-30. GREENWOOD-VAN MEERVELD B, GARDNER CJ, LITTLE PJ, HICKS GA, DEHAVEN-HUDKINS DL: Preclinical studies of opioids and opioid antagonists on gastrointestinal function. Neurogastroenterol. Motil. (2004) 16(Suppl. 2):46-53. 89. JURNA I, KAISER R, KRETZ O, BALDAUF J: Oral naloxone reduces constipation but not antinociception from oral morphine in the rat. Neurosci. Lett. (1992) 142:62-64. 90. SYKES NP: An investigation of the ability of oral naloxone to correct opioid-related constipation in patients with advanced cancer. Palliat. Med. (1996) 10:135-144. d n a in r P 83. CHESKIN LJ, CHAMI TN, JOHNSON RE, JAFFE JH: Assessment of nalmefene glucuronide as a selective gut opioid antagonist. Drug Alcohol Depend. (1995) 39:151-154. 84. YUAN CS, ISRAEL RJ: Methylnaltrexone, a novel peripheral opioid receptor antagonist for the treatment of opioid side effects. Expert Opin. Investig. Drugs (2006) 15(5):541-552. Comprehensive review of the experimental and clinical pharmacology and toxicology of methylnaltrexone. •• 85. 86. • YUAN CS, FOSS JF, OSINSKI J, TOLEDANO A, ROIZEN MF, MOSS J: The safety and efficacy of oral methylnaltrexone in preventing morphine-induced delay in oral-cecal transit time. Clin. Pharmacol. Ther. (1997) 61:467-475. YUAN CS, FOSS JF, O’CONNOR M, TOLEDANO A, ROIZEN MF, MOSS J: Methylnaltrexone prevents morphineinduced delay in oral-cecal transit time without affecting analgesia: a double-blind randomized placebo-controlled trial. Clin. Pharmacol. Ther. (1996) 59:469-475. Clinical trial demonstrating the efficacy of methylnaltrexone in preventing OBD. Expert Opin. Investig. Drugs (2007) 16(2) ly t c •• 91. •• 92. •• pr MURPHY DB, SUTTON JA, PRESCOTT LF, MURPHY MB: Opioid-induced delay in gastric emptying: a peripheral mechanism in humans. Anesthesiology (1997) 87:765-770. n tio u b tri i oh ri t s YUAN CS, WEI G, FOSS JF, O’CONNOR M, KARRISON T, OSINSKI J: Effects of subcutaneous methylnaltrexone on morphine-induced peripherally mediated side effects: a double-blind randomized placebo-controlled trial. J. Pharmacol. Exp. Ther. (2002) 300:118-123. Clinical study demonstrating the efficacy of subcutaneous methylnaltrexone in controlling OBD. YUAN CS, FOSS JF, O’CONNOR M et al.: Effects of enteric-coated methylnaltrexone in preventing opioid-induced delay in oral-cecal transit time. Clin. Pharmacol. Ther. (2000) 67:398-404. Clinical study addressing the efficacy of oral methylnaltrexone in preventing OBD. YUAN CS, FOSS JF, O’CONNOR M et al.: Methylnaltrexone for reversal of constipation due to chronic methadone use: a randomized, controlled trial. JAMA (2000) 283:367-372. Clinical study demonstrating the efficacy of intravenous methylnaltrexone in preventing OBD. 93. YUAN CS, FOSS JF: Oral methylnaltrexone for opioid-induced constipation. JAMA (2000) 284:1383-1384. 94. FUKUDA H, SUENAGA K, TSUCHIDA D et al.: The selective µ opioid receptor antagonist, alvimopan, improves delayed GI transit of postoperative ileus in rats. Brain Res. (2006) 1102:63-70. Experimental study of the efficacy of alvimopan in ameliorating postoperative ileus. •• d ite b s di MEISSNER W, SCHMIDT U, HARTMANN M, KATH R, REINHART K: Oral naloxone reverses opioid-associated constipation. Pain (2000) 84:105-109. g it n d Lt LUCKEY A, LIVINGSTON E, TACHE Y: Mechanisms and treatment of postoperative ileus. Arch. Surg. (2003) 138:206-214. Review of the pathophysiological mechanisms underlying postoperative ileus. 73. 88. 79. 82. CALI RL, MEADE PG, SWANSON MS, FREEMAN C: Effect of morphine and incision length on bowel function after colectomy. Dis. Colon Rectum (2000) 43:163-168. 72. KOTAKE AN, KUWAHARA SK, BURTON E, McCOY CE, GOLDBERG LI: Variations in demethylation of N-methylnaltrexone in mice, rats, dogs, and humans. Xenobiotica (1989) 19:1247-1254. ALLAN L, HAYS H, JENSEN NH et al.: Randomised crossover trial of transdermal fentanyl and sustained release oral morphine for treating chronic non-cancer pain. Br. Med. J. (2001) 322:1154-1158. 81. RUSSELL J, BASS P, GOLDBERG LI, SCHUSTER CR, MERZ H: Antagonism of gut, but not central effects of morphine with quaternary narcotic antagonists. Eur. J. Pharmacol. (1982) 78:255-261. 71. 87. 78. 80. BIANCHI G, FIOCCHI R, TAVANI A, MANARA L: Quaternary narcotic antagonists’ relative ability to prevent antinociception and gastrointestinal transit inhibition in morphine-treated rats as an index of peripheral selectivity. Life Sci. (1982) 30:1875-1883. 70. y p Co pain with transdermal fentanyl. J. Pain Symptom Manage. (1998) 15:168-175. FOSS JF: A review of the potential role of methylnaltrexone in opioid bowel dysfunction. Am. J. Surg. (2001) 182(Suppl.):19S-26S. 67. 193 Treatment of opioid-induced gut dysfunction SCHMIDT WK: Alvimopan (ADL 8-2698) is a novel peripheral opioid antagonist. Am. J. Surg. (2001) 182:27S-38S (Supplement). Review of the early development of alvimopan for the management of OBD. 95. • LESLIE JB: Alvimopan for the management of postoperative ileus. Ann. Pharmacother. (2005) 39:1502-1510. Review of the usefulness of alvimopan in the management of postoperative ileus. 96. •• NEARY P, DELANEY CP: Alvimopan. Expert Opin. Investig. Drugs (2005) 14(4):479-488. Comprehensive review of the experimental and clinical pharmacology and toxicology of alvimopan. 97. •• ZIMMERMAN DM, GIDDA JS, CANTRELL BE, SCHOEPP DD, JOHNSON BG, LEANDER JD: Discovery of a potent, peripherally selective trans-3,4-dimethyl-4-(3hydroxyphenyl)piperidine opioid antagonist for the treatment of gastrointestinal motility disorders. J. Med. Chem. (1994) 37:2262-2265. 98. LIU SS, HODGSON PS, CARPENTER RL, FRICKE JR: ADL 8-2698, a trans-3,4-dimethyl4-(3-hydroxyphenyl) piperidine, prevents gastrointestinal effects of intravenous morphine without affecting analgesia. Clin. Pharmacol. Ther. (2001) 69:66-71. 99. 100. PAULSON DM, KENNEDY DT, DONOVICK RA et al.: Alvimopan: an oral, peripherally acting, µ-opioid receptor antagonist for the treatment of opioid-induced bowel dysfunction – a fo rm n fI UK •• a 21-day treatment-randomized clinical trial. J. Pain (2005) 6:184-192. Clinical study addressing the effect of prolonged intake of alvimopan to prevent OBD. 101. TAGUCHI A, SHARMA N, SALEEM RM • 105. VISCUSI ER, GOLDSTEIN S, et al.: Selective postoperative inhibition of gastrointestinal opioid receptors. N. Engl. J. Med. (2001) 345:935-940. Clinical trial reporting on the therapeutic efficacy of alvimopan in postoperative ileus. WITKOWSKI T et al.: Alvimopan, a peripherally acting µ-opioid receptor antagonist, compared with placebo in postoperative ileus after major abdominal surgery: results of a randomized, double-blind, controlled study. Surg. Endosc. (2006) 20:64-70. Phase III trial evaluating the efficacy and safety of alvimopan in the management of postoperative ileus. ly t c 102. WOLFF BG, MICHELASSI F, •• GERKIN TM et al.; ALVIMOPAN POSTOPERATIVE ILEUS STUDY GROUP: Alvimopan, a novel peripherally acting µ opioid antagonist. Results of a multicenter, randomized, double-blind, placebo-controlled, Phase III trial of major abdominal surgery and postoperative ileus. Ann. Surg. (2004) 240:728-735. Phase III trial evaluating the efficacy and safety of alvimopan in the management of postoperative ileus. nd a 103. DELANEY CP, WEESE JL, HYMAN NH ng et al.; ALVIMOPAN POSTOPERATIVE ILEUS STUDY GROUP: Phase III trial of alvimopan, a novel, peripherally acting, µ opioid antagonist, for postoperative ileus after major abdominal surgery. Dis. Colon Rectum (2005) 48:1114-1125. Phase III trial evaluating the efficacy and safety of alvimopan in the management of postoperative ileus. i t n i r P •• . d Lt 104. HERZOG TJ, COLEMAN RL, GUERRIERI JP et al.: A double-blind, randomized, placebo-controlled Phase III study of the safety of alvimopan in patients who undergo simple total abdominal o t h ig r y p o C 194 •• hysterectomy. Am. J. Obstet. Gynecol. (2006) 195:445-453. Phase III trial evaluating the efficacy and safety of alvimopan in the management of postoperative ileus. Expert Opin. Investig. Drugs (2007) 16(2) •• pr ri t s 106. TAN EK, CORNISH J, DARZI AW, TEKKIS PP: Meta-analysis: alvimopan vs. placebo in the treatment of post-operative ileus. Aliment. Pharmacol. Ther. (2006) (In Press). Meta-analysis confirming a significant beneficial effect of alvimopan in the treatment of postoperative ileus. u b tri is •• d n tio b i oh 107. GARNETT W, KELLEHER DL, HICKMOTT F et al.: Alvimopan (ALV) shortens whole bowel transit time in adults with chronic constipation (CC). Gastroenterology (2004) 126:A643. Affiliation Peter Holzer PhD, Professor Research Unit of Translational Neurogastroenterology, Institute of Experimental and Clinical Pharmacology, Medical University of Graz, Universitätsplatz 4, A-8010 Graz, Austria Tel: +43 316 380 4500; Fax: +43 316 380 9645; E-mail: [email protected] d ite