Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Nervous system network models wikipedia , lookup
Neuroplasticity wikipedia , lookup
Multielectrode array wikipedia , lookup
Neural engineering wikipedia , lookup
Neuroregeneration wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Haemodynamic response wikipedia , lookup
Adult neurogenesis wikipedia , lookup
Metastability in the brain wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Optogenetics wikipedia , lookup
Development of the nervous system wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuroanatomy wikipedia , lookup
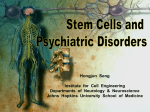
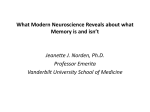
Journal of Neuropathology and Experimental Neurology Copyright q 2003 by the American Association of Neuropathologists Vol. 62, No. 8 August, 2003 pp. 801 811 From Cell Death to Neuronal Regeneration: Building a New Brain after Traumatic Brain Injury NICOLAS C. ROYO, PHD, JOOST W. SCHOUTEN, MD, CARL T. FULP, BA, BS, SAORI SHIMIZU, MD, PHD, NIKLAS MARKLUND, MD, PHD, DAVID I. GRAHAM, MB, PHD, AND TRACY K. MCINTOSH, PHD Abstract. During the past decade, there has been accumulating evidence of the involvement of passive and active cell death mechanisms in both the clinical setting and in experimental models of traumatic brain injury (TBI). Traditionally, research for a treatment of TBI consists of strategies to prevent cell death using acute pharmacological therapy. However, to date, encouraging experimental work has not been translated into successful clinical trials. The development of cell replacement therapies may offer an alternative or a complementary strategy for the treatment of TBI. Recent experimental studies have identified a variety of candidate cell lines for transplantation into the injured CNS. Additionally, the characterization of the neurogenic potential of specific regions of the adult mammalian brain and the elucidation of the molecular controls underlying regeneration may allow for the development of neuronal replacement therapies that do not require transplantation of exogenous cells. These novel strategies may represent a new opportunity of great interest for delayed intervention in patients with TBI. Key Words: Apoptosis; Cell death; Necrosis; Neurogenesis; Replacement therapy; Transplantation; Traumatic brain injury. INTRODUCTION Ongoing and progressive cell death after a single initial mechanical injury is one of the hallmark features of the pathophysiology of traumatic brain injury (TBI). Evidence for the involvement of both passive and active cell death mechanisms has been documented in both the clinical setting and in experimental models of TBI developed to understand the mechanisms of this progressive and diffuse cell loss. Traditionally, treatment of TBI consists of the prevention of cell death using acute pharmacological therapy, but to date, this strategy remains only partially effective. In addition to the prevention of cell death, a more novel therapeutic approach may be to replace lost cells in order to restore function. Cell replacement therapies, including cellular transplantation and manipulation of the endogenous neurogenic potential of the brain, may offer an opportunity for delayed treatment of TBI. NECROTIC CELL DEATH FOLLOWING EXPERIMENTAL TBI Neurodegenerative cells exhibiting necrotic features under light and electron microscopy are observed within the first hour after fluid percussion (FP) brain injury in rats (1). Morphologically, necrotic cell death associated From the Head Injury Center, Department of Neurosurgery (NCR, JWS, CTF, NM, TKM), University of Pennsylvania, and the Veterans Administration Medical Center (TKM), Philadelphia, Pennsylvania; University Department of Neuropathology, Institute of Neurological Sciences (DIG), Southern General Hospital, Glasgow, United Kingdom. Correspondence to: Tracy K. McIntosh, PhD, Department of Neurosurgery, 105C Hayden Hall, 3320 Smith Walk, Philadelphia, PA 191046074. E-mail: [email protected] This work was supported, in part, by grants from the National Institute of Health National Institute of Neurological Disorders and Stroke (P50-NS08803 and RO1-NS40978), the National Institute of General Medical Sciences (RO1-GM34690), a Merit Review grant from the Veterans Administration and a Veterans Administration-DOD consortium Merit Review grant. with TBI can be differentiated from apoptosis and is generally characterized by a loss of membrane integrity, early organelle damage, cellular swelling, mitochondrial swelling, and uncontrolled cell lysis (Fig. 1A). In addition, necrosis induces an inflammatory response in brain tissue, resulting in secondary damage. Neuronal cell death has been demonstrated in a variety of experimental models of TBI using Nissl (1, 2), acid fuchsin (1, 2), silver staining (1), TUNEL (3), and Fluoro-Jade staining (4) after TBI. Following experimental TBI, Cortez et al (2) observed necrotic neurons in the injured cortex, CA1, CA2, and CA3 regions of the hippocampus and granule cells in the dentate gyrus (DG) using acid fuchsin staining at acute time points (between 10 min and 24 h), followed by a significant reduction of neurons in the injured pyramidal cell layer of the hippocampus and in the ventral and lateral posterior thalamus in the more chronic postinjury phase (between 1 and 4 weeks) (2). Intensely acidophilic neurons were observed that appeared to have undergone necrosis, that is, cells were shrunken and eosinophilic. Others have observed dystrophic neurons after controlled cortical impact (CCI) injury in the rat localized to the DG, hippocampal CA1 and CA3 regions, amygdala, entorhinal and piriform cortices, and thalamic and hypothalamic regions (5). Following experimental TBI, neuronal cell body and dendrites are often stained by silver stains and appear as dark or argyrophilic neurons (6). Although necrotic neurons detected by silver staining appeared in a similar spatial pattern as those detected by acid fuchsin, silver staining also detected microglia, astrocytes, and cellular debris. More recently, Fluoro-Jade, an acidic dye that is thought to stain the same substrates as acid fuchsin, has been used as a marker of degenerating neuronal cell bodies and their processes. After FP brain injury in rat, the regional distribution of FluoroJade-labeled neurons corresponded to a similar pattern of silver and TUNEL staining (4). Severely injured neurons 801 802 ROYO ET AL characteristics inconsistent with the morphology they exhibit at a given time point (e.g. DNA laddering patterns suggestive of apoptosis), while having ultrastructural features consistent with a necrotic phenotype. It has been suggested that when sufficient sources of cellular energy are available, cell death will occur via a process consistent with the apoptotic morphology, but when energy is lacking, necrotic cell death will occur (7). Thus, the constant balance between energy supply and consumption during the death continuum is a critical factor in determining whether cell death ultimately becomes an active (apoptotic) or passive (necrotic) process. APOPTOTIC CELL DEATH FOLLOWING EXPERIMENTAL TBI Fig. 1. Two types of TUNEL-positive cells were detected under electron microscopy after FP brain injury in rat. Type I: necrotic cell death is characterized by a loss of membrane integrity, early organelle damage, cellular swelling, mitochondrial swelling, and uncontrolled cell lysis (A). Type II: apoptotic cell death is characterized by a condensation and margination of chromatin, activation of an endonuclease that degrades nuclear DNA, and cellular fragments containing intact organelles (B). Reprinted with permission from the American Society for Investigative Pathology (8). appeared in the cortex and hippocampus within 3 h after injury and were most evident at 24 h postinjury. In the thalamus, a delayed peak of necrotic neurons was observed at 7 days after injury and remained until 28 days. At later time points, these Fluoro-jade-positive cells exhibited deterioration of the neuronal cell body and processes. Traditionally, necrosis was believed to be the primary cause of cell death following TBI. However, distinguishing between apoptosis and necrosis within a particular group of cells at a particular time point after injury is often misleading since cells appear to move freely between the two morphologies over the continuum of the death processes. Cells may, in fact, assume biochemical J Neuropathol Exp Neurol, Vol 62, August, 2003 Apoptosis is the morphological manifestation of cells that die by programmed cell death during CNS development. The defining characteristics of apoptosis include condensation and margination of the chromatin, activation of an endonuclease that degrades nuclear DNA, and the formation of cellular fragments containing intact organelles (Fig. 1B). Using combined in situ DNA nick end labeling and DNA gel electrophoresis, numerous studies have detected internucleosomal DNA fragmentation following experimental TBI. After FP brain injury in rats, TUNEL staining at acute time points (12–72 h) yielded both type I (necrotic) and type II (apoptotic) populations of TUNEL(1) cells localized to the subcortical white matter, DG, and hippocampal CA3 region, in addition to the cortical site of injury (8). Consistent with these results, an apoptotic-like internucleosomal DNA gel electrophoresis fragmentation pattern (185–200 bp) was observed within tissue isolated from the injured cortex and hippocampus and this degree of fragmentation directly correlated with the severity of the injury (8). Colicos et al (5) subsequently observed that at 24 h following CCI injury in rats, a subpopulation of cells within the DG, CA1, and CA3 subfields exhibited apoptotic-like morphology. Conti et al (9) observed a biphasic increase of apoptotic cells in the injured cortex, with an initial peak at 24 h that colabeled with markers for neurons and oligodendrocytes, and a secondary peak at 1 week following injury. Increased numbers of apoptotic cells were observed up to 8 weeks postinjury. Within the hippocampus, apoptotic neurons were significantly increased as early as 12 h, with a peak at 48 h, and returning to control levels by 4 weeks. By 1 week following injury, apoptotic neurons were observed in the thalamus, with a significant peak at 2 weeks postinjury. Additional biochemical evidence exists to support the observation that DNA fragmentation is a result of the activation of endonucleases. The stress-activated kinases, including the p38 mitogen-activated protein kinase (MAPK) and Jun N-terminal kinase (JNK), are activated in response to DNA damage (10). However, the question of whether JNK or p38 plays CELL REPLACEMENT THERAPY FOR BRAIN TRAUMA Fig. 2. 803 Apoptotic cell death pathways. a role in cell death following TBI remains highly controversial. Following FP injury in rats, immunoreactivity for phospho-JNK, but not phospho-p38, has been observed to significantly increase within intact pyramidal cells of the injured hippocampus as early as 5 min and return to baseline expression levels at 1 h, while phospho-ERK was also significantly increased in hippocampal regions vulnerable to TBI (11). Recently, a more prolonged activation (up to 72 h) of ERK1/2 and JNK was reported in a similar model (12). In contrast, following CCI injury, phospho-ERK and p-p38, but not p-JNK, are transiently increased within the injured cortex at acute time points, and administration of an ERK kinase inhibitor, but not a p38/JNK kinase inhibitor, resulted in decreased traumatic lesion volume (13). However, Dash et al (14) reported a significant enhancement of loss of MAP-2-immunoreactivity within the CA3 subfield of the hippocampus upon administration of an ERK kinase inhibitor. The caspase family of proteins, of which 14 are now known in mammals, are interleukin-1b-converting enzyme (ICE)-like, aspartate-specific proteases, synthesized as procaspases that are cleaved at active Asp-X sites, generating a large and small subunit, which together constitute the active protease. Caspases can be categorized into 2 broad groups: initiator caspases, which generally contain large prodomains, autoactivate, and are thought to be involved in the initiation of the apoptotic response, and executioner caspases, which generally contain short prodomains and appear to be activated by initiator caspases. The activation of effector caspases, particularly caspase3, appears to represent the cell’s commitment to die and the convergence of numerous signaling pathways (Fig. 2). Activation of caspase-3 has been observed after TBI, and intracerebroventricular administration of the caspase3 inhibitor z-DEVD-fmk was shown to reduce DNA cleavage and TUNEL staining and to improve neurological outcome after FP injury (15). Cytochrome c-mediated pathways such as cytochrome c and activated caspase-3 are readily detected in damaged axons following the impact acceleration model of TBI in rats (16). Following experimental TBI, caspase-8 mRNA and protein rapidly increase within neurons, astrocytes, and oligodendrocytes in the cortex and hippocampus. It is now clear that the homeostatic mechanisms that are involved in the activation of caspases are far more complex than the simple regulation of their cleavage. The Bcl-2 family of protein plays a critical role in the intracellular apoptotic signaling transduction cascade. Following CCI injury with induced hypoxia in rats, bcl-2 expression has been shown to increase primarily within TUNEL(2) neurons, and to a lesser extent in the glia, the ipsilateral cortex, DG, and CA3 region, beginning at J Neuropathol Exp Neurol, Vol 62, August, 2003 804 ROYO ET AL 8 h and continuing up to 7 days (17). Increased expression of Bcl-2 protein, but not Bcl-XL or Bax, within neurons was also observed in the cortical regions of excised tissue from patients sustaining severe TBI (18). Recent evidence has suggested the existence of a caspase-independent pathway of apoptosis involving the release of apoptosis-inducing factor (AIF) from the mitochondria. In dying cells, AIF relocates from the mitochondria to the nucleus where its DNA binding activity is thought to mediate chromatin condensation and large-scale DNA fragmentation (19). CELL DEATH FOLLOWING HUMAN TBI The nature and distribution of the pathological cell death after blunt head injury in man has been partially determined (20). These include surface contusions, a focal form of TBI that occurs at the moment of injury, traumatic axonal injury (TAI), and subsequently hypoxicischemic damage, which are diffuse (multifocal) forms of TBI. Microscopic studies of patients dying after TBI have identified necrosis as the principal type of death by which cells die in the acute phase following injury (21), although apoptosis, initiated early in the course of clinical TBI, can persist for many weeks or months postinjury (22). In man, initial studies were undertaken on surface contusions either from material that had been surgically excised from head-injured patients admitted to a neurosurgical intensive trauma unit (18) or sampled at autopsy (23). In the latter study, frontal lobe contusions from 18 patients who survived 6 h to 10 days were stained by the TUNEL histochemical technique for evidence of DNA fragmentation. TUNEL(1) cells were found in both the neocortex and in the associated white matter. First seen in grey and white matter at 5 h postinjury, TUNEL(1) cells peaked in number between 25 h and 48 h and were still identifiable at 10 days postinjury. Quantitation showed that there were fewer TUNEL(1) cells in grey than in white matter and that most of these were neurons with the morphological features of necrosis, i.e. type I or nonapoptotic cells (8). However, the microscopic features of some of the TUNEL(1) neurons and of glial cells in both grey and white matter were those of apoptosis—the type II cell (8). Apoptosis was not observed in age-sexmatched uninjured controls. The morphology and immunohistochemical profile of the TUNEL(1) cells indicated that in the acute phase after TBI, some of these strongly resembled oligodendroglia, whereas by 5 to 10 days after injury, many appeared as macrophages. Further studies on the hippocampus, the cingulate, parasagittal and the insular cortex, and the associated white matter from patients who had died 5 h to 10 days after blunt TBI showed that TUNEL(1) cells were present in both grey and white matter, and that their numbers increased between 5 h and 24 h before peaking between 24 h and 48 h and were still present at 10 days postinjury (23). J Neuropathol Exp Neurol, Vol 62, August, 2003 Quantitation showed that in short surviving cases there were more TUNEL(1) cells in grey than white matter corresponding to necrotic cell change, whereas with increasing survival, fewer TUNEL(1) cells in grey matter were visible and more were seen in the corpus callosum, parasagittal white matter, the external and extreme capsules, and white matter of the hippocampus. Type I cells again predominated in the acute post-traumatic period and were strongly associated with ischemic neurons, whereas type II cells with the morphology of neurons and glia were seen at all survival periods. By 5 to 10 days postinjury, most of the type II cells were in the white matter and resembled macrophages. The experimental literature suggests that cellular changes initiated by acute head injury might persist and indeed be progressive. Such evidence combined with analogous clinical observations indicates that in addition to the necrosis induced at the time of acute TBI, there may also be continuing or progressive loss of cells via apoptosis over the ensuing months. Additional studies using the TUNEL technique for evidence of DNA fragmentation were performed in multiple brain areas in 18 patients who survived for up to 12 months after head injury. Compared with matched controls, more TUNEL(1) cells were observed in the TBI patients and quantitative studies showed that these were predominantly localized to the white matter. Some of these cells had the morphological features of apoptosis and routine H&E staining and double labeling immunohistochemical studies indicated that most of these cells were microglia or macrophages (22). Similar changes were reported in patients who survived in a vegetative state for many months or years after TBI (Wilson et al, personal communication), and age at time of injury did not appear to influence the amount of DNA fragmentation in the brains of fatal cases of TBI aged 4 to 89 years compared with controls (24). Taken together, these studies in autopsy material from patients after TBI suggest that TUNEL(1) cells are present in both acutely injured material, but also in the white matter of patients whose TBI was months or years earlier. Most of the TUNEL(1) cells appeared as microglia/macrophages and were thought to reflect the prolonged time course of the macrophage response of Wallerian degeneration. Evidence that oligodendrocytes can undergo apoptosis days or even weeks after injury raises the possibility that the death of oligodendroglia by apoptosis may contribute to demyelination of intact axons (25). CELL REPLACEMENT STRATEGIES Cell Transplantation after TBI Restorative and regenerative strategies that have focused on replacement or repair of dysfunctional and dead cells have received little attention in the treatment of TBI. CELL REPLACEMENT THERAPY FOR BRAIN TRAUMA Cellular transplantation is one option to repair the injured CNS, aiming at replacing the function of cells lost to injury. Initially, neural transplantation was developed as a potential therapy for neurodegenerative diseases such as Parkinson disease (PD) and Huntington disease (HD), and although cellular transplantation has begun to be evaluated in models of traumatic CNS injury, the variability in anatomical structures involved and cell types to be replaced is one of the major challenges of replacement therapy for TBI compared to other neurodegenerative diseases. Early studies initially evaluated the use of fetal tissue in models of PD, where grafts of fetal mesencephalic tissue, rich in dopaminergic neurons, were shown to reinnervate the denervated rat striatum, synthesize and release dopamine, and ameliorate motor symptoms. Fetal cortical tissue that was transplanted into the injured cortex of nonimmunosuppressed adult rats subjected to FP brain injury survived best when transplanted between 2 days and 2 weeks postinjury (26), and was shown to ameliorate post-traumatic hippocampal cell death (27). Transplantation at 4 weeks postinjury resulted in reduced graft integration as measured by acetylcholinergic fibers crossing the graft-host interface, most likely due to increased glial scar formation at later postinjury time-points. Recovery of both cognitive and motor function was observed subsequently after transplantation of fetal rat cortical tissue into the injured cortex in combination with nerve growth factor (NGF) infusion after lateral FP TBI in nonimmunosuppressed adult rats (28). Although promising results have been obtained transplanting fetal tissue in clinical trials for PD, technical and ethical concerns in the use of fetal tissue as source for transplantation have been raised, and alternative sources for cellular transplantation are currently under investigation. While multipotent stem and progenitor cells have been shown to differentiate into the 3 major neural cell types in vitro, their fate after transplantation in vivo in the adult brain depends on both cell intrinsic features and the host environment. The age of the host, the location of transplantation, and the factors and signals generated by the injured CNS all seem to influence transplanted stem and progenitor cells as well as endogenous neural stem cells, possibly limiting their multipotentiality and forcing them to differentiate into predominantly glial lineages (29). When the goal of cellular transplantation is strictly neuronal replacement, one option is the transplantation of a homogenous population of terminally differentiated postmitotic neurons such as NT2N cells, commercially known as hNT cells or LBS neurons. These cells are derived from a human embryonal teratocarcinoma line (NT2 cell line) by in vitro retinoic acid treatment and are a safe and well-characterized source of human neurons (30). These cells resemble region-specific neuronal morphology at the location of transplantation 805 and possess many of the key features of mature human neurons, including the development of appropriate axonal and dendritic polarity, expression of cytoskeletal proteins, synaptophysin expression, and synaptic vesicle formation. Positive behavioral and histological results in experimental models of focal ischemia recently resulted in the initiation of the first phase I neuronal transplantation trial in 12 patients with chronic basal ganglia infarction (31). The efficacy of the transplantation to improve stroke-related neurological deficits was suggestive of a trend towards improved scores in 4 patients receiving the highest number of cells (6 million), and improved metabolism in the area of the stroke as shown by fluorodeoxyglucose positron emission tomography (32). Philips et al (33) transplanted hNT cells into the injured cortex of nonimmunosuppressed adult rats 24 h after FP brain injury and observed viable hNT transplants up to 4 weeks, without attenuation of post-traumatic neuromotor deficits. The presence of activated macrophages and microglia at 4 weeks post-transplantation suggested a variable degree of graft rejection. More recently, transplantation of hNT cells transduced ex vivo to express NGF into the medial septum following CCI injury in mice attenuated long-term cognitive dysfunction and protected the NGF responsive cholinergic neurons of the septo-hippocampal pathway (34). As another source of cells for transplantation, multipotential immortalized stem and progenitor cell lines combine the advantages of cultured cells (unlimited expansion in cultures and the potential to be genetically manipulated in vitro) with the ability to give rise to multiple lineages. Three immortalized cell lines (i.e. HiB5, MHP36, and C17.2) have been transplanted in experimental models of TBI. The HiB5 cells are conditionally immortalized progenitor cells derived from an embryonic (E16) rat hippocampus and have been shown to differentiate into neurons and glia when transplanted into the neonatal hippocampus, cerebellum, and cortex, or into the adult striatum. In rats subjected to FP brain injury, HiB5 cells transduced to secrete NGF (HiB5-NGF) were transplanted into 3 sites surrounding the injured cortex 24 h after injury (35). Braininjured animals receiving either the HiB5-NGF cells or untransduced HiB5 cells showed a similar improvement in neuromotor function and spatial learning. However, hippocampal cell death was significantly reduced only in the HiB5-NGF-engrafted group (35). Although engrafted progenitor or stem cells are likely to secrete various trophic factors that can contribute to plasticity, regeneration, and neuroprotection, the transplantation of cells transduced to produce NGF (e.g. hNT cells and the HiB5 cells described above or fetal tissue transplanted in combination with NGF infusion [28]) seems to have distinct advantages over cell engraftment alone. J Neuropathol Exp Neurol, Vol 62, August, 2003 806 ROYO ET AL The use of transplanted migrating cells will allow for long-term expression and diffuse delivery of neuroprotective factors and may have a greater potential to integrate with the host tissue. In addition, autocrine and paracrine effects of the expressed neurotrophic factors might be important in increasing graft survival. The MHP36 cells are conditionally immortalized cells derived from E14 hippocampal neuro-epithelium of the H-2Kb-tsA58 transgenic mouse and have the ability to self-renew and differentiate into neurons, astrocytes, and oligodendrocytes. When transplanted contralateral into a focal ischemic infarct, cells migrated to the cortex, striatum, and corpus callosum of the injured hemisphere, resulting in recovery of motor function (36). Transplantation of MHP-36 cells into the injured cortex of adult immunosuppressed rats 48 h after FP TBI significantly improved cognition by 16 weeks postinjury (P. M. Lenzlinger et al, personal communication). Finally, the clonal multi-potent C17.2 progenitor is derived from the external germinal layer of the neonatal murine cerebellum immortalized by retroviral transduction of the avian myc gene. Transplantation of C17.2 cells in the newborn mouse brain resulted in widespread engraftment in a cytoarchitecturally appropriate, nontumorigenic manner and differentiated into neuronal and glial cells (37). In mice subjected to CCI injury, transplantation of C17–2 cells 3 days after injury significantly improved motor function over a 12-week period. By 12 weeks postinjury, C17–2 cells expressed 60% neuronal and 40% astrocytic markers when transplanted ipsilateral to the lesion, whereas after contralateral transplantation only neuronal markers were observed (38). A stem cell is an undifferentiated cell (i.e. lacking antigenic markers typical of mature cells), displaying significant proliferation potential in combination with the potential to give rise to differentiated cells through asymmetric division. Embryonic stem cells are totipotent cells derived from the inner cell mass of the early blastocyst phase and can be propagated in vitro before transplantation. Following intracerebroventricular transplantation into the naı ¨ve E16-E18 embryonic brain, embryonic stem cells can enter and integrate throughout the neuraxis and differentiate into neurons, astrocytes, and oligodendrocytes, suggesting that they retain the entire developmental program of neural stem cells. In adult animals, neural stem cells exist throughout life and can be isolated from the walls of the ventricular system of the adult CNS, as well as from the hippocampus. Embryo-derived neural stem cells have been transplanted into unilateral striatum or the injury cavity, with or without an injectable fibronectin-based scaffold, 1 week after CCI injury in mice (39). Cells seeded in the scaffold and transplanted survived better and after 1 week were found lining the injury cavity. By 3 months postinjury, the majority of the cells had migrated towards the hippocampus, suggesting that J Neuropathol Exp Neurol, Vol 62, August, 2003 transplant location and environment may play an important role in neural stem cell graft survival and integration after experimental TBI (39). To date, studies involving transplantation of adult-derived neural stem cells or embryonic stem cells into the traumatically injured brain have not been performed. One exciting, albeit controversial discovery is the possibility that bone marrow-derived cells, either hematopoietic stem cells or mesenchymal stem cells, may be able to give rise to neural and glial cells when transplanted into the adult CNS (40). Recently, mesenchymal stem cells have been shown to possess the ability to express neuronal and glial markers in vitro. When transplanted into the naive adult rat CNS, these cells migrate throughout the brain and lose their immunoreactivity for mesenchymal markers and express neuronal and glial markers at 12 and 45 days post-transplantation. In rodent models of focal ischemia, intra-parenchymal, intravenous, and intra-arterial administration of bone marrowderived cells or whole bone marrow has been reported to attenuate postischemic neurological deficits, with or without reduction of lesion volume. In rats subjected to CCI injury, mesenchymal stem cells administered 24 h postinjury via the tail vein or internal carotid artery migrated into the injured brain parenchyma and were observed to express neuronal and astroglial markers at 2 weeks after administration and improved the neuromotor function of animals (33). Intra-parenchymal transplantation of whole bone marrow into the pericontusional tissue in the CCI model in rats, at 24 h after injury, also improved functional outcome and differentiation of transplanted cells into neurons and glia (40). Although the field is still in its infancy, transplantation of a wide variety of cells into the CNS is currently under laboratory investigation. Cells have been shown to survive and integrate after transplantation into the injured brain, but mechanisms of graft function are still unclear. In addition, results obtained using rodent-derived stem and progenitor cells should be confirmed using human equivalents to evaluate if positive results can be replicated. Neurogenesis The discovery of a population of endogenous progenitor cells and their association with continuing neurogenesis within the adult brain has engendered great interest in the potential role of these cell populations for neuronal replacement therapy in CNS injury and disease (41, 42). Under physiological conditions, neurogenesis in adult animals is restricted to the subgranular layer of the dentate gyrus (DG) and the subventricular zone (SVZ). For endogenous neural stem cells to yield therapeutic value in models of CNS injury, they must proliferate at a rate sufficient to replace dying cells, migrate to sites of pathology, survive within the site of pathology, differentiate CELL REPLACEMENT THERAPY FOR BRAIN TRAUMA into the appropriate cellular phenotypes, and in the case of neurons, undergo a program of maturation that includes neuritogenesis, myelination, and synaptogenesis. The hippocampal formation is selectively vulnerable to experimental TBI (1). Bilateral loss of dentate hilar cells projecting to the molecular layers of the DG following FP TBI has been associated with persistent memory dysfunction and loss of both DG neurons and CA3 pyramidal neurons has been observed (1, 27). Nonetheless, TBI appears to induce a transient increase in the regenerative potential of injured hippocampal neurons, as evidenced by enhanced expression of growth-related proteins, including polysialylated neural cell adhesion molecule (PSA-NCAM) (43) and growth-associated protein 43 (GAP43) (44). Dash and colleagues (45) were the first to document increased neurogenesis following CCI injury and reported a bilateral increase in BrdU-immunopositive cells within the granule cell layer of the hippocampus as early as 24 h postinjury. This reactive proliferation peaked between 3 d and 7 d postinjury and returned to baseline levels by 14 d postinjury. Despite the fact that the environment of the damaged CNS contains high levels of molecules that inhibit neurite outgrowth (46), a population of endogenous cells within the DG in response to brain injury has been shown to proliferate and project axons to the correct hippocampal subfield, that is, from the DG to the CA3 (D. L. Emery et al, personal communication). Within rodent and nonhuman primate brain, cells from the SVZ normally traverse the brain to their target, the olfactory bulb, via the rostral migratory stream. Upon reaching the core of the olfactory bulb, these neuroblasts move radially into the granular and periglomerular layers, where they differentiate into mature neurons (47). Recently, an increase in cellular proliferation was observed 48 h after TBI in rats both in the hippocampus and in the SVZ (45, 48). While these proliferating hippocampal cells were positive for immature astrocyte and activated microglia markers, the proliferating cells in the SVZ seemed not to have begun to differentiate at this time point after injury. It has been suggested that neural stem cells exhibit an intrinsic tropism CNS pathology (49), allowing them to migrate toward the site of injury. Although an increase in the rate of neurogenesis within the DG of the hippocampus and SVZ has been observed in several models of experimental TBI (45, 50) it is unclear whether these new cells are capable of migrating towards the site of injury. Although recent evidence suggests that newly born cells possess essential properties of functional neurons in uninjured adult mice (51), it remains to be unequivocally determined whether these cells contribute to behavioral changes in normal or pathological conditions. Suggesting a potential role for endogenous neural stem cells in ‘‘self-repair,’’ Macklis and colleagues (52) observed that the formation of mature neurons from endogenous precursors was restricted to the layer of cortex 807 where synchronous apoptosis was induced, and these new neurons survived at least 28 weeks. Retrograde labeling from the thalamus revealed that BrdU-immunopositive cells extended axons to the thalamus. However, this model lacked the immune response associated with more clinically relevant injury models and was limited to few cells. Nonetheless, these data provide an important ‘‘proof of principle,’’ i.e. a small number of cells from neurogenic regions retain the ability to respond to injury by migrating toward the sites of injury, becoming mature neurons, and express regional-specific markers consistent with those normally expressed by cells lost as a result of the injury. Although this phenomena remains to be evaluated in models of TBI, it has recently been observed that the dormant capacity of endogenous progenitor cells to participate in structural and functional recovery after transient forebrain ischemia in rats can be induced with infusion of basic fibroblast growth factor (FGF-2) and epidermal growth factor (EGF) into the lateral ventricles (53). Most interestingly, these new neurons appeared in the pyramidal layer of the CA1, an area of brain exquisitely vulnerable to ischemia-induced cell death, and the presence of these new neurons correlated with a significant amelioration of cognitive deficits. These observations suggest that exogenous augmentation of the neurogenic response to CNS injury will likely be required to result in functional recovery. The identification of the factors regulating adult neurogenesis has been intensively investigated during the past decade. The birth and survival of new neurons in the adult brain appears to be under dynamic regulation and neurogenic regions are sensitive to both pharmacological manipulation and environmental stimuli. Adult animals housed in an enriched environment exhibit increased dentate granule cell neurogenesis (54), as well as improved spatial memory (55), while voluntary exercise is sufficient for enhanced neurogenesis in the adult mouse DG (56). Studies have demonstrated that chronic stress elevates circulating adrenal steroids and stimulates glutamate release in the hippocampus (57). Subsequent activation of NMDA receptors decreases DG granule cell proliferation, while administration of NMDA antagonists leads to an increase in production of new granule cells. In addition, the stress-induced suppression of LTP resembles the alterations in LTP that occur after TBI (58). Although a massive release of glutamate is thought to be one of the major initial events in the pathophysiology of TBI, whether this prolonged elevation in glutamate levels compromises the neurogenic response following TBI remains to be elucidated. Interestingly, Riluzole, a sodiumchannel blocker with glutamate antagonist activity, previously shown to be neuroprotective in experimental models of TBI (59), has recently been shown to enhance expression of BDNF with consequent proliferation of J Neuropathol Exp Neurol, Vol 62, August, 2003 808 ROYO ET AL granule precursor cells in the rat hippocampus (60). Regulation of neurogenesis by environmental stimuli, stress, and corticosteroids has led to the investigation of the effect of psychotropic drugs on neurogenesis. Serotonin seems to play an important role in the regulation of neurogenesis through the activation of the 5HT–1A receptor. Chronic treatment with selective serotonin reuptake inhibitors (SSRI) such as fluoxetine was shown to increase rat hippocampal neurogenesis (61). Consistent with these results, the administration of 5HT–1A receptor antagonists was shown to decrease cell proliferation in the DG of the hippocampus of experimental animals (62). Several studies suggest that the cAMP signaling cascade and phosphorylation of the transcription factor CREB are implicated in hippocampal neurogenesis since phosphodiesterase (PDE) inhibitors such as Rolipram (PDE-4) (63) and Sidenafil (PDE-5) have been shown to enhance neurogenesis and to be neuroprotective after experimental cerebral ischemia (64). Endogenous growth factors that affect neurogenesis in vivo have also been identified. Peripheral administration of IGF-1 has been shown to selectively induce neurogenesis in the adult rat hippocampus (65), and exercise-induced neurogenesis in the adult rat hippocampus has been reported to be mediated by uptake of IGF-1 into the brain parenchyma (66). Since peripheral administration IGF-1 has also been shown to be neuroprotective after experimental TBI (67), it would be interesting to evaluate its ability to stimulate neurogenesis in the context of injury. EGF and FGF-2 also appear to have differential effects on neural progenitors. While intracerebroventricular administration of both growth factors has been shown to expand the SVZ progenitor population, only FGF-2 was able to induce an increase in newborn cells, mostly neurons, in the olfactory bulb (68). Following experimental cerebral ischemia, it has been demonstrated that endogenously synthesized FGF-2 is necessary and sufficient to stimulate proliferation and differentiation of neuroprecursor cells in the hippocampus (69). Heparin-bindingEGF-like growth factor, an endogenous mitogenic and chemotactic glycoprotein containing an EGF-like domain, has also been shown to stimulate proliferation of neuronal precursors in the SVZ and the DG (70), while vascular endothelial growth factor (VEGF) has been shown to stimulate neurogenesis in vitro and in vivo together with the proliferation of astrocytes and endothelial cells (71). The angiogenic properties of VEGF together with its ability to stimulate the proliferation of neuronal progenitors may represent an interesting strategy to promote both angiogenesis and neurogenesis after TBI. It has recently been shown that erythropoietin (EPO) is not only a hematopoietic factor, but is also an intrinsic hypoxia-induced factor produced in the brain together with J Neuropathol Exp Neurol, Vol 62, August, 2003 its receptor, capable of regulating the production of neuronal progenitor cells from the forebrain neurogenic region in mice (72). Although several members of the neurotrophin family have been shown to stimulate neuronal proliferation and/or survival in vitro, only BDNF has been demonstrated to stimulate neurogenesis in vivo. Administration of BDNF has been demonstrated to increase the number of new neurons in the striatum, thalamus, and hypothalamus of mature rats (73) as well as in the olfactory bulb (74). A decrease in DG cell proliferation has also been observed in heterozygous BDNF knockout mice (73). Conversely, long-term delivery via the transduction of BDNF gene in the hippocampus has been shown to suppress ischemia-induced proliferation in the DG of adult rats (75). In many regions of the brain following TBI, neuronal cell bodies are spared but their axonal connections are severed. One crucial event for proper neuronal regeneration may be the ability to rebuild appropriate circuitry, implicating proper growth and guidance of the newly forming axons and dendrites towards the target cells, and the degree of axonal regeneration may play a major role in determining outcome after TBI. This process is under the control of intrinsic molecules within the growth cones and extrinsic guidance molecules (either attractant or repellent), sometimes acting over long distances in the CNS (76). These molecules include netrins, semaphorins, ephrins, slits, and cell adhesion molecules, all of which are transcriptionally regulated, constituting a system able to generate diverse and sometimes opposed outcomes (77). Although adult mammalian CNS neurons exhibit a capacity for axonal outgrowth given a permissive environment, anatomical and functional recovery is limited by inhibitory factors including myelin-associated glycoprotein (MAG), oligodendrocyte myelin glycoprotein (OMgp), chondroitin sulphate proteoglycans (CSPG), and Nogo-A, a myelin-associated neurite outgrowth inhibitor expressed by oligodendrocytes (78, 79). MAG, Nogo, and OMgp all bind with high affinity to the Nogo receptor complex, interacting with p75 as a co-receptor (80), and may cause intracellular activation of the family of Rho GTPases including Rho, Rac, and Cdc42. Rho activation, also by netrin and ephrin receptors and cell adhesion molecules, causes growth cone collapse, neurite retraction, and cell rounding through its effect on the cytoskeleton (81). Whether this incomplete regeneration after CNS injury to the adult brain results from a lack of intrinsic growth capacity or the presence of an extrinsic growth inhibitory environment remains to be established. Recently, a monoclonal antibody against Nogo-A (11C7) was found to improve neurological and cognitive outcome following TBI in rats (P. M. Lenzlinger et al, personal communication), and inhibition of Rho was shown to promote axonal growth and regeneration with rapid neurological recovery after spinal cord injury in mice CELL REPLACEMENT THERAPY FOR BRAIN TRAUMA (82). Promoting axonal recovery through a combination of neurogenesis and modulation of the factors mentioned above may be a future treatment option in TBI. CONCLUSION The complete understanding of the mechanisms controlling the proliferation, migration, differentiation, and axon extension of endogenous precursors will likely aid in the development of efficient therapies for CNS injury such as TBI. Pharmacological manipulation of this neurogenic potential, either by increasing the proliferation rate or inducing neuronal differentiation, may represent a new strategy with tremendous potential for the treatment of TBI. These observations underscore the need for further exploration of the role of growth factors in mediating neurogenesis in the adult CNS to advance the development of neuronal replacement strategies after brain damage by pharmacologically manipulating neural precursors in situ. Despite improvements in the medical and surgical treatment of TBI, there are still currently no neuroprotective agents available to counteract secondary or delayed damage to the injured brain or to stimulate its repair and recovery. The development of cell replacement therapies may offer an alternative or a complementary strategy for the treatment of TBI. Recent advances both in the identification of a variety of cell lines with a potential for CNS transplantation and in the characterization of the neurogenic regions of the brain represent a new opportunity of great interest for delayed intervention in TBI patients. REFERENCES 1. Hicks RR, Soares HD, Smith DH, McIntosh TK. Temporal and spatial characterization of neuronal injury following lateral fluid-percussion brain injury in the rat. Acta Neuropathol 1996;91:236–46 2. Cortez SC, McIntosh TK, Noble L. Experimental fluid percussion brain injury: Vascular disruption and neuronal and glial alterations. Brain Res 1989;482:271–82 3. Raghupathi R, Graham DI, McIntosh TK. Apoptosis after traumatic brain injury. J Neurotrauma 2000;17:927–38 4. Sato M, Chang E, Igarashi T, Noble LJ. Neuronal injury and loss after traumatic brain injury: Time course and regional variability. Brain Res 2001;917:45–54 5. Colicos MA, Dixon CE, Dash PK. Delayed, selective neuronal death following experimental cortical impact injury in rats: Possible role in memory deficits. Brain Res 1996;739:111–19 6. Gallyas F, Zoltay G, Balas I. An immediate light microscopic response of neuronal somata, dendrites and axons to contusing head injury in the rat. Acta Neuropathol 1992;83:394–401 7. Roy M, Sapolsky R. Neuronal apoptosis in acute necrotic insults: Why is this subject such a mess? Trends Neurosci 1999;22:419–22 8. Rink AD, Fung K-M, Trojanowski JQ, Lee V, Neugebauer E, McIntosh TK. Evidence of apoptotic cell death after experimental traumatic brain injury in the rat. Am J Pathol 1995;147:1575–83 9. Conti AC, Raghupathi R, Trojanowski JQ, McIntosh TK. Experimental brain injury induces regionally distinct apoptosis during the acute and delayed post-traumatic period. J Neurosci 1998;18: 5663–72 809 10. Gibson S, Widmann C, Johnson GL. Differential involvement of MEK kinase 1 (MEKK1) in the induction of apoptosis in response to microtubule-targeted drugs versus DNA damaging agents. J Biol Chem 1999;274:10916–22 11. Otani N, Nawashiro H, Fukui S, Nomura N, Shima K. Temporal and spatial profile of phosphorylated mitogen-activated protein kinase pathways after lateral fluid percussion in the cortex of the rat brain. J Neurotrauma 2002;19:1587–96 12. Raghupathi R, Muir JK, Fulp CT, Pittman RN, Grady MS, McIntosh TK. Acute alterations in mitogen-activated protein kinases following traumatic brain injury: Implications for post-traumatic cell death. Exp Neurol 2003; in press 13. Mori T, Wang X, Jung JC, et al. Mitogen-activated protein kinase inhibition in traumatic brain injury: In vitro and in vivo effects. J Cereb Blood Flow Metab 2002;22:444–52 14. Dash PK, Mach SA, Moore AN. The role of extracellular signalregulated kinase in cognitive and motor deficits following experimental traumatic brain injury. Neurosci 2002;114:755–67 15. Yakovlev AG, Knoblach S, Fan L, Fox GB, Goodnight R, Faden AI. Activation of CPP32-like caspases contributes to neuronal apoptosis and neurological dysfunction after traumatic brain injury. J Neurosci 1997;17:7415–24 16. Buki A, Okonkwo DO, Wang KK, Povlishock JT. Cytochrome c release and caspase activation in traumatic axonal injury. J Neurosci 2000;20:2825–34 17. Clark RSB, Kochanek PM, Dixon CD, et al. Early neuropathologic effects of mild or moderate hypoxemia after controlled cortical impact injury in rats. J Neurotrauma 1997;14:179–89 18. Clark RS, Kochanek PM, Chen M, et al. Increases in Bcl-2 and cleavage of caspase-1 and caspase-3 in human brain after head injury. FASEB Journal 1999;13:813–21 19. Ye H, Cande C, Stephanou NC, et al. DNA binding is required for the apoptogenic action of apoptosis inducing factor. Nature Struct Biol 2002;9:680–84 20. Graham DI, Gennarelli TA, McIntosh TK. Cellular and molecular consequences of TBI. In: Graham DI, Luntus PL, eds. Greenfield’s Neuropathology 2002; 823–98 21. Graham DI, Ford I, Adams JH, Doyle D, Teasdale G, Lawrence A, McLellan DR. Ischaemic brain damage is still common in fatal nonmissile head injury. J Neurol Neurosurg Psychiatry 1989;52: 346–50 22. Williams S, Raghupathi R, MacKinnon MA, McIntosh TK, Saatman KE, Graham DI. In situ DNA fragmentation occurs in white matter up to 12 months after head injury in man. Acta Neuropathol 2001;102:581–90 23. Smith FM, Raghupathi R, MacKinnon M-A, et al. TUNEL-positive staining of surface contusions after fatal head injury in man. Acta Neuropathol 2000;100:537–45 24. Fowler J, MacKinnon MA, Raghupathi R, Saatman KE, McIntosh TK, Graham DI. Age does not influence DNA fragmentation in the hippocampus after fatal traumatic brain injury in young and aged humans compared with controls. Clin Neuropathol 2002;21:156–62 25. Shuman SL, Bresnahan JC, Beattie MS. Apoptosis of microglia and oligodendrocytes after spinal cord contusion in rats. J Neurosci Res 1997;50:798–808 26. Soares HD, McIntosh TK. Fetal cortical transplants in adult rats subjected to experimental brain injury. J Neural Trans & Plas 1991; 2:207–20 27. Soares HD, Sinson G, McIntosh TK. Fetal hippocampal transplants attenuate hippocampal CA3 pyramidal cell death resulting from fluid percussion brain injury in the rat. J Neurotrauma 1995;12:1059–67 28. Sinson G, Voddi M, McIntosh TK. Combined fetal neural transplantation and nerve growth factor infusion: Effects on neurological outcome following fluid-percussion brain injury in the rat. J Neurosurg 1996;84:655–62 J Neuropathol Exp Neurol, Vol 62, August, 2003 810 ROYO ET AL 29. Cao Q, Benton RL, Whittemore SR. Stem cell repair of central nervous system injury. J Neurosci Res 2002;68:501–10 30. Trojanowski JQ, Kleppner SR, Hartley RS, et al. Transfectable and transplantable postmitotic human neurons: A potential ‘‘platform’’ for gene therapy of nervous system diseases. Exp Neurol 1997;144: 92–97 31. Kondziolka D, Wechsler L, Goldstein S, et al. Transplantation of cultured human neuronal cells for patients with stroke. Neurol 2000;55:565–69 32. Meltzer CC, Kondziolka D, Villemagne VL, et al. Serial [18F] fluorodeoxyglucose positron emission tomography after human neuronal implantation for stroke. Neurosurg 2001;49:586–91 33. Philips MF, Muir JK, Saatman KE, et al. Survival and integration of transplanted postmitotic human neurons following experimental brain injury in immunocompetent rats. J Neurosurg 1999;90: 116–24 34. Watson DJ, Longhi L, Lee EB, et al. Genetically modified NT2N human neuronal cells mediate long-term gene expression as CNS grafts in vivo and improve functional cognitive outcome following experimental brain injury. J Neuropathol Exp Neurol 2003; 62:368–80 35. Philips MF, Mattiasson G, Wieloch T, et al. Neuroprotective and behavioral efficacy of nerve growth factor-transfected hippocampal progenitor cells transplants after experimental traumatic brain injury. J Neurosurg 2001;94:765–74 36. Gray JA, Hodges H, Sinden J. Prospects for the clinical application of neural transplantation with the use of conditionally immortalized neuroepithelial stem cells. Phil Trans R Soc Lond 1999;354:1407–21 37. Park KI, Liu S, Flax JD, Nissim S, Stieg PE, Snyder EY. Tranplantation of neural progenitor and stem cells: Developmental insights may suggest new therapies for spinal cord and other CNS dysfunction. J Neurotrauma 1999;16:675–87 38. Riess P, Zhang C, Saatman KE, et al. Transplanted neural stem cells survive, differentiate, and improve neurological motor function after experimental traumatic brain injury. Neurosurgery 2002;51: 1043–54 39. Tate MC, Shear DA, Hoffman SW, Stein DG, Archer DR, LaPlaca MC. Fibronectin promotes survival and migration of primary neural stem cells transplanted into the traumatically injured mouse brain. Cell Transplant 2002;11:283–95 40. Sanchez-Ramos JR. Neural cells derived from adult bone marrow and umbilical cord blood. J Neurosci Res 2002;69:880–93 41. Cameron HA, McKay R. Stem cells and neurogenesis in the adult brain. Curr Opin Neurobiol 1998;8:677–80 42. Gage FH, Ray J, Fisher LJ. Isolation, characterization, and use of stem cells from the CNS. Annu Rev Neurosci 1995;18:159–92 43. Emery DL, Raghupathi R, Saatman KE, Fischer I, Grady MS, McIntosh TK. Bilateral growth-related protein expression suggests a transient increase in regenerative potential following brain trauma. J Comp Neurol 2000;424:521–31 44. Christman CW, Salvant JB, Walker SA, Povlishock JT. Characterization of a prolonged regenerative attempt by diffusely injured axons following traumatic brain injury in the adult cat: A light and electron microscopic immunocytochemical study. Acta Neuropathol (Berl) 1997;94:329–37 45. Dash PK, Mach SA, Moore AN. Enhanced neurogenesis in the rodent hippocampus following traumatic brain injury. J Neurosci Res 2001;63:313–19 46. Grandpre T, Strittmatter SM. Nogo: A molecular determinant of axonal growth and regeneration. Neuroscientist 2001;7:377–86 47. Lois C, Alvarez-Buylla A. Proliferating subventricular zone cells in the adult mammalian forebrain can differentiate into neurons and glia. Proc Natl Acad Sci USA 1993;90:2074–77 J Neuropathol Exp Neurol, Vol 62, August, 2003 48. Chirumamilla S, Sun D, Bullock MR, Colello RJ. Traumatic brain injury induced cell proliferation in the adult mammalian central nervous system. J Neurotrauma 2002;19:693–703 49. Snyder EY, Yoon C, Flax JD, Macklis JD. Multipotent neural precursors can differentiate toward replacement of neurons undergoing targeted apoptotic degeneration in adult mouse neocortex. Proc Natl Acad Sci USA 1997;94:11663–68 50. Kernie SG, Erwin TM, Parada LF. Brain remodeling due to neuronal and astrocytic proliferation after controlled cortical injury in mice. J Neurosci Res 2001;66:317–26 51. van Praag H, Schinder AF, Christie BR, Toni N, Palmer TD, Gage FH. Functional neurogenesis in the adult hippocampus. Nature 2002;415:1030–34 52. Magavi SS, Leavitt BR, Macklis JD. Induction of neurogenesis in the neocortex of adult mice. Nature 2000;405:951–55 53. Nakatomi H, Kuriu T, Okabe S, et al. Regeneration of hippocampal pyramidal neurons after ischemic brain injury by recruitment of endogenous neural progenitors. Cell 2002;110:429–41 54. Kempermann G, Kuhn HG, Gage FH. More hippocampal neurons in adult mice living in an enriched environment. Nature 1997;386: 493–95 55. Nilsson M, Perfilieva E, Johansson U, Orwar O, Eriksson PS. Enriched environment increases neurogenesis in the adult rat dentate gyrus and improves spatial memory. J Neurobiol 1999;39:569–78 56. van Praag H, Kempermann G, Gage FH. Running increases cell proliferation and neurogenesis in the adult mouse dentate gyrus. Nat Neurosci 1999;2:266–70 57. Gould E, Tanapat P, Cameron HA. Adrenal steroids suppress granule cell death in the developing dentate gyrus through an NMDA receptor-dependent mechanism. Brain Res Dev Brain Res 1997; 103:91–93 58. Reeves TM, Lyeth BG, Povlishock JT. Long-term potentiation deficits and excitability changes following traumatic brain injury. Exp Brain Res 1995;106:248–56 59. Wahl F, Stutzmann JM. Neuroprotective effects of riluzole in neurotrauma models: A review. Acta Neurochir (Suppl) 1999;73:103–10 60. Katoh-Semba R, Asano T, Ueda H, et al. Riluzole enhances expression of brain-derived neurotrophic factor with consequent proliferation of granule precursor cells in the rat hippocampus. FASEB J 2002;16:1328–30 61. Brezun JM, Daszuta A. Serotonergic reinnervation reverses lesioninduced decreases in PSA- NCAM labeling and proliferation of hippocampal cells in adult rats. Hippocampus 2000;10:37–46 62. Radley JJ, Jacobs BL. 5-HT1A receptor antagonist administration decreases cell proliferation in the dentate gyrus. Brain Res 2002; 955:264–67 63. Nakagawa S, Kim JE, Lee R, et al. Localization of phosphorylated cAMP response element-binding protein in immature neurons of adult hippocampus. J Neurosci 2002;22:9868–76 64. Zhang R, Wang Y, Zhang L, et al. Sildenafil (Viagra) induces neurogenesis and promotes functional recovery after stroke in rats. Stroke 2002;33:2675–80 65. Anderson MF, Aberg MA, Nilsson M, Eriksson PS. Insulin-like growth factor-I and neurogenesis in the adult mammalian brain. Brain Res Dev Brain Res 2002;134:115–22 66. Trejo JL, Carro E, Torres-Aleman I. Circulating insulin-like growth factor I mediates exercise-induced increases in the number of new neurons in the adult hippocampus. J Neurosci 2001;21:1628–34 67. Saatman KE, Contreras PC, Smith DH, et al. Insulin-like growth factor-1 (IGF-1) improves both neurological motor and cognitive outcome following experimental brain injury. Exp Neurol 1997; 147:418–27 68. Kuhn HG, Winkler J, Kempermann G, Thal LJ, Gage FH. Epidermal growth factor and fibroblast growth factor-2 have different ef- CELL REPLACEMENT THERAPY FOR BRAIN TRAUMA 69. 70. 71. 72. 73. 74. fects on neural progenitors in the adult rat brain. J Neurosci 1997; 17:5820–29 Yoshimura S, Takagi Y, Harada J, et al. FGF-2 regulation of neurogenesis in adult hippocampus after brain injury. Proc Natl Acad Sci USA 2001;98:5874–79 Jin K, Mao XO, Sun Y, et al. Heparin-binding epidermal growth factor-like growth factor: Hypoxia-inducible expression in vitro and stimulation of neurogenesis in vitro and in vivo. J Neurosci 2002; 22:5365–73 Jin K, Zhu Y, Sun Y, Mao XO, Xie L, Greenberg DA. Vascular endothelial growth factor (VEGF) stimulates neurogenesis in vitro and in vivo. Proc Natl Acad Sci USA 2002;99:11946–50 Shingo T, Sorokan ST, Shimazaki T, Weiss S. Erythropoietin regulates the in vitro and in vivo production of neuronal progenitors by mammalian forebrain neural stem cells. J Neurosci 2001;21: 9733–43 Pencea V, Bingaman KD, Wiegand SJ, Luskin MB. Infusion of brain-derived neurotrophic factor into the lateral ventricle of the adult rat leads to new neurons in the parenchyma of the striatum, septum, thalamus, and hypothalamus. J Neurosci 2001;21:6706–17 Zigova T, Pencea V, Wiegand SJ, Luskin MB. Intraventricular administration of BDNF increases the number of newly generated 75. 76. 77. 78. 79. 80. 81. 82. 811 neurons in the adult olfactory bulb. Mol Cell Neurosci 1998;11: 234–45 Larsson E, Mandel RJ, Klein RL, Muzyczka N, Lindvall O, Kokaia Z. Suppression of insult-induced neurogenesis in adult rat brain by brain-derived neurotrophic factor. Exp Neurol 2002;177:1–8 Chisholm A, Tessier-Lavigne M. Conservation and divergence of axon guidance mechanisms. Curr Opin Neurobiol 1999;9:603–15 Grunwald IC, Klein R. Axon guidance: Receptor complexes and signaling mechanisms. Curr Opin Neurobiol 2002;12:250–59 Huber AB, Schwab ME. Nogo-A, a potent inhibitor of neurite outgrowth and regeneration. Biol Chem 2000;381:407–19 McKerracher L, Winton MJ. Nogo on the go. Neuron 2002;36: 345–48 Wang KC, Kim JA, Sivasankaran R, Segal R, He Z. P75 interacts with the Nogo receptor as a co-receptor for Nogo, MAG and OMgp. Nature 2002;420:74–78 Fritz JL, VanBerkum MF. Regulation of rho family GTPases is required to prevent axons from crossing the midline. Dev Biol 2002;252:46–58 Dergham P, Ellezam B, Essagian C, Avedissian H, Lubell WD, McKerracher L. Rho signaling pathway targeted to promote spinal cord repair. J Neurosci 2002;22:6570–77 J Neuropathol Exp Neurol, Vol 62, August, 2003