Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
G protein–coupled receptor wikipedia , lookup
Signal transduction wikipedia , lookup
Paracrine signalling wikipedia , lookup
Butyric acid wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Biochemistry wikipedia , lookup
Lipid signaling wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Endocannabinoid system wikipedia , lookup
Specialized pro-resolving mediators wikipedia , lookup
Wilson's disease wikipedia , lookup
Fatty acid synthesis wikipedia , lookup
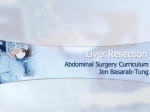
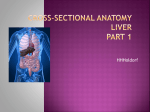
250 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism: Implications in NAFLD Michele Vacca, MD, PhD1,2 Michael Allison, MD, PhD3 Antonio Vidal-Puig, MD, PhD2 1 Medical Research Council - Human Nutrition Research (MRC-HNR), Cambridge, United Kingdom 2 Department of Clinical Biochemistry and University of Cambridge Metabolic Research Laboratories, Institute of Metabolic Science, Cambridge, United Kingdom 3 Liver Unit, Department of Medicine, Cambridge Biomedical Research Centre, Cambridge University NHS Foundation Trust, United Kingdom 4 Department of Biochemistry, University of Cambridge, United Kingdom Julian L. Griffin, PhD1,4 Address for correspondence Antonio Vidal-Puig, MD, PhD, FRCP, FmedSci, TVPLab, Metabolic Research Laboratories Level 4, Institute of Metabolic Science, Box 289, Addenbrooke’s Hospital, Cambridge CB2 0QQ, United Kingdom (e-mail: [email protected]). Michele Vacca, MD, PhD, Medical Research Council – Human Nutrition Research (MRC-HNR) & Institute of Metabolic Science, University of Cambridge, Elsie Widdowson Laboratory, 120 Fulbourn Road, Cambridge CB1 9NL, United Kingdom (e-mail: [email protected]). Semin Liver Dis 2015;35:250–261. Abstract Keywords ► insulin resistance ► mitochondrial dysfunction ► peroxisome proliferator-activated receptors ► sterol regulatory element binding protein 1 ► carbohydrate response elementbinding protein The term nonalcoholic fatty liver disease (NAFLD) covers a pathologic spectrum from lipid accumulation alone (simple steatosis) to steatosis with associated inflammation and fibrosis (nonalcoholic steatohepatitis [NASH]). Nonalcoholic steatohepatitis can progress to cirrhosis and potentially to hepatocellular carcinoma. Although a genetic predisposition has been highlighted, NAFLD is strongly associated with an unhealthy lifestyle and hypercaloric diet in the context of obesity and metabolic disease. The dysregulation of specific pathways (insulin signaling, mitochondrial function, fatty acid, and lipoprotein metabolism) have been linked to steatosis, but elucidating the molecular events determining evolution of the disease still requires further research before it can be translated into specific personalized interventional strategies. In this review, the authors focus on the early events of the pathophysiology of NASH, dissecting the metabolic and nutritional pathways involving fatty acids and glucose sensors that can modulate lipid accumulation in the liver, but also condition the progression to cirrhosis and hepatocellular carcinoma. The liver is a key player in the modulation of whole body energy homeostasis, and hepatic dysfunction is usually associated with systemic metabolic unbalances and vice versa. The nonalcoholic fatty liver disease (NAFLD) spectrum includes histologic changes ranging from simple steatosis to steatohepatitis (NASH), fibrosis, and cirrhosis (developing in 29% of NASH patients) ultimately leading (in 27% of NASH-cirrhosis patients) to hepatocellular carcinoma (HCC) development.1–3 Steatosis is defined as an intrahepatic triglyceride (TG) deposition exceeding the 95th percentile of TG content (> 55 mg/g of liver) for lean healthy individuals, or as the presence of micro- or macrovesicles in > 5% of hepato- Issue Theme Nonalcoholic Fatty Liver Disease; Guest Editors, Christopher P. Day, FMedSci, and Quentin M. Anstee, BSc, MBBS, PhD, MRCP(UK) cytes.2,3 Often benign and self-limited, steatosis can progress when hepatocyte injury (ballooning and cell death), inflammatory infiltrates and/or extracellular matrix deposition develop, histologic changes diagnosed as nonalcoholic steatohepatitis (NASH). Nonalcoholic steatohepatitis has emerged as the most rapidly increasing cause of chronic liver disease; it is related to the epidemic of obesity extending to both adults and children.4 Epidemiologic data has shown that NAFLD is the typical hepatic manifestation of metabolic syndrome (MetS), with a 50% prevalence of NAFLD in subjects with diabetes, 76% in those with obesity, and 100% in those morbidly obese with type 2 diabetes.3 Conversely, 50 to 100% Copyright © 2015 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel: +1(212) 584-4662. DOI http://dx.doi.org/ 10.1055/s-0035-1562945. ISSN 0272-8087. Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism of subjects with NASH are overweight, 50 to 60% have systemic hypertension, and 50 to 60% have dyslipidemia.3 When compared with the general population, NAFLD patients also show an increased mortality and risk for cardiovascular disease (CVD).1 The first step in the pathophysiology of NAFLD is the accumulation of lipids in the liver that follow an imbalance between lipid acquisition and removal. Whether steatosis can progress toward NASH, or these entities represent two different diseases, is still highly debated. In fact, it can be argued that when lipids are qualitatively inert, they lead to “simple steatosis.” Alternatively, when they are reactive, they promote lipotoxicity and NASH due to the formation of TG-derived toxic metabolites (e.g., diacylglycerols, ceramides, cholesterol, reactive oxygen species) ultimately causing hepatocyte dysfunction, lipoapoptosis, and the development of proinflammatory and fibrogenic stimuli.2 Sources of increased lipid (TG) in the liver include excess dietary TG intake, enhanced intrahepatic TG synthesis (fatty acids formed from de novo lipogenesis [DNL]), excess fatty acid (FA) influx into the liver from adipose tissue lipolysis, diminished export of lipids from the liver, and reduced fatty acid oxidation (FAO). Nonalcoholic fatty liver disease thus results from excessive storage of lipid species occasionally exceeding the capability of the hepatocytes to accommodate them physiologically.5 All these biochemical events are under the control of a complex system of signaling/transcriptional pathways, governed by hormones, cytokines, adipokines, and nutrient-sensing transcription factors. In this review, we will focus on the events that coordinately induce lipotoxicity, namely: (1) adipose tissue dysfunction, lipotoxicity, and insulin resistance; (2) reduced oxidative potential of the liver; (3) unbalances in lipoprotein trafficking; (4) prolonged positive energy balance (►Fig. 1); and on how they are controlled by insulin and nutrient-sensing transcription factors. Adipose Tissue Dysfunction, Lipotoxicity, and Insulin-Resistance Patients with NAFLD typically present with hyperinsulinemia and insulin resistance (IR). Insulin resistance originates from the convergence of genetic predisposition and environmental stressor factors, and has strong negative effects in liver metabolism.2,6 In the liver, insulin is essential to control the “fast-to-fed” metabolic shift in hepatic carbohydrate metabolism (promoting hepatic glucose uptake, glycolysis, and glycogen synthesis; inhibiting gluconeogenesis and glycogen utilization), and to modulate lipid metabolism (inhibiting FAO; promoteing DNL, free fatty acid [FFA] influx, and very low-density lipoprotein [VLDL] secretion) thus leading to hepatic lipid accumulation and to the promotion of hepatic triglyceride export (inducing hypertriglyceridemia6,7). Under physiologic conditions, insulin also inhibits lipolysis and FFA release from adipose tissue (AT) repressing the activity of hormone-sensitive lipase (HSL) (►Fig. 2).6,7 As a consequence of hyperinsulinemia (with/without hyperglycemia) excess glucose in the liver is converted to glycogen or is used to produce acetyl-CoA (via glycolysis) to be either further Vacca et al. Fig. 1 Nutrient fate in relationship to caloric intake. During isocaloric balanced feeding, nutrients are mainly used to produce energy and for structural purposes (e.g., membranes, proteins, organelles, DNA). Only a small quantity of these nutrients is stored during the fed states (to be released during fasting). A continuous hypercaloric feeding is associated with the need of storing excess calories. Cells have limited carbohydrate-storage capacity as glycogen; as a consequence, proteins and carbohydrates are converted into fatty acids and triglycerides having neither osmotic nor colloidal effects for the cell, and providing high caloric density (9 kcal/g).TGs, triglycerides. metabolized or, alternatively, utilized as a substrate for DNL.6,7 De novo lipogenesis facilitates the synthesis of saturated fatty acids (SFAs) for TG formation7 that can be stored within hepatocytes or, alternatively, packaged into VLDL lipoproteins to be secreted into the circulation (to be subsequently used in peripheral organs or stored in adipocytes).2 Triglycerides provide high caloric density (9 kcal/g), are insoluble in water, and have neither osmotic nor colloidal effects for the cell2; thus DNL is the preferred mechanism to stock excess energy within the body. When DNL is overactivated in the liver because of hyperinsulinemia, it promotes hepatic fat accumulation leading to NAFLD, and hypertriglyceridemia. Adipose tissue function is thus an important factor in the pathophysiology of NAFLD and its progression toward NASH as shown by the fact that loss of function of key genes in adipogenesis promotes steatosis and the progression of liver damage,8–10 and variants in genes known to be associated to steatosis (e.g., PNPLA3) also affect AT distribution.11 In health, AT protects the body from an excessive exposure to fatty acids; when adipocyte expandability is exhausted, this event is associated with lipotoxicity (the accumulation of toxic fatty acids derivatives in organs different from AT) and peripheral insulin resistance. Adipose tissue acquires a proinflammatory profile (suppression of adiponectin, promotion of adipocytokines) and these events in the liver lead to accumulation of lipid toxic species, reactive oxygen species (ROS) production, endoplasmic reticulum stress, activation of stellate cells, and progression of liver damage.12,13 Adipose tissue dysfunction and IR are early processes in the development of hepatic damage: In a population of “healthy” (nonobese, nondiabetic, normolipidemic) biopsy-proven NAFLD patients, hyperinsulinemia, and Seminars in Liver Disease Vol. 35 No. 3/2015 251 252 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism Vacca et al. Fig. 2 Role of hepatic fatty acid metabolism in the development of hepatic steatosis. Hepatic lipid accumulation can result from (1) a prolonged positive energy balance, (2) adipose tissue dysfunction and insulin resistance, (3) impairment of fatty acid oxidation and mitochondrial function, and (4) unbalances in lipoprotein trafficking. Insulin-mediated activation of SREBP1 proteins and glucose-mediated activation of ChREBP play a major role in these processes. Continuous arrows represent direct biochemical reactions, dash arrows represent modulatory mechanisms. ApoEr, ApoE receptor; FAT/CD36, fatty acid translocase/cluster differentiation protein-36; CETP, cholesteryl ester transfer protein; ChREBP, carbohydrate response element-binding protein; CM, chylomicrons; HDL, high-density lipoprotein; HSL, hormone-sensitive lipase; IDL, intermediate-density lipoprotein; LDL, low-density lipoprotein; LDLr, lowdensity lipoprotein receptor; OxLDL, oxidized low-density lipoprotein; Ox-Phos, oxidative phosphorylation; sLDL, small low-density lipoprotein; SREBPs, sterol regulatory element binding proteins; TG, triglyceride; VLDL, very low-density lipoprotein. AT/hepatic IR already coexist at the time of the diagnosis and progressively increase across NAFLD stages; of note, AT IR independently predicts liver histology and alters cardiometabolic risk parameters.14 Conversely, NAFLD can occur also in the absence of peripheral IR.3,5 Rats fed with a short-term high fat diet (HFD) develop hepatic fat accumulation and hepatic IR in the absence of changes in the whole body IR.15 Even if it is still debated whether peripheral or hepatic IR arises first, adipocyte dysfunction represents a contributing factor to the onset of lipotoxicity and (both peripheral and hepatic) IR, and could have a major role for the progression of fatty liver disease. Fatty Acid Oxidation, Mitochondrial Function, and the Progression of NASH Fatty acid β-oxidation allows the oxidation of FAs into acetylCoA, a substrate for oxidative phosphorylation (OXPHOS), ketone body formation, or for other biochemical reactions (e.g., gluconeogenesis or DNL).16,17 In normal conditions, β-oxidation occurs in mitochondria more than in peroxisomes. Mitochondrial β-oxidation is mostly controlled by Seminars in Liver Disease Vol. 35 No. 3/2015 the uptake of FA into the mitochondrial matrix via carnitine-palmityl-transferase 1 (CPT-1), which is inhibited by malonyl-CoA.16,17 Fatty acids can be metabolized exclusively in the presence of oxygen as the final acceptor of the reducing equivalents deriving from their oxidation by the four mitochondrial respiratory complexes. The mitochondrial respiratory complex couples the electron transfer activities to Hþtranslocation from the matrix to the outer side of the mitochondrial inner membrane thus building up a transmembrane electrochemical potential (Δψ).16,17 When adenosine diphosphate (ADP) is available, this electrochemical gradient is utilized for adenosine triphosphate (ATP) synthesis by ATP synthase, or it can otherwise exert a negative control feedback on the respiratory flux.16,17 Furthermore, ROS overproduction occurs when mitochondrial FAO supplies excessive respiratory substrates in the absence of a concomitant upregulation of mitochondrial respiratory chain activity, increases mitochondrial membrane potential (Δψ), or produces imbalances in the ATP/ADP ratio causing stalling of the respiratory flux.16,17 Excess FAs and ROS also promote uncoupling proteins (UCPs) activation that lower the mitochondrial Δψ and the intracellular oxygen tension increasing the respiration Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism rate (thus leading to reduced ROS production); this is a relay system that, when overactivated (e.g., in obesity and steatosis), affects OXPHOS efficiency.16 Thus, FAO itself promotes the saturation of the oxidative system in steatosis, and leads to mitochondrial dysfunction and to the promotion of the extramitochondrial (microsomal and peroxisomal oxidation) oxidation systems.16–18 Ω-oxidation of FAs is normally a minor pathway of FAO because one of its key enzymes, cytochrome P450 4A (CYP4A), is inhibited by insulin. Hence, IR leads to a significant overactivation of this pathway that produces long-chain dicarboxylic acids that further inhibit mitochondrial function.16–18 Long-chain dicarboxylic acids (and very long chain FAs) can be metabolized by the peroxisomal β-oxidation to complete their oxidation processes in mitochondria; the genetic ablation of enzymes involved in the peroxisomal β-oxidation leads to hepatic steatosis.19 Mitochondrial dysfunction and the activation of the extramitochondrial oxidation systems are thus key events in the development of a lethal vicious cycle able to generate a dramatic amplification of ROS production and liver damage that promotes the progression of NAFLD into NASH. The mitochondria are also the primary targets ROS-induced damage: Oxidative modifications of the respiratory complexes are associated with the impairment of their catalytic functions, mutagenesis of the mitochondrial DNA, mitochondrial dysfunction, and propagation of the oxidative damage, thus leading to hepatocellular death and NASH progression.17 Strategies aimed to improve the cellular REDOX homeostasis by supplying the hepatocyte with nonenzymatic antioxidant molecules (such as vitamin E20) could thus be a promising approach to the management of NASH. If Lipoproteins Deal with Liver’s Fat, What Goes Wrong in Steatosis? The liver is the major regulator of metabolite flux in the body, processing lipids provided by diet and AT-released FFAs (contributing in equal amounts), and to a smaller part by DNL in the liver itself. During the development of IR, the massive increase of FFA and the promotion of DNL render lipoprotein trafficking efficiency a critical step in the pathophysiology of NAFLD.2,21 The fate of newly formed or dietary lipids is to be oxidized, or to be esterified to TGs, incorporated into VLDL, secreted into the systemic circulation and delivered to the peripheral tissues. Very low-density lipoprotein particles are constituted by apolipoprotein (Apo) B-100 (ApoB-100) and C (ApoC), lipids (TGs and cholesterol esters), and phospholipids. Within the hepatocytes, microsomal transfer protein (MTP) promotes ApoB-100 fusion with TGs droplets, and VLDL formation and secretion.2,21 In the initial phases of steatosis, lipid accumulation is counterbalanced by increased VLDL secretion, but this adaptive mechanism reaches a point at which it is inadequate to compensate for the degree of intracellular TG accumulation.22,23 In fact, the VLDL-ApoB-100 secretion rates (the rate-limiting step in VLDL formation) is not increased in subjects with steatosis, thus leading to the production of very large TG-rich VLDL (that cannot be secreted through the sinusoidal endothelial Vacca et al. pores) and impairment of VLDL synthesis and export.24 Subsequently, serum levels of LDL and of the atherogenic small LDL (sLDL) also increase due to the promotion of cholesteryl ester transfer protein (CETP; enriches VLDL in cholesterol), and of hepatic lipase ([HL] regulates plasma concentration of the atherogenic lipoproteins intermediatedensity lipoproteins -IDL- and of sLDL). Both CETP and HL activities are increased in NAFLD and may favor the formation of sLDL.2 Dietary lipids are absorbed by enterocytes, incorporated in TG-rich chylomicrons, transported into the systemic circulation, and then delivered to the liver (20%) or peripheral tissue (80%), where lipoprotein lipase ([LPL] the rate-limiting step of TG uptake) releases FFAs for uptake.2 One of the strongest inhibitors of LPL is apolipoprotein C-III (ApoC-III; an essential constituent of VLDL particles), and a loss of function of this apolipoprotein has been associated with obesity and metabolic complications due to an enhanced peripheral activity of LPL.25 On the other hand, the overexpression of ApoC-III promotes liver steatosis and hepatic insulin resistance due to reduced peripheral FFA uptake, increased hepatic triglyceride delivery, and surprisingly, a reduction in hepatic triglyceride secretion.26 Interestingly, insulin and glucose exert opposite effects on ApoC-III, which is promoted by glucose and inhibited by insulin27,28; insulin instead promotes the expression of transporter fatty acid translocase / cluster differentiation protein-36 (FAT/CD36 mediates the uptake and the intracellular transport of FAs), thus facilitating lipid accumulation in the liver.29 In individuals with IR, insulin fails to suppress efficiently ApoC-III in the liver (thus leading to LPL inhibition in peripheral tissues, and to the increase of the hepatic uptake of TGs-rich chylomicrons remnants) and hormone-sensitive lipase (HSL) in AT (thus leading to an increase of adipose-derived FFA flux to the liver).29,30 Hepatic IR thus promotes a progressive deterioration of steatosis and a deleterious lipoprotein profile; this is the strongest evidence linking hepatic steatosis to the consequences of obesity and metabolic syndrome. Diet, Nutrient Sensors, and Modulation of Lipid Metabolism Sugar or Fat: Which Is the Enemy? Insights for addressing the role of excess calories and diet composition in the pathophysiology of NAFLD come from the study of animal models fed high-energy diets. Although not standardized in macronutrient content or composition, these studies show that prolonged energy excess, especially in the form of high carbohydrate or fat, rapidly induces fatty liver with differences in the progression of liver injury potentially depending on macronutrient composition.31,32 When energy balance is positive, mammalian livers preferentially use glycolysis to generate energy, while excess glucose is stored in the form of glycogen (glycogen synthesis) and fatty acids (DNL) that will be stored in the adipose tissue in the form of triglycerides; when positive excess energy intake is prolonged, the liver is also able to store significant quantities of lipids leading to hepatic steatosis (►Fig. 1).31,32 In terms of Seminars in Liver Disease Vol. 35 No. 3/2015 253 254 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism macronutrient composition, high sucrose/fructose diets induce intrahepatic lipid accumulation independently from their fat content, and do not necessarily progress toward steatohepatitis.32–34 On the other hand, it has also been shown that “high-fat” diets (35–70% of total calories constituted by fat) induce steatosis and liver damage not only due to fat content, but also due to their content in simple sugars. For example, ketogenic diets (very high in fat with almost no carbohydrate) neither induce massive steatosis nor raise alanine aminotransferase (ALT) outside the normal range.35 Saturated fat is able to stimulate both FAO via a peroxisome proliferator activated receptor-α (PPAR-α) dependent mechanism and DNL in the liver, but the prominence of these effects seems to depend on sucrose content;36,37 when saturated fat is consumed without sucrose, FAO promotion is the prominent feature, thus leading to minimal hepatic steatosis or liver injury.37 Diets that incorporate both macronutrients (carbohydrate and fat) thus appear to represent a situation closer to the so-called “Western” diet; such diets (enriched in saturated fat, cholesterol, sucrose and/or fructose) induce obesity, insulin resistance, and hepatic steatosis, along with different degrees of hepatic injury, inflammation, and mild fibrosis.38–40 The types of FA have also been invoked as a factor contributing to differences in the capability of diets to induce steatosis, for example, both small/medium-chain FAs (that need more energy to be utilized) and long-chain saturated FAs alone (stimulating FAO by promoting PPARα and its coactivator PGC-1-α) fail to induce massive steatosis,36,37,41 whereas transfats (> 15% of total calories)42,43 promote hepatic steatosis even in the absence of free sucrose. The role of polyunsaturated fatty acids (PUFAs) is still discussed because they decrease liver triglyceride content and plasma ALT levels in leptin-deficient mice,44 but when administered in excess (> 35% of total calories) via total enteral nutrition, PUFAs overfeeding causes steatosis and liver damage.45 Therefore, micronutrient composition could affect the capability of a specific diet to induce DNL and/or FAO. Further studies are necessary to assess whether specific nutrient mixtures cause liver injury in excess to their ability to induce hepatic steatosis. Sterol Regulatory Element Binding Protein 1c and Carbohydrate-Response Element-Binding Protein: Partners in DNL Promotion De novo lipogenesis is finely regulated at the transcriptional level mainly by two transcription factors, the sterol regulatory element binding protein 1 (SREBP1), and the glucose sensor carbohydrate response element-binding protein (ChREBP), which are activated by insulin and glucose, respectively. Both these transcription factors promote the expression of key enzymes for DNL (e.g., ATP citrate lyase [ACL]; acetyl-CoA carboxylase [ACC]; fatty acid synthase [FAS]).7,46 Insulin, SFAs, and the oxysterol sensor liver X receptor (LXR) promote SREBP1c,47,48 whereas PUFAs, glucagon, and 5' AMP-activated protein kinase (AMPK) signaling inhibit it.44,48,49 The relationship between insulin and SREBP-1c is finely regulated: Insulin promotes the expression of a SREBPSeminars in Liver Disease Vol. 35 No. 3/2015 Vacca et al. 1-mediated negative loop that activates DNL, but limits an excessive activation of this metabolic pathway toward the promotion of SREBP-1c inhibitor insulin-induced gene 1 (Insig1)50,51; SREBP-1c also negatively feedbacks insulin signaling through the inhibition of insulin receptor substrate 2 (IRS2), thus silencing phosphatidylinositol 3-kinases/protein kinase B, PI3K/Akt cascade.52,53 In obesity, hyperinsulinemia thus boosts SREBP-1c activation, which promotes DNL, negatively feedbacks insulin signaling (leading to decreased glycogen synthesis and increased gluconeogenesis), and directly promotes gluconeogenesis (e.g., phosphoenolpyruvate carboxykinase [PEPCK]), thus inducing steatosis and hyperglycemia.7,52 Increased intracellular glucose levels activate ChREBP54 resulting in the induction of the transcription of genes involved in glycolysis (e.g., liver pyruvate kinase [LPK]) and DNL,55 causing a further worsening of steatosis.5 In murine models of obesity, liver-specific adenovirus-mediated inhibition of ChREBP markedly impairs lipogenic gene expression in the liver, protects from hepatic steatosis, ameliorates insulin signaling and overall glucose tolerance, and also decreases plasma levels of triglycerides and nonesterified fatty acids.56 In patients with NASH, ChREBP expression correlates with the degree of steatosis; however, its expression decreases in the presence of severe insulin resistance.57 ChREBP overexpression promotes DNL genes and stearoyl-CoA desaturase-1 (Scd1), a critical regulator of energy metabolism that catalyzes the transformation of SFAs into monounsaturated fatty acids (MUFAs). As a consequence, ChREBP activation results in a prevalent accumulation of MUFAs that does not impact much on insulin sensitivity.57 In this the concomitant knockdown of Scd1 worsens insulin sensitivity.57 These findings are in line with a previous report showing that liver-specific Scd1 knockout (KO) mice are protected from steatosis when fed a high-carbohydrate very low-fat diet.32 Therefore, SREBP1c and ChREBP activation in hyperinsulinemic subjects has a crucial role in the development of hepatic lipid accumulation (►Fig. 2). The relative balance between SREBP1c and ChREBP contribution in modulating the lipogenic pathway could have different outcomes for the accumulation of specific lipid species and for the degree of IR, and could potentially explain different outcomes in terms of MetS complications.58,59 Peroxisome Proliferator-Activated Receptors and Their Coactivators in the Modulation of Hepatic Lipid Accumulation Lipid-sensing nuclear receptors (NRs) are transcription factors participating in the control of complex processes in living organisms. Nuclear receptors show considerable specificity in their activation and tissue-specific expression.60 In the human genome, 48 NRs have been identified, while in rodents there are 49.61 A subfamily of these transcription factors, known as “adopted-orphan NRs” acts as lipid sensors and have been involved in the pathophysiology of MetS.62 Of particular interest for the pathophysiology of NAFLD, are the “fatty acid sensors” peroxisome proliferator-activated receptors (PPARs) and their coactivators peroxisome Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism proliferator-activated receptor γ coactivators 1 (PGC1s; see ►Table 1). Peroxisome proliferator-activated receptors (PPARα/NR1C1; PPARβ/δ/NR1C2; PPARγ/NR1C3) form heterodimers with the retinoid X receptors (RXR) to control metabolic programs and to regulate energy homeostasis.62 Peroxisome proliferator-activated receptors bind to specific DNA consensus sites termed PPAR response elements (PPREs). Although sharing sequence and structure homology, PPARs are characterized by specific ligand-binding domains (that can accommodate a wide diversity of natural and synthetic compounds), tissue distributions, and physiologic functions.63 Peroxisome Proliferator-Activated Receptor α Peroxisome proliferator-activated receptor α (PPARα) is prominently expressed in the liver (also expressed at a lower level in kidney, heart, skeletal muscle, small intestine, brown AT, and immune cells) and can be activated by fatty acids, 1palmitoyl-2-oleoyl-sn-glycerol-3-phosphocholine, fibrates, highly selective PPARα agonists (e.g., LY518674), and SPPARMs (selective PPAR modulators).63 The major physiologic function of PPARα is to promote fatty acid utilization during fasting to allow gluconeogenesis,44,64,65 but PPARα is also one of the key regulators of the response to excess fat. In fact, PPARα modulates fatty acid uptake (fatty acid binding protein [FATP], CD36, CPT-1) and lipid trafficking (promotion of LPL and apoA proteins; inhibition of the LPL inhibitor apoCIII and of proprotein convertase subtilisin/type 9 [PCSK9]), promotes β-oxidation (acyl-CoA oxidase [ACOX], thiolase, acyl-CoA-dehydrogenase, cytochrome P450-ω-hydroxylase), and inhibits DNL.64,66–69 Given the ability of PPARα agonists to modulate both TG and HDL metabolism,70,71 fibrates are thus employed for the management of primary hypertriglyceridemia and mixed hyperlipid- Vacca et al. emia.72,73 Peroxisome proliferator-activated receptor α has also shown a potential in the regulation of the pathophysiologic events causing liver steatosis. Following a high-fat diet (HFD), high fructose or methionine-choline deficient ([MCD]; a model to induce NASH) diets, PPARα null mice develop hypertriglyceridemia and are more susceptible to steatosis and to the progression of NASH due to an impairment of mitochondrial fatty acid β-oxidation, and to increased hepatic oxidative stress and expression of proinflammatory genes. These mice also develop massive steatosis, lobular inflammation, with a significant increase of the NASH activity score when compared with wild-type animals.74–76 Conversely, PPARα ligands protect the liver from NAFLD and NASH, promoting fatty acid oxidation, and reducing endoplasmic reticulum stress, hepatic insulin resistance, glucose intolerance, and levels of expression of inflammatory genes.74,77–79 Despite the robustness of this evidence in animal models, only few trials with relatively low numbers of patients have been performed to confirm these results in humans, and have not so far provided additional support for significant efficacy in NASH. Although clofibrate was not effective in the management of NASH,80 fenofibrate was able to ameliorate the degree of metabolic impairment (especially fasting glucose, triglycerides, and apolipoprotein A1), and improve liver enzymes in a small cohort of patients with NASH; however, its effects on liver histology were minimal.81 Peroxisome Proliferator-Activated Receptor β/δ Peroxisome proliferator-activated receptor β/δ (PPARβ/δ) exhibits a broad expression pattern63,82 and can be activated by polyunsaturated fatty acids (eicosapentaenoic acid [EPA], arachidonic acid [ARA], and dihomo-γ-linoleic acid), prostaglandins (PGs; PGA1, PGE2, PGD2, prostacyclin -PGI- and its stable analogue carba-prostacyclin), 4-hydroxynonenal, and Table 1 Potential relevance of peroxisome proliferator-activated receptor (PPARs) and peroxisome proliferator-activated receptor γ coactivators (PGCs) in the pathophysiology of nonalcoholic fatty liver disease PPARα PPARβ/δ De novo lipogenesis ↓ ? Fatty acid oxidation & mitochondrial function " " Fatty acids uptake " / Lipoprotein transport " " Gluconeogenesis " Glycolysis PPARγ PGC1α PGC1β / " " " " " " / " " " / " (hepatic) ↓ (AT/systemic) " / " " " " " " Inflammation/damage ↓ ↓ ↓ ↓ ↓ Steatosis ↓ ? " (hepatic) ↓ (AT/systemic) ↓ ↓ Hepatic insulin sensitivity " " ↓ (hepatic) " (AT/systemic) " ¼ Triglycerides ↓ ↓ " (hepatic) ↓ (AT/systemic) ↓ " Abbreviations: ?, contradictory results; /, not investigated; ", promoted; ↓, inhibited; ¼, unchanged; hepatic, effects of hepatic-specific modulation; AT/systemic, effects of systemic or adipose tissue-specific modulation. Seminars in Liver Disease Vol. 35 No. 3/2015 255 256 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism selective synthetic agonists (GW501516, GW0742).83–85 In the liver, PPARβ/δ controls fatty acid oxidation and the uncoupling of oxidative phosphorylation through activation of its target genes such as long chain acyl-CoA dehydrogenase (LCAD), CPT-1, ACOX1, long chain acyl-CoA-synthetase (ACSL) and UCP-1. Depending on the organ targeted and the experimental design used, PPARβ/δ has shown positive or negative action on liver steatosis, but an overall beneficial action on its progression. Adipose tissue-specific overexpression of PPARβ/δ in rodents protects from diet-induced obesity, hypertriglyceridemia, and hepatic steatosis.86 In models of obesity-induced steatosis (HFD and ob/ob), pharmacologic or liver-specific adenoviral activation of PPARβ/δ promotes hepatic fatty acid oxidation (increase of plasma β-hydroxybutyrate and of mRNA expression of PPARα and its target genes, promotion of the AMPK/PGC-1α-lipin1/PPARα pathway) and the Krebs cycle,87,88 but also stimulates (AMPKmediated) insulin sensitivity, thus reducing fasting glucose levels, promoting hepatic glycogen deposition, and glycolysis.87,89 The effects of PPARβ/δ activation on DNL are controversial because some authors show that PPARβ/δ directly promotes the transcription of Insig-1 (thus leading to SREBP1c inhibition, DNL suppression, and reduced hepatic steatosis in obese diabetic db/db mice), whereas other authors indicate that PPARβ/δ induces hepatic lipid production mainly in the form of unsaturated (rather than saturated) fat.89,90 In both cases, liver damage has been shown to be reduced,89,90 and this goes in line with the inhibitory effect of PPARβ/δ on STAT3 phosphorylation that prevents the activation of proinflammatory signals (e.g., tumor growth factor β1, interleukin- [IL-] 6, IL-1β, MCP-1, tumor necrosis factor α, nuclear factor-κB1).91,92 Animal and human studies also provide evidence that PPARβ/δ is beneficial on lipoprotein metabolism because PPARβ/δ activation increases apoAI, apoAII, and HDL-cholesterol, while reducing small dense LDL levels.93–97 Apparent discrepancies in the role of PPARβ/δ to modulate DNL could be thus explained by the different experimental designs (i.e., obesity models, PPARβ/δ activation strategies) that preferentially select for specific functions of PPARβ/δ, depending on the pathophysiologic context. It seems likely that in the liver PPARβ/δ physiologically reacts to an excessive accumulation of lipids and/or products of oxidative stress and/or proinflammatory mediators (prostaglandins) to limit further accumulation of fat (by promoting FAO), to prevent hepatic insulin resistance (by promoting AMPK/PGC1α axis), and to limit further FA production associated with an excessive diet-induced insulinmediated activation of DNL (by promoting Insig-1). Nevertheless, analysis of the PPARβ/δ function in the progression of NASH deserves further attention because it has been shown that it promotes stellate cell activation and fibrosis (upon CCL4 challenge),98 and its role in hepatic proliferation and hepatocarcinogenesis is contentious.99,100 Peroxisome Proliferator-Activated Receptor γ The PPARγ gene encodes for three splicing variants giving rise to two functional proteins (PPARγ1 and PPARγ3 transcripts encode for PPARγ1 and is expressed in AT, immune cells, Seminars in Liver Disease Vol. 35 No. 3/2015 Vacca et al. intestine, liver, and kidney; PPARγ2 transcript encodes for a protein expressed in ATs). Peroxisome proliferator-activated receptor γ is an important transcriptional regulator of adipocyte differentiation and function.9,10,63 Mutations in the PPARγ gene (e.g., familial partial lipodystrophy type 3 [FPLD3], PPARγ Pro12Ala, C1431T polymorphisms) induce severe insulin resistance, dyslipidemia, steatosis, and earlyonset hypertension.101–105 A wide spectrum of PPARγ ligands has been identified, ranging from the potential natural ligands including monounsaturated and polyunsaturated FA, eicosanoid FA-derivatives (hydroxyoctadecanoic acid [HODE]; 13-HODE and 9-HODE), and prostanoids (e.g., 15-deoxy-Δ12,14-prostaglandin J2) to the pharmacologic agonists thiazolidinediones (TZDs), selective PPARγ modulators (SPARMs), partial PPARγ/α agonists (e.g., TDZ18), curcumin, protopanaxatriol, and harmine.72,106 Thiazolidinediones (pioglitazone and rosiglitazone) have been approved for clinical use in type 2 diabetes, and proposed as possibly effective in NASH.107 The primary therapeutic effect of TZDs is to promote the expansion of subcutaneous AT due to an enhanced differentiation of preadipocytes in mature adipocytes. This event promotes lipid repartitioning from visceral fat, liver, and skeletal muscle to the subcutaneous AT, preventing lipotoxicity-induced insulin resistance and increased circulating levels of FFA.8,9,108 Peroxisome proliferator-activated receptor γ also stimulates adiponectin secretion (by promoting AMPK signaling and FA oxidation, while inhibiting hepatic gluconeogenesis)63,109 and is a negative modulator of the proinflammatory cascades in the liver thus potentially preventing the progression of NASH.110 Tissue-specific PPARγ modulation strategies have provided the evidence that PPARγ exerts its beneficial effects on liver steatosis mainly due to its action in AT.8,10,111–115 A targeted deletion of PPARγ in AT is associated with elevated plasma levels of FFAs and triglycerides and increased susceptibility to HFD-induced steatosis, hyperinsulinemia, and IR.8 On the other hand, hepatocyte-specific PPARγ-knockout mice are protected against HFD-induced hepatic steatosis, show improved glucose tolerance, and reduced gluconeogenesis. Peroxisome proliferator-activated receptor γ-knockout mice are also characterized by a downregulation of genes involved in lipogenesis (SCD1, SREBP-1c, and ACC), lipid transport (CD36/ FAT, L-FABP, and MTP), and β-oxidation (PPARα and ACO).115 As a confirmation of a candidate “pro-steatotic” action of PPARγ into the liver, adenoviral PPARγ hepatic overexpression causes hepatic steatosis,116 overexpression of genes involved in fatty acid transport, and triglyceride synthesis.114,116 However, the pharmacologic systemic activation of PPARγ using TZDs has been suggested to be potentially beneficial in the management of NAFLD20 because the net result of systemic PPARγ activation is to (1) increase AT lipid uptake and storage, (2) decrease serum FFA and TG, (3) increase peripheral glucose absorption, and (4) enhance energy expenditure. Altogether these effects improve insulin sensitivity, and reduce hepatic gluconeogenesis and steatosis.9,63 Unfortunately, although effective in controlling glycosylated hemoglobin and reducing liver steatosis, the enthusiasm for TZDs as therapeutic agents has been limited in recent years Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism because they are not devoid of side effects such as weight gain (2–3 kg per 1% glycosylated hemoglobin lowered), anemia, pulmonary edema, congestive cardiac failure, and increased risk of myocardial infarction.117 Thus rosiglitazone was voluntarily withdrawn from the market despite being one of the most effective drugs in reducing glycosylated hemoglobin. Peroxisome Proliferator-Activated Receptor γ Coactivators A more radical approach to the treatment and the prevention of NASH could be the modulation of lipid homeostasis by strategies aiming at inducing peroxisome proliferator-activated receptor γ coactivator 1 (PGC1) α and β. First characterized as important regulators of mitochondrial biogenesis and function, PGC1s have been described as central coordinators of metabolic homeostasis and their modulation appears to be potentially beneficial in NAFLD. Peroxisome proliferator-activated receptor γ coactivator 1α coactivates multiple transcription factors (FoxO1, glucocorticoid receptor, hepatic nuclear factor-4α, estrogen-related receptor-α, and PPARα), thus acting as a key promoter of gluconeogenesis, fatty acid oxidation, lipid transport, and oxidative phosphorylation during times of nutrient deprivation.118 Hepatic PGC1α transcription is induced by fasting (because it is promoted by glucagon and inhibited by insulin), HFD, obesity, and insulin resistance. PGC1a is also tightly modulated at posttranscriptional level (e.g., by the AMPK/ SIRT pathway that is activated by cold, exercise, metformin, resveratrol, and other stimuli).118 PGC1α KO mice develop metabolic abnormalities in energy-demanding organs that lead to increased body fat, susceptibility to cold and, following short term starvation, hepatic steatosis (due to a combination of reduced mitochondrial respiratory capacity, promotion of lipogenic genes, and increased supply of FAs).119 Hepatic-specific PGC1α heterozygous mice show hypertriglyceridemia (due to increased expression of genes involved in triglyceride-rich lipoprotein assembly), hepatic steatosis and diminished ketogenesis during fasting (decreased expression of genes involved in β-oxidation). These mice also develop hepatic insulin resistance following HFD.120 Interestingly, mice lacking SIRT1 (one of the upstream regulators of the PGC1α/PPARα pair) in the liver show a similar phenotype. When fed with HFD, SIRT1 KO mice develop hepatic steatosis, hepatic inflammation, and endoplasmic reticulum stress due to the suppression of PGC-1α/PPARα.121 Altogether, these data indicate that pharmacologic modulation of AMPK/SIRT1 cascade could be an effective approach to preventing obesity-associated metabolic diseases. Peroxisome proliferator-activated receptor γ coactivator 1β is considered an important regulator of metabolism in the liver because it coactivates different key transcription factors (including estrogen-related receptors, nuclear respiratory factor 1, liver X receptors, etc.) involved in mitochondrial biogenesis, oxidative metabolism, lipogenesis, and TG secretion. HFD stimulates not only the expression of SREBP1 in liver, but also of PGC1β, which contributes to the induction of the lipogenic program facilitating the release of triglycerides and cholesterol in VLDL particles. However, unlike SREBP1, Vacca et al. PGC1β reduces fat accumulation in the liver through concomitant stimulation of FAO and lipoprotein transport.122 The global knockout of PGC1β, although not showing overt phenotype under normal laboratory conditions, is characterized by a general defect in the expression of genes involved in the electron transport chain of the mitochondria; and, in response to acute high fat dietary loads, the lack of PGC1β impairs hepatic lipid metabolism in the liver, resulting in hepatic steatosis123,124 and reduced lipoprotein-associated triglyceride and cholesterol content.123 Conversely, MCD-fed hepatocyte-selective PGC1β transgenic mice are protected from lipid overload and from the progression to fibrosis due to a coordinated promotion of mitochondrial function and lipoprotein metabolism, and a reduction of oxidative stress.125 In the context of liver steatosis, the selective modulation of PGC1 proteins and their targeted pathways is thus a candidate strategy to protect the liver from lipid accumulation and oxidative damage due to the pleiotropic action of these coactivators in lipid homeostasis. However, to date the strategies aiming at activating this pathway rely on indirectly modulating PGCs upstream cascades (e.g., with metformin, resveratrol, etc.) or on stimulating the relevant coactivated receptor (e.g., PPARs), whereas mechanisms to target PGC1 proteins directly in humans are still being sorted. Conclusion Hepatic steatosis and NASH are the hepatic manifestation of lipid-induced toxicity in the context of MetS, and are closely related to excessive dietary calorie intake, obesity, and impaired metabolic homeostasis. The close interrelationship between obesity, AT dysfunction, onset of IR, and NAFLD have been widely characterized, with defective insulin signaling, impaired mitochondrial function, and dysregulated lipoprotein trafficking being the key effectors leading to hepatic TG accumulation. However, the exact natural history of the disease and the factors responsible for the progression toward liver damage still remain elusive. Although lipotoxicity, oxidative stress, exogenous factors (e.g., drugs, microbiota, alcohol, and fructose consumption), and genetic predisposition have been proposed as modulators in this progression, more detailed insights are needed to elucidate the mechanisms responsible for the evolution of NAFLD toward more severe forms of hepatic disease. Currently, the modulation of lifestyle through diet and exercise and the management of obesity, insulin resistance, and diabetes are the toolkit of management with proven positive effects on steatosis likely to reduce the risk of progression of established NASH. However, a more detailed characterization of the pathways that define lipid-related reactive toxic species that cause the lipid-related hepatocyte cell death inflammation as well as those attempting to promote regeneration, hepatic stellate cell activation, and extracellular matrix deposition may provide an integrated picture of the pathophysiology of NASH and identify novel therapeutic approaches to prevent its progression toward cirrhosis and HCC. Seminars in Liver Disease Vol. 35 No. 3/2015 257 258 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism Vacca et al. Abbreviations Acknowledgments Prof. Vidal-Puig was funded by the MRC and BHF program grants; Dr. Vacca and Dr. Griffin by MRC program grant (MC_PC_13030); Dr. Allison by the Evelyn Trust Grant. Dr. Vacca was a fellow of Fondazione Umberto Veronesi (Italy). The authors are members of the EPoS (Elucidating Pathways of Steatohepatitis) consortium funded by the Horizon 2020 Framework Program of the European Union under Grant Agreement 634413. ACC ACL ACSL ACOX ADP Apo ARA AT ALT ATP ChREBP CPT-1 CVD CYP4A DNL EPA FA FAS FATP FFA FAO FPLD3 HCC HFD HL HODE HSL Insig1 IR IRS2 IL LCAD LPL MetS MTP NAFLD NASH OXPHOS PCSK9 PEPCK PG PGC1 PPARs PPREs PUFAs ROS RXRs SPARMs SREBP1 TG TZDs UCPs VLDL acetyl-CoA carboxylase ATP citrate lyase acyl-CoA-synthetase acyl-CoA oxidase adenosine diphosphate apolipoprotein arachidonic acid adipose tissue alanine aminotransferase adenosine triphosphate carbohydrate response element-binding protein carnitine palmityl transferase 1 cardiovascular disease cytochrome P450 4A de novo lipogenesis eicosapentaenoic acid fatty acid fatty acid synthase fatty acid binding protein free fatty acid fatty acid oxidation familial partial lipodystrophy type 3 hepatocellular carcinoma high-fat diet hepatic lipase hydroxyoctadecanoic acid hormone-sensitive lipase insulin-induced gene 1 insulin resistance insulin receptor substrate 2 interleukin long chain acyl-CoA dehydrogenase lipoprotein lipase metabolic syndrome microsomal transfer protein nonalcoholic fatty liver disease nonalcoholic steatohepatitis oxidative phosphorylation proprotein convertase subtilisin/type 9 phosphoenolpyruvate carboxykinase prostaglandin peroxisome proliferator-activated receptor γ coactivator 1 peroxisome proliferator-activated receptors PPAR response elements polyunsaturated fatty acids reactive oxygen species retinoid X receptors selective PPARγ modulators sterol regulatory element binding protein 1 triglyceride thiazolidinediones uncoupling proteins very-low-density lipoprotein Seminars in Liver Disease Vol. 35 No. 3/2015 References 1 Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 McCullough AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116(6): 1413–1419 Cohen JC, Horton JD, Hobbs HH. Human fatty liver disease: old questions and new insights. Science 2011;332(6037):1519–1523 Adams LA, Angulo P, Lindor KD. Nonalcoholic fatty liver disease. CMAJ 2005;172(7):899–905 Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 2004;40(6):1387–1395 Browning JD, Horton JD. Molecular mediators of hepatic steatosis and liver injury. J Clin Invest 2004;114(2):147–152 Korenblat KM, Fabbrini E, Mohammed BS, Klein S. Liver, muscle, and adipose tissue insulin action is directly related to intrahepatic triglyceride content in obese subjects. Gastroenterology 2008;134(5):1369–1375 Postic C, Girard J. The role of the lipogenic pathway in the development of hepatic steatosis. Diabetes Metab 2008;34(6 Pt 2):643–648 He W, Barak Y, Hevener A, et al. Adipose-specific peroxisome proliferator-activated receptor gamma knockout causes insulin resistance in fat and liver but not in muscle. Proc Natl Acad Sci U S A 2003;100(26):15712–15717 Medina-Gomez G, Gray SL, Yetukuri L, et al. PPAR gamma 2 prevents lipotoxicity by controlling adipose tissue expandability and peripheral lipid metabolism. PLoS Genet 2007;3(4):e64 Rodriguez-Cuenca S, Carobbio S, Vidal-Puig A. Ablation of Pparg2 impairs lipolysis and reveals murine strain differences in lipolytic responses. FASEB J 2012;26(5):1835–1844 Kempinska-Podhorodecka A, Krawczyk M, Klak M, et al. Healthy PNPLA3 risk allele carriers present with unexpected body fat composition. A study of one thousand subjects. J Gastrointestin Liver Dis 2014;23(1):33–37 Cusi K. Role of obesity and lipotoxicity in the development of nonalcoholic steatohepatitis: pathophysiology and clinical implications. Gastroenterology 2012;142(4):711–725.e6 Virtue S, Vidal-Puig A. Adipose tissue expandability, lipotoxicity and the Metabolic Syndrome—an allostatic perspective. Biochim Biophys Acta 2010;1801(3):338–349 Musso G, Cassader M, De Michieli F, Rosina F, Orlandi F, Gambino R. Nonalcoholic steatohepatitis versus steatosis: adipose tissue insulin resistance and dysfunctional response to fat ingestion predict liver injury and altered glucose and lipoprotein metabolism. Hepatology 2012;56(3):933–942 Kraegen EW, Clark PW, Jenkins AB, Daley EA, Chisholm DJ, Storlien LH. Development of muscle insulin resistance after liver insulin resistance in high-fat-fed rats. Diabetes 1991;40(11):1397–1403 Rolo AP, Teodoro JS, Palmeira CM. Role of oxidative stress in the pathogenesis of nonalcoholic steatohepatitis. Free Radic Biol Med 2012;52(1):59–69 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism Vacca et al. 17 Pessayre D, Fromenty B. NASH: a mitochondrial disease. J Hepatol 36 Sampath H, Miyazaki M, Dobrzyn A, Ntambi JM. Stearoyl-CoA 2005;42(6):928–940 Sanyal AJ, Campbell-Sargent C, Mirshahi F, et al. Nonalcoholic steatohepatitis: association of insulin resistance and mitochondrial abnormalities. Gastroenterology 2001;120(5):1183–1192 Fan CY, Pan J, Usuda N, Yeldandi AV, Rao MS, Reddy JK. Steatohepatitis, spontaneous peroxisome proliferation and liver tumors in mice lacking peroxisomal fatty acyl-CoA oxidase. Implications for peroxisome proliferator-activated receptor alpha natural ligand metabolism. J Biol Chem 1998;273(25):15639–15645 Sanyal AJ, Chalasani N, Kowdley KV, et al; NASH CRN. Pioglitazone, vitamin E, or placebo for nonalcoholic steatohepatitis. N Engl J Med 2010;362(18):1675–1685 Donnelly KL, Smith CI, Schwarzenberg SJ, Jessurun J, Boldt MD, Parks EJ. Sources of fatty acids stored in liver and secreted via lipoproteins in patients with nonalcoholic fatty liver disease. J Clin Invest 2005;115(5):1343–1351 Adiels M, Taskinen MR, Packard C, et al. Overproduction of large VLDL particles is driven by increased liver fat content in man. Diabetologia 2006;49(4):755–765 Fabbrini E, Mohammed BS, Magkos F, Korenblat KM, Patterson BW, Klein S. Alterations in adipose tissue and hepatic lipid kinetics in obese men and women with nonalcoholic fatty liver disease. Gastroenterology 2008;134(2):424–431 Horton JD, Shimano H, Hamilton RL, Brown MS, Goldstein JL. Disruption of LDL receptor gene in transgenic SREBP-1a mice unmasks hyperlipidemia resulting from production of lipid-rich VLDL. J Clin Invest 1999;103(7):1067–1076 Duivenvoorden I, Teusink B, Rensen PC, Romijn JA, Havekes LM, Voshol PJ. Apolipoprotein C3 deficiency results in diet-induced obesity and aggravated insulin resistance in mice. Diabetes 2005; 54(3):664–671 Lee HY, Birkenfeld AL, Jornayvaz FR, et al. Apolipoprotein CIII overexpressing mice are predisposed to diet-induced hepatic steatosis and hepatic insulin resistance. Hepatology 2011; 54(5):1650–1660 Caron S, Verrijken A, Mertens I, et al. Transcriptional activation of apolipoprotein CIII expression by glucose may contribute to diabetic dyslipidemia. Arterioscler Thromb Vasc Biol 2011; 31(3):513–519 Chen M, Breslow JL, Li W, Leff T. Transcriptional regulation of the apoC-III gene by insulin in diabetic mice: correlation with changes in plasma triglyceride levels. J Lipid Res 1994;35(11): 1918–1924 Schenk S, Saberi M, Olefsky JM. Insulin sensitivity: modulation by nutrients and inflammation. J Clin Invest 2008;118(9): 2992–3002 Mittendorfer B, Magkos F, Fabbrini E, Mohammed BS, Klein S. Relationship between body fat mass and free fatty acid kinetics in men and women. Obesity (Silver Spring) 2009;17(10): 1872–1877 Anstee QM. Animal models in nonalcoholic steatohepatitis research: utility and clinical translation. Liver Int 2011;31(4): 440–442 Miyazaki M, Flowers MT, Sampath H, et al. Hepatic stearoyl-CoA desaturase-1 deficiency protects mice from carbohydrate-induced adiposity and hepatic steatosis. Cell Metab 2007;6(6): 484–496 Bergheim I, Weber S, Vos M, et al. Antibiotics protect against fructose-induced hepatic lipid accumulation in mice: role of endotoxin. J Hepatol 2008;48(6):983–992 Feldstein AE, Canbay A, Guicciardi ME, Higuchi H, Bronk SF, Gores GJ. Diet associated hepatic steatosis sensitizes to Fas mediated liver injury in mice. J Hepatol 2003;39(6):978–983 Kennedy AR, Pissios P, Otu H, et al. A high-fat, ketogenic diet induces a unique metabolic state in mice. Am J Physiol Endocrinol Metab 2007;292(6):E1724–E1739 desaturase-1 mediates the pro-lipogenic effects of dietary saturated fat. J Biol Chem 2007;282(4):2483–2493 Romestaing C, Piquet MA, Bedu E, et al. Long term highly saturated fat diet does not induce NASH in Wistar rats. Nutr Metab (Lond) 2007;4:4 Newberry EP, Xie Y, Kennedy SM, Luo J, Davidson NO. Protection against Western diet-induced obesity and hepatic steatosis in liver fatty acid-binding protein knockout mice. Hepatology 2006; 44(5):1191–1205 Pfluger PT, Herranz D, Velasco-Miguel S, Serrano M, Tschöp MH. Sirt1 protects against high-fat diet-induced metabolic damage. Proc Natl Acad Sci U S A 2008;105(28):9793–9798 Singh R, Wang Y, Xiang Y, Tanaka KE, Gaarde WA, Czaja MJ. Differential effects of JNK1 and JNK2 inhibition on murine steatohepatitis and insulin resistance. Hepatology 2009;49(1): 87–96 Tetri LH, Basaranoglu M, Brunt EM, Yerian LM, NeuschwanderTetri BA. Severe NAFLD with hepatic necroinflammatory changes in mice fed trans fats and a high-fructose corn syrup equivalent. Am J Physiol Gastrointest Liver Physiol 2008;295(5):G987–G995 Koppe SW, Elias M, Moseley RH, Green RM. Trans fat feeding results in higher serum alanine aminotransferase and increased insulin resistance compared with a standard murine high-fat diet. Am J Physiol Gastrointest Liver Physiol 2009;297(2):G378–G384 Obara N, Fukushima K, Ueno Y, et al. Possible involvement and the mechanisms of excess trans-fatty acid consumption in severe NAFLD in mice. J Hepatol 2010;53(2):326–334 Sekiya M, Yahagi N, Matsuzaka T, et al. Polyunsaturated fatty acids ameliorate hepatic steatosis in obese mice by SREBP-1 suppression. Hepatology 2003;38(6):1529–1539 Baumgardner JN, Shankar K, Hennings L, Badger TM, Ronis MJ. A new model for nonalcoholic steatohepatitis in the rat utilizing total enteral nutrition to overfeed a high-polyunsaturated fat diet. Am J Physiol Gastrointest Liver Physiol 2008;294(1): G27–G38 Denechaud PD, Bossard P, Lobaccaro JM, et al. ChREBP, but not LXRs, is required for the induction of glucose-regulated genes in mouse liver. J Clin Invest 2008;118(3):956–964 Repa JJ, Liang G, Ou J, et al. Regulation of mouse sterol regulatory element-binding protein-1c gene (SREBP-1c) by oxysterol receptors, LXRalpha and LXRbeta. Genes Dev 2000;14(22):2819–2830 Horton JD, Goldstein JL, Brown MS. SREBPs: activators of the complete program of cholesterol and fatty acid synthesis in the liver. J Clin Invest 2002;109(9):1125–1131 Li Y, Xu S, Mihaylova MM, et al. AMPK phosphorylates and inhibits SREBP activity to attenuate hepatic steatosis and atherosclerosis in diet-induced insulin-resistant mice. Cell Metab 2011; 13(4):376–388 Takaishi K, Duplomb L, Wang MY, Li J, Unger RH. Hepatic insig-1 or -2 overexpression reduces lipogenesis in obese Zucker diabetic fatty rats and in fasted/refed normal rats. Proc Natl Acad Sci U S A 2004;101(18):7106–7111 Engelking LJ, Kuriyama H, Hammer RE, et al. Overexpression of Insig-1 in the livers of transgenic mice inhibits SREBP processing and reduces insulin-stimulated lipogenesis. J Clin Invest 2004; 113(8):1168–1175 Shimomura I, Matsuda M, Hammer RE, Bashmakov Y, Brown MS, Goldstein JL. Decreased IRS-2 and increased SREBP-1c lead to mixed insulin resistance and sensitivity in livers of lipodystrophic and ob/ob mice. Mol Cell 2000;6(1):77–86 Ide T, Shimano H, Yahagi N, et al. SREBPs suppress IRS-2mediated insulin signalling in the liver. Nat Cell Biol 2004;6(4): 351–357 Towle HC, Kaytor EN, Shih HM. Regulation of the expression of lipogenic enzyme genes by carbohydrate. Annu Rev Nutr 1997; 17:405–433 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 Seminars in Liver Disease Vol. 35 No. 3/2015 259 260 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism Vacca et al. 55 Iizuka K, Horikawa Y. ChREBP: a glucose-activated transcription 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 factor involved in the development of metabolic syndrome. Endocr J 2008;55(4):617–624 Dentin R, Benhamed F, Hainault I, et al. Liver-specific inhibition of ChREBP improves hepatic steatosis and insulin resistance in ob/ ob mice. Diabetes 2006;55(8):2159–2170 Benhamed F, Denechaud PD, Lemoine M, et al. The lipogenic transcription factor ChREBP dissociates hepatic steatosis from insulin resistance in mice and humans. J Clin Invest 2012;122(6): 2176–2194 Aarsland A, Wolfe RR. Hepatic secretion of VLDL fatty acids during stimulated lipogenesis in men. J Lipid Res 1998;39(6):1280–1286 Korchak HM. Regulation of hepatic lipogenesis. Tufts Folia Med 1962;8:134–143 Bookout AL, Jeong Y, Downes M, Yu RT, Evans RM, Mangelsdorf DJ. Anatomical profiling of nuclear receptor expression reveals a hierarchical transcriptional network. Cell 2006;126(4):789–799 Mangelsdorf DJ, Thummel C, Beato M, et al. The nuclear receptor superfamily: the second decade. Cell 1995;83(6):835–839 Mangelsdorf DJ, Evans RM. The RXR heterodimers and orphan receptors. Cell 1995;83(6):841–850 Christodoulides C, Vidal-Puig A. PPARs and adipocyte function. Mol Cell Endocrinol 2010;318(1-2):61–68 Atherton HJ, Gulston MK, Bailey NJ, et al. Metabolomics of the interaction between PPAR-alpha and age in the PPAR-alpha-null mouse. Mol Syst Biol 2009;5:259 Le May C, Pineau T, Bigot K, Kohl C, Girard J, Pégorier JP. Reduced hepatic fatty acid oxidation in fasting PPARalpha null mice is due to impaired mitochondrial hydroxymethylglutaryl-CoA synthase gene expression. FEBS Lett 2000;475(3):163–166 Vu-Dac N, Gervois P, Jakel H, et al. Apolipoprotein A5, a crucial determinant of plasma triglyceride levels, is highly responsive to peroxisome proliferator-activated receptor alpha activators. J Biol Chem 2003;278(20):17982–17985 Schoonjans K, Peinado-Onsurbe J, Lefebvre AM, et al. PPARalpha and PPARgamma activators direct a distinct tissue-specific transcriptional response via a PPRE in the lipoprotein lipase gene. EMBO J 1996;15(19):5336–5348 Wolfrum C, Borrmann CM, Borchers T, Spener F. Fatty acids and hypolipidemic drugs regulate peroxisome proliferator-activated receptors alpha - and gamma-mediated gene expression via liver fatty acid binding protein: a signaling path to the nucleus. Proc Natl Acad Sci U S A 2001;98(5):2323–2328 Martin G, Schoonjans K, Lefebvre AM, Staels B, Auwerx J. Coordinate regulation of the expression of the fatty acid transport protein and acyl-CoA synthetase genes by PPARalpha and PPARgamma activators. J Biol Chem 1997;272(45):28210–28217 Fruchart JC. Peroxisome proliferator-activated receptor-alpha (PPARalpha): at the crossroads of obesity, diabetes and cardiovascular disease. Atherosclerosis 2009;205(1):1–8 Staels B, Dallongeville J, Auwerx J, Schoonjans K, Leitersdorf E, Fruchart JC. Mechanism of action of fibrates on lipid and lipoprotein metabolism. Circulation 1998;98(19):2088–2093 Vacca M, Degirolamo C, Mariani-Costantini R, Palasciano G, Moschetta A. Lipid-sensing nuclear receptors in the pathophysiology and treatment of the metabolic syndrome. Wiley Interdiscip Rev Syst Biol Med 2011;3(5):562–587 Shah A, Rader DJ, Millar JS. The effect of PPAR-alpha agonism on apolipoprotein metabolism in humans. Atherosclerosis 2010; 210(1):35–40 Ip E, Farrell GC, Robertson G, Hall P, Kirsch R, Leclercq I. Central role of PPARalpha-dependent hepatic lipid turnover in dietary steatohepatitis in mice. Hepatology 2003;38(1):123–132 Abdelmegeed MA, Yoo SH, Henderson LE, Gonzalez FJ, Woodcroft KJ, Song BJ. PPARalpha expression protects male mice from high fat-induced nonalcoholic fatty liver. J Nutr 2011;141(4):603–610 Su Q, Baker C, Christian P, et al. Hepatic mitochondrial and ER stress induced by defective PPARα signaling in the pathogenesis Seminars in Liver Disease Vol. 35 No. 3/2015 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 of hepatic steatosis. Am J Physiol Endocrinol Metab 2014; 306(11):E1264–E1273 Chan SM, Sun RQ, Zeng XY, et al. Activation of PPARα ameliorates hepatic insulin resistance and steatosis in high fructose-fed mice despite increased endoplasmic reticulum stress. Diabetes 2013; 62(6):2095–2105 Stienstra R, Mandard S, Patsouris D, Maass C, Kersten S, Müller M. Peroxisome proliferator-activated receptor alpha protects against obesity-induced hepatic inflammation. Endocrinology 2007;148(6):2753–2763 Shiri-Sverdlov R, Wouters K, van Gorp PJ, et al. Early diet-induced non-alcoholic steatohepatitis in APOE2 knock-in mice and its prevention by fibrates. J Hepatol 2006;44(4):732–741 Laurin J, Lindor KD, Crippin JS, et al. Ursodeoxycholic acid or clofibrate in the treatment of non-alcohol-induced steatohepatitis: a pilot study. Hepatology 1996;23(6):1464–1467 Fernández-Miranda C, Pérez-Carreras M, Colina F, López-Alonso G, Vargas C, Solís-Herruzo JA. A pilot trial of fenofibrate for the treatment of non-alcoholic fatty liver disease. Dig Liver Dis 2008; 40(3):200–205 Barish GD, Narkar VA, Evans RM. PPAR delta: a dagger in the heart of the metabolic syndrome. J Clin Invest 2006;116(3):590–597 Grimaldi PA. Regulatory functions of PPARbeta in metabolism: implications for the treatment of metabolic syndrome. Biochim Biophys Acta 2007;1771(8):983–990 Berger J, Leibowitz MD, Doebber TW, et al. Novel peroxisome proliferator-activated receptor (PPAR) gamma and PPARdelta ligands produce distinct biological effects. J Biol Chem 1999; 274(10):6718–6725 Coleman JD, Prabhu KS, Thompson JT, et al. The oxidative stress mediator 4-hydroxynonenal is an intracellular agonist of the nuclear receptor peroxisome proliferator-activated receptorbeta/delta (PPARbeta/delta). Free Radic Biol Med 2007;42(8): 1155–1164 Wang YX, Lee CH, Tiep S, et al. Peroxisome-proliferator-activated receptor delta activates fat metabolism to prevent obesity. Cell 2003;113(2):159–170 Roberts LD, Hassall DG, Winegar DA, Haselden JN, Nicholls AW, Griffin JL. Increased hepatic oxidative metabolism distinguishes the action of Peroxisome proliferator-activated receptor delta from Peroxisome proliferator-activated receptor gamma in the ob/ob mouse. Genome Med 2009;1(12):115 Barroso E, Rodríguez-Calvo R, Serrano-Marco L, et al. The PPARβ/δ activator GW501516 prevents the down-regulation of AMPK caused by a high-fat diet in liver and amplifies the PGC-1α-Lipin 1-PPARα pathway leading to increased fatty acid oxidation. Endocrinology 2011;152(5):1848–1859 Liu S, Hatano B, Zhao M, et al. Role of peroxisome proliferatoractivated receptor delta/beta in hepatic metabolic regulation. J Biol Chem 2011;286(2):1237–1247 Qin X, Xie X, Fan Y, et al. Peroxisome proliferator-activated receptor-delta induces insulin-induced gene-1 and suppresses hepatic lipogenesis in obese diabetic mice. Hepatology 2008; 48(2):432–441 Serrano-Marco L, Barroso E, El Kochairi I, et al. The peroxisome proliferator-activated receptor (PPAR) β/δ agonist GW501516 inhibits IL-6-induced signal transducer and activator of transcription 3 (STAT3) activation and insulin resistance in human liver cells. Diabetologia 2012;55(3):743–751 Nagasawa T, Inada Y, Nakano S, et al. Effects of bezafibrate, PPAR pan-agonist, and GW501516, PPARdelta agonist, on development of steatohepatitis in mice fed a methionine- and choline-deficient diet. Eur J Pharmacol 2006;536(1-2):182–191 Vu-Dac N, Chopin-Delannoy S, Gervois P, et al. The nuclear receptors peroxisome proliferator-activated receptor alpha and Rev-erbalpha mediate the species-specific regulation of apolipoprotein A-I expression by fibrates. J Biol Chem 1998;273(40): 25713–25720 Fatty Acid and Glucose Sensors in Hepatic Lipid Metabolism 94 Tanaka T, Yamamoto J, Iwasaki S, et al. Activation of peroxisome 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 proliferator-activated receptor delta induces fatty acid betaoxidation in skeletal muscle and attenuates metabolic syndrome. Proc Natl Acad Sci U S A 2003;100(26):15924–15929 Leibowitz MD, Fiévet C, Hennuyer N, et al. Activation of PPARdelta alters lipid metabolism in db/db mice. FEBS Lett 2000;473(3): 333–336 Oliver WR Jr, Shenk JL, Snaith MR, et al. A selective peroxisome proliferator-activated receptor delta agonist promotes reverse cholesterol transport. Proc Natl Acad Sci U S A 2001;98(9): 5306–5311 Wallace JM, Schwarz M, Coward P, et al. Effects of peroxisome proliferator-activated receptor alpha/delta agonists on HDL-cholesterol in vervet monkeys. J Lipid Res 2005;46(5):1009–1016 Kostadinova R, Montagner A, Gouranton E, et al. GW501516activated PPARβ/δ promotes liver fibrosis via p38-JNK MAPKinduced hepatic stellate cell proliferation. Cell Biosci 2012;2(1): 34 Vacca M, Degirolamo C, Massafra V, et al. Nuclear receptors in regenerating liver and hepatocellular carcinoma. Mol Cell Endocrinol 2013;368(1-2):108–119 Vacca M, D’Amore S, Graziano G, et al. Clustering nuclear receptors in liver regeneration identifies candidate modulators of hepatocyte proliferation and hepatocarcinoma. PLoS ONE 2014; 9(8):e104449 Savage DB, Tan GD, Acerini CL, et al. Human metabolic syndrome resulting from dominant-negative mutations in the nuclear receptor peroxisome proliferator-activated receptor-gamma. Diabetes 2003;52(4):910–917 Barroso I, Gurnell M, Crowley VE, et al. Dominant negative mutations in human PPARgamma associated with severe insulin resistance, diabetes mellitus and hypertension. Nature 1999; 402(6764):880–883 Semple RK, Chatterjee VK, O’Rahilly S. PPAR gamma and human metabolic disease. J Clin Invest 2006;116(3):581–589 Jeninga EH, Gurnell M, Kalkhoven E. Functional implications of genetic variation in human PPARgamma. Trends Endocrinol Metab 2009;20(8):380–387 Gawrieh S, Marion MC, Komorowski R, et al. Genetic variation in the peroxisome proliferator activated receptor-gamma gene is associated with histologically advanced NAFLD. Dig Dis Sci 2012; 57(4):952–957 Krey G, Braissant O, L’Horset F, et al. Fatty acids, eicosanoids, and hypolipidemic agents identified as ligands of peroxisome proliferator-activated receptors by coactivator-dependent receptor ligand assay. Mol Endocrinol 1997;11(6):779–791 Dyson JK, Anstee QM, McPherson S. Non-alcoholic fatty liver disease: a practical approach to treatment. Frontline Gastroenterol 2014;5(4):277–286 Chao L, Marcus-Samuels B, Mason MM, et al. Adipose tissue is required for the antidiabetic, but not for the hypolipidemic, effect of thiazolidinediones. J Clin Invest 2000;106(10):1221–1228 Maeda N, Takahashi M, Funahashi T, et al. PPARgamma ligands increase expression and plasma concentrations of adiponectin, an adipose-derived protein. Diabetes 2001;50(9):2094–2099 Collino M, Aragno M, Castiglia S, et al. Pioglitazone improves lipid and insulin levels in overweight rats on a high cholesterol and 111 112 113 114 115 116 117 118 119 120 121 122 123 124 125 Vacca et al. fructose diet by decreasing hepatic inflammation. Br J Pharmacol 2010;160(8):1892–1902 Hevener AL, Olefsky JM, Reichart D, et al. Macrophage PPAR gamma is required for normal skeletal muscle and hepatic insulin sensitivity and full antidiabetic effects of thiazolidinediones. J Clin Invest 2007;117(6):1658–1669 Hevener AL, He W, Barak Y, et al. Muscle-specific Pparg deletion causes insulin resistance. Nat Med 2003;9(12):1491–1497 Norris AW, Chen L, Fisher SJ, et al. Muscle-specific PPARgammadeficient mice develop increased adiposity and insulin resistance but respond to thiazolidinediones. J Clin Invest 2003;112(4): 608–618 Lee YJ, Ko EH, Kim JE, et al. Nuclear receptor PPARγ-regulated monoacylglycerol O-acyltransferase 1 (MGAT1) expression is responsible for the lipid accumulation in diet-induced hepatic steatosis. Proc Natl Acad Sci U S A 2012;109(34): 13656–13661 Morán-Salvador E, López-Parra M, García-Alonso V, et al. Role for PPARγ in obesity-induced hepatic steatosis as determined by hepatocyte- and macrophage-specific conditional knockouts. FASEB J 2011;25(8):2538–2550 Yu S, Matsusue K, Kashireddy P, et al. Adipocyte-specific gene expression and adipogenic steatosis in the mouse liver due to peroxisome proliferator-activated receptor gamma1 (PPARgamma1) overexpression. J Biol Chem 2003;278(1):498–505 Cheng AY, Fantus IG. Oral antihyperglycemic therapy for type 2 diabetes mellitus. CMAJ 2005;172(2):213–226 Finck BN, Kelly DP. PGC-1 coactivators: inducible regulators of energy metabolism in health and disease. J Clin Invest 2006; 116(3):615–622 Leone TC, Lehman JJ, Finck BN, et al. PGC-1alpha deficiency causes multi-system energy metabolic derangements: muscle dysfunction, abnormal weight control and hepatic steatosis. PLoS Biol 2005;3(4):e101 Estall JL, Kahn M, Cooper MP, et al. Sensitivity of lipid metabolism and insulin signaling to genetic alterations in hepatic peroxisome proliferator-activated receptor-gamma coactivator-1alpha expression. Diabetes 2009;58(7):1499–1508 Purushotham A, Schug TT, Xu Q, Surapureddi S, Guo X, Li X. Hepatocyte-specific deletion of SIRT1 alters fatty acid metabolism and results in hepatic steatosis and inflammation. Cell Metab 2009;9(4):327–338 Lin J, Yang R, Tarr PT, et al. Hyperlipidemic effects of dietary saturated fats mediated through PGC-1beta coactivation of SREBP. Cell 2005;120(2):261–273 Lelliott CJ, Medina-Gomez G, Petrovic N, et al. Ablation of PGC1beta results in defective mitochondrial activity, thermogenesis, hepatic function, and cardiac performance. PLoS Biol 2006;4(11): e369 Sonoda J, Mehl IR, Chong LW, Nofsinger RR, Evans RM. PGC-1beta controls mitochondrial metabolism to modulate circadian activity, adaptive thermogenesis, and hepatic steatosis. Proc Natl Acad Sci U S A 2007;104(12):5223–5228 Bellafante E, Murzilli S, Salvatore L, Latorre D, Villani G, Moschetta A. Hepatic-specific activation of peroxisome proliferator-activated receptor γ coactivator-1β protects against steatohepatitis. Hepatology 2013;57(4):1343–1356 Seminars in Liver Disease Vol. 35 No. 3/2015 261