Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
DNA supercoil wikipedia , lookup
Non-coding DNA wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Cre-Lox recombination wikipedia , lookup
Genome evolution wikipedia , lookup
Genomic library wikipedia , lookup
Hybrid (biology) wikipedia , lookup
Genetic engineering wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Gene expression programming wikipedia , lookup
Dominance (genetics) wikipedia , lookup
Point mutation wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Extrachromosomal DNA wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Genomic imprinting wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
History of genetic engineering wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Y chromosome wikipedia , lookup
Genome (book) wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Fetal origins hypothesis wikipedia , lookup
Neocentromere wikipedia , lookup
Designer baby wikipedia , lookup
Microevolution wikipedia , lookup
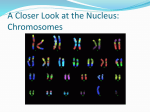
PowerPoint Summary of Chapters 23-25 • Use this PowerPoint along with the outline notes • If a term appears in bold and is not defined, be sure to go look on the text for it • Refer back to the text for any additional info you would like to have • Have fun! Chapter 23 Reproductive System • Meiosis – A form of cell division specific to gametes that results in only half the number of original chromosomes (fig 21-1) – Stem cells (46 chromosomes) divide into functional gametes which only have 23 chromosomes – For males, this process doesn’t start until puberty and continues throughout the rest of their life • Once started, males will produce 500,000 spermatozoa per day. • Spermatogenesis – creation of sperm – A single stem cell divides twice to produce four spermatozoa (sperm cell) – This process occurs along the nearly half mile of seminiferous tubules in each testis – The seminiferous tubules drain into the epididymus. There spermatozoa mature up to 2 weeks in the super coiled 23 ft of tubule. – The next part of the pathway is the ductus deferens (vas deferens) that runs from the posterior of each testis to a single ejaculatory duct. • Sperm can be stored in the ductus deferens for several months • Spermatogenesis – (cont’d) – Accessory glands add to the seminal fluid at the ejaculatory ducts and proximal end of the urethra. • Seminal Vesicles • Prostate Gland • Bulbourethral (see fig 23-1 for location of these glands) – What are the functions of semen? • Spermatogenesis – (cont’d) – The urethra is the final path for seminal fluid as it travels through the penis and is ejaculated out of the body • A typical ejaculate is 2 to 5 ml of semen and contains 50-100 million sperm per ml – Interstitial cells between the seminiferous tubules produce the hormone testosterone. • This production increase dramatically after puberty in the presence of FSH and LH – Refer back to Chapter 12 about the regulation and production of these hormones • Oogenesis – formation of an egg (ovum) – Stem cells during prenatal development divide twice to produce an ovum with 23 chromosomes • Each female is born with nearly 2 million ovum, but by the time they will start being released at puberty, the number withers down to ~200,000. All are stored in a pair of ovaries. – Levels of FSH and LH stimulate the development and release • Even so, she will only release less than 400 in a lifetime. One per month, alternating from the right or left ovary. • This process will end with menopause. • Oogenesis – formation of an egg (ovum) – One ovum from the left or right ovary is ovulated into the fimbriae of the 5 inch uterine tube • Cilia in the tube draw the ovum towards the uterus; a trip that takes 3-4 days – This cycle usually lasts about 28 days, but can be longer or shorter per individual • Increased LH levels stimulate the development of a follicle, which will then release its ovum in 14days • Fertilization needs to occur in the first 48 hrs after ovulation or the ovum will disintegrate in the uterus and be flushed out during menstration. • If fertilizations does occur, then the cycle is stopped until after birth • Read both the menstrual cycle which starts on page 466 • Review fig. 23-13 which summarizes the hormonal events and uterus development for this cycle. • Read the Hot Topic (Box 23-3) and Birth Control Strategies on pages 468 and 469 • Be familiar with the types of cancer of this system – Prostatic, Testicular, Breast, Endometrial, Ovarian, Cervical Chapter 24 Development • Begins at fertilization, or conception and ends at birth – Gestation lasts approximately 38 weeks • Prenatal development is divided into two stages – Embryo for the first two months – Fetus from the ninth week to birth • Fertilization – Fusion of egg and sperm – Each contain 23 chromosomes to form a zygote containing 46 chromosomes – 200 million sperm are released into the vagina, 10,000 make it into the uterine tube, and about 100 may actually make it to the egg. – Penetration of the egg by a single sperm allows the chromosomes to combine Gestation • Average prenatal period is 38 weeks or 266 days (divided into three trimesters) • First Trimester – 40% of the eggs that are fertilized produce embryos that survive the first trimester – Embryo formation • Zygote undergoes rapid cell divisions called cleavage • By day 5, the cells have entered the uterus, and developed into a blastocyst • First Trimester continued – Implantation • About day 7, the blastocyst adheres to the surface of the uterus and will become completely embedded within its membrane – The outer cells of the blastocyst develops into the placenta • The placenta begins secreting human chorionic gonadotropin (hGC) which signals the corpus luteum to maintain production of estrogens and progesterone – This hormone maintains a functional endometrial lining • The inner cell mass of the blastocyst becomes organized into three germ layers that will form different body tissues • First Trimester continued – Placenta (fig 24-2) • Extensions from the chorion extend into maternal tissue where chorionic blood vessels develop • These chorionic villi enlarge as the heart starts beating and extend further into the endometrium where they will come in close proximity of maternal blood vessels • The vessels develop into two umbilical arteries and a single umbilical vein • The chorionic villi provide the surface area for the exchange of gasses, nutrients and wastes between maternal and fetal blood flow. • First Trimester continued – Placenta (cont’d) • Also releases hormones (progesterone and estrogen) which will take over for the declining corpus luteum • Prevents menstration, prepares mammary glands to produce milk, and prepare the body for delivery • The following slide shows embryos at different stages and an early fetus – Interesting note: Picture b is during a phase where we don’t look too much different from fish or chicken embryo • Second and Third Trimester – The framework for the major organ systems have formed by the start of the second trimester • The fetus grows from ~1oz to 1.4lbs – Those organ systems become mostly functional in the third trimester • The fetus gains most its weight and shoots up to an average of 7lbs Changes • The fetus is totally dependant on the mother’s organ systems – That means that the mother has to increase all her norms to provide proper nutrition to the developing fetus • Increase CV activity, blood volume, Respiratory Rate, appetite, and excretion Changes • Early contractions of uterine smooth muscle are weak, short and painless – Late in development rising estrogen levels increase smooth muscle sensitivity and stimulate an rise in oxytocin levels. – Oxytocin increases the force and frequency of contractions in response to a stretch in the uterine cervix – Uterine tissues also produce prostaglandins that increase contractions as well • Typically at 9 months, these changes lead to labor contractions that continue until delivery has been completed. Stages of Labor (Parturition) • First Stage – Cervix dilates and the fetus begins to slide down the cervical canal – Labor contractions are once every 10 to 30 min and at some point the amnion will rupture releasing amniotic fluid (“water break”) • Second Stage – Starts after the cervix has dilated completely and concludes when the fetus emerges from the vagina – Time varies but usually lasts two hours or less Stages of Labor (Parturition) • Third Stage – This stage ends with the ejection of the placenta (“afterbirth”) and an associated blood loss of 500600ml. • Along with the placenta, the amniotic sac membranes, and the umbilical cord (except the part attached to the baby which forms the umbilicus) are ejected • Fourth Stage – The period the body controls the bleeding after the birth – Involves uterine contractions and repair of an episiotomy, if conducted. Stages of Labor • An episiotomy can be performed to prevent perineal tearing if the vaginal opening is too small – This procedure enlarges the vaginal opening by placing an incision through the perineal musculature between the vagina and anus. It can be repaired with sutures after delivery • A Cesarean (C) section can be performed if complications arise – Here the abdominal wall is opened and a 6-7 inch incision is made in the uterus to allow the head (the widest part) to pass through Multiple Births • New stats on births reveals that twins occur 1 in 100 births and with African-Americans, the rate is greater (1 in 77) • Fraternal twins are created when two eggs are released and fertilized at the same time. May or may not be the same gender. • Identical twins are produced when the fertilized zygote cells split apart during development. The offspring’s genetic makeup is exactly the same. – Fraternal twins are twice as common as identical twins and are increasing with the practice of fertility medicine. Genetics and Inheritance Chapter 25 • Genetics is the study of heredity, or how different traits are inherited. • Families have similar traits because they are passed on from generation to generation through their chromosomes Genes and Chromosomes • Chromosomes contain DNA (Chapter 2 if you forgot) – No cell uses every bit of its genetic information – Genes are functional segments of DNA • Every somatic cell carries copies of the 46 original chromosomes that were in the zygote – Except gametes / RBCs figure 2 Genes and Chromosomes • Genotype – Chromosomes and their component genes ►Arrangement of nucleotide bases – ATGCGCCCCATA or AGCCGCATAGCG… • Phenotype – physical expression of the genotype ►Hair color, skin tone, vision, bone structure * The genotype dictates the phenotype • A gene’s position on a chromosome is called a locus – The locus helps map the DNA strand to indicate which section is responsible for certain traits • Each DNA strand has a “partner” within the nucleus – This pairing is referred to as Homologous Chromosomes, with one strand coming from paternal DNA and the other from maternal DNA Karyotyping • a sample of amniotic fluid is taken (amniocentesis) and fetal DNA is analyzed • a Karyotype displays homologous pairs of chromosomes • Sampling procedures can be dangerous to the fetus and mother – Amniocentesis is only performed when known risk factors are present • I.e. Family history, age complications, drug user, etc. – Amniotic fluid has to be sufficienct enough to be taken without implication to the fetus • Usually at a gestational age of 14 weeks • Results take several weeks Patterns of inheritance • Somatic cells contain 23 pairs of chromosomes – All 23 are Homologous chromosomes – 22 pair of autosomal and one pair of sex chromosomes • Various forms of a gene are called alleles • Homozygous if homologous chromosomes carry the same alleles - AA, or aa • Heterozygous if homologous chromosomes carry different alleles - Aa • Alleles are either dominant – Always expressed in the phenotype – Usually represented by a capital letter (A) • or recessive – Expressed only when both alleles are present – Usually represented by a lowercase letter (a) • Incomplete Dominance – Phenotype that is different from phenotypes of homozygous for either allele – Example: Sickle cell – Recessive trait (s) that causes RBCs to fold • ss: individual has the sickle cell disorder • Ss: individual has RBCs that fold only when tissue O2 levels drop • Codominance – Heterozygous allele that shows both traits in its phenotype – Example: Blood type • IA: antigen A present • IB: antigen B present • i: no antigen present • • • • ii = Type O IB IB or IB i = Type B IA IA or IA i = Type A IA IB = Type AB • Teratogens – factors that disrupt normal development by damaging cells, altering chromosome structure, or by changing the pattern of gene activation and expression. – Examples are nicotine, radiation, and alcohol – Fetal alcohol syndrome (FAS) produces developmental defects caused by mothers who drink during pregnancy • Number 1 cause of mental retardation in the U.S. Punnett square diagram predicts probabilities of traits A = normal color, a = albino (see next slide) • In diagram A, a homozygous dominate male mates with a homozygous recessive female – The probability of them having offspring with normal pigment is 100% (all are heterozygous dominant) • In diagram B, a heterozygous dominant male mates with a homozygous recessive female – The probability that they will have normal pigment offspring is 50%, the other 50% have albinism Inheritance • Simple inheritance – Phenotypic characteristics are determined by interactions between single pair of alleles • Polygenic inheritance – Phenotypic characteristics are determined by interactions among alleles on several genes Inheritance • More than 1200 inherited conditions have been identified that are linked to 1 or 2 abnormal alleles for a single gene Sources of Individual Variation • Genetic recombination – Gene reshuffling, common, creates variations within a gene pool • Crossing over and translocation (fig next slide) – Occurs during meiosis – May produce abnormal chromosomes • The production of chromosomes with extra or missing segments • Most result in miscarriages but some result in developmental disorders Crossover and Translocation • Spontaneous mutations – Random errors in DNA replication where extra or missing code occurs – Many of these errors are hidden as the recessive trait, and some don’t make it past the embryo stage – Heterozygous for the abnormal trait would be a carrier Sex-Linked Inheritance • Sex chromosomes are X chromosome and Y chromosome – Male = XY – Female = XX – X chromosome carries X-linked (sex linked) genes • Affect somatic structures • The X chromosome is longer therefore no corresponding alleles on Y chromosome (i.e. no competition for traits) Sex-linked Punnett Human Genome Project • Mapped ~24,000 of our genes – Including some responsible for inherited disorders click for more Human Genome info click for DNA sequence list DNA Map Genetic Disorders • Mistakes caused during meiosis – Extra copies or missing pieces of DNA • Down Syndrome – Most common chromosomal abnormality – Caused by an extra copy of chromosome #21 – Marked by mental retardation of various levels and specific common physical features – Most die early of cardiovascular problems or develop neurological problems as they age – Incidence increases as the age of the mother being impregnated increases after age 35. Genetic Disorders • Klinefelter Syndrome – Male with an extra X chromosome – Reduces testosterone production so testis fail to mature, individuals are sterile, and breasts enlarge • Turner Syndrome – Female with a single X chromosome – Therefore a chromosome short – Causes an absence of development at puberty, ovaries are non-functional, and estrogen production is insignificant. – Will require hormone injections to develop adult female characteristics Ectopic (“displaced”) Pregnancies • Normal implantation occurs in the endometrial lining of the uterus, ectopics implant somewhere else. • 95% implant in the uterine tube which cannot expand like the uterus. – The developing embryo ruptures the tube which causes internal bleeding and a risk to the mother – In some cases, the embryo can continue to develop full term and with surgical removal at birth • Incidence increases with regular douching or uterine tube infection Placenta Problems • Placenta Previa – Implantation occurs in the lower portion of the uterus – The placenta then may form near or over the cervical opening which increases the risk of tearing and bleeding out – Treatment includes bed rest for the mother and a scheduled C section when gestation has reached a safe point • Abrupto Placentae – Placenta tears away from the uterus after the fifth month of gestation – Internal bleeding may lead to maternal anemia or shock – Fetal mortality is between 30 and 100%