Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Sensory substitution wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Synaptogenesis wikipedia , lookup
Central pattern generator wikipedia , lookup
Amyotrophic lateral sclerosis wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuroregeneration wikipedia , lookup
Proprioception wikipedia , lookup
End-plate potential wikipedia , lookup
Embodied language processing wikipedia , lookup
Microneurography wikipedia , lookup
Electromyography wikipedia , lookup
Muscle memory wikipedia , lookup
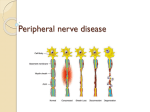
NEUROMUSCULAR EMERGENCIES July 28, 2010 Sandra Derghazarian Outline • Approach to rapidly progressing LMN weakness • Myasthenic crisis • GBS Intro • Three major tasks: – Assess stability, signs of imminent resp failure – Generate differential diagnosis • Knowledge of localisation • Knowledge of major disorders – Determine management Brief Review of Anatomy • Motor unit anatomy – Anterior horn cell – Its motor axon – The synaptic cleft – The muscle fibers it innervates • Remember sensory and autonomic systems – Many disorder with rapidly progressing peripheral neuropathic weakness will have sensory loss and dysautonomia Classification • Motor neuron – Loss of anterior horn cells • Motor axon – Disruption of myelin sheath – Axonal degeneration • Neuromuscular junction – Pre-synaptic (e.g. Release of Ach) – Post-synaptic (e.g. Abnormalities of Ach receptor) • Muscle – Membrane, contractile elements – Genetic or acquired secondary (infex, inflamm, vasc.) Approach to Determining Cause of Weakness • • • • Knowledge of some of the possible disorders Focused history Physical exam Lab studies Major Disorders Level of motor unit Disorders causing rapidly progressing weakness Motor neuron ALS Poliomyelitis, West Nile virus Peripheral nerve Guillain-Barre syndrome/AIDP Tick paralysis Diphtheric, porphyric, arsenic neuropathy Shellfish poisoning Neuromuscular junction Myasthenia gravis Botulism Lambert-Eaten myasthenic syndrome Hypermagnesemia Muscle Acquired: Dermato- and polymyositis, Myoglobinuric myopathy, Hypokalemic paralysis, Toxic myopathy, Acute myopathy of intensive care Genetic disorders: X-linked dystrophies, myotonic dystrophy, acid maltase deficiency, mitochondrial History – Key Elements • Pre-existing NM disorder? – MG – exacerbation 2ary systemic illness, medication – ALS – accelerated phase, decompensation 2ary pneumonia • Pre-existing systemic disorder? – Malignancy, CTD, sepsis • What drugs is pt taking? • Any recent illness? • Diet in last 48 hours? – Shellfish (saxitoxin, brevetoxin) – Home-canned goods (botulinum toxin) • Any possible exposure to tick bite, snake bite? • Any sensory or autonomic symptoms? Drugs • Diuretics – Hypokalemia • Corticosteroids, statins, colchicine, cyclosporine, cocaine, chloroquine, L-tryptophan, penicillamine, zidovudine – Myotoxic effect • Amiodarone, cytarabine, streptokinase – Demyelinating neuropathy • Magnesium-containing antacids with pre-existing renal insufficiency – Hypermagnesemia Physical Exam • Vital signs – Unstable? – Dysautonomia? • Respiratory status Signs of impending NM resp failure • • • • • • • • Tachypnea, sinus tachycardia Staccato speech Inability to count to 20 Profound weakness of neck flexion Use of accessory muscles (visible, palpable) Orthopnea Paradoxical breathing pattern Signs of bulbar dysfunction (nasal voice, accumulation of saliva, weak cough) – think about aspiration! Physical Exam Physical Exam • Vital signs • Note any dysautonomia • Presence and pattern muscle weakness • Proximal (myopathy), distal (peripheral neuropathy) • Symmetric, asymmetric • Involvement of cranial muscles • Reflexes • Sensory changes • Dysautonomia Localisation of the Disorders • Clinical picture varies depending on which part of motor unit is involved Level of motor unit Key Clinical Feature Motor neuron Predominantly motor signs Often asymmetric Occasional sensory signs DTRs may be increased if ALS Peripheral nerve Weakness and sensory signs +/- autonomic signs +/- cranial muscles DTRs reduced or lost Localisation ctn’d Level of motor unit Key Clinical Features Neuromuscular junction Involve cranial, limb girdle, proximal muscles +/- respiratory muscles Normal sensation (If presynaptic: +ve autonomic signs and post-exercise increase in strength If post-synaptic: fatigability) Muscle Predilection for neck, limb girdle, proximal muscles Normal sensation Possible cardiomyopathy Occasional resp muscle involvement Possible risk of myoglobinuria Regroup • • • • • • • Is respiratory failure imminent? Should ICU be involved? Where can I localise motor findings? Does it fit with sensory findings? Does it fit with autonomic findings? Does it fit with the history? Can the history help me narrow things down? Major Disorders Level of motor unit Disorders causing rapidly progressing weakness Motor neuron ALS Poliomyelitis Peripheral nerve Guillain-Barre syndrome Tick paralysis Diphtheric, porphyric, arsenic neuropathy Shellfish poisoning Neuromuscular junction Myasthenia gravis Botulism Lambert-Eaten myasthenic syndrome Hypermagnesemia Muscle Acquired: Dermato- and polymyositis, Myoglobinuric myopathy, Hypokalemic paralysis, Toxic myopathy, Acute myopathy of intensive care Genetic disorders: X-linked dystrophies, myotonic dystrophy, acid maltase deficiency, mitochondrial Laboratory Studies • CBC • Anemia or leukocytosis - systemic disease • Eosinophilia - possibly elevated in vasculitic neuropathy, porphyria • • • • • • Lytes, Cr, BUN, Ca, Mg, PO4, Liver enzymes (consider EtOH myotoxicity) CK (myopathy if very elevated) ESR (infectious or inflammatory disorders) CXR (pneumonia, atelectasis, elevated hemidiaphragm) EKG – Changes associated with electrolyte imbalances – Arrythmias 2ary to dysautonomia in GBS – Axis deviation – may be suggestive of cardiomyopathy Assess Respiratory Status • Tests in ER – MIP – MEP – FVC – ABG • 20/30/40 rule – VC: 20 ml/kg – MIP: -30cmH20 – MEP: +40cm H20 MYASTHENIC CRISIS Myasthenia Gravis • Disorder of transmission across NM junction • Auto-immune and congenital form • Epidemiology (auto-immune form): – 200-400 cases per million population – Women > men (3:2) – Bimodal incidence • F: 20s, 30s; M: 50s, 60s – 5-10% co-association with other auto-immune disorders Classification • Auto-immune – two forms – Acquired anti-AChR Abs (85%) – Acquired anti-MuSK Abs, a muscle-specific TK • 40-50% of anti-AChR seronegative pts • Congenital – Heterogeneous group (pre or post-synaptic) – Of note: do not affect respiratory muscles therefore do not present with myasthenic crisis Clinical Features • Painless, fatigable weakness of voluntary muscles – Repeated activity progressive paresis – Rest restoration of strength (at least partial) • Usually insidious onset – May occur more rapidly after precipitant (stress, infection) • Association with thymic abnormalities – 10-15% thymoma – 50-70% thymic lymphoid hyperplasia Clinical Features • Presenting symptoms: Diplopia Ptosis Generalised weakness Leg weakness 50-64% 50-64% 35% 10% Fatigue Respiratory failure 9% 1% • MuSK-MG – Younger women – Predominantly facial, bulbar and respiratory weakness – Relatively mild limb weakness Severity Classification Myasthenic Crisis • Myasthenic weakness leading to respiratory failure and need for ventilatory assistance • Severe weakness of respiratory muscles and/or • Severe weakness of upper airway muscles (bulbar myasthenia) Prevalence and Characteristics • Life-time prevalence: 20-30% – Early onset younger pt, median onset w/in 8 mos, fast recovery – Late onset older pts, later in dz course, slower recovery • White pts respond more poorly than black pts • Pregnancy aggravates MG in 30% of women – High potential mortality of crisis Precipitants • Elements to look for in history/chart: – Poor control of generalised disease – Medical treatment for bulbar myasthenia • Steroids and anti-cholinesterases – – – – – Use of certain drugs (next slide) Systemic infection, esp. of respiratory tract Aspiration Surgery Others (in refractory myasthenia): • Emotional stress • Hot environment • Hyperthyroidism Drugs • Anticholinesterases can also lead to myasthenic crisis • Signs of excessive cholinergic activity – Miosis, diarrhea, salivation, abdominal cramps, sweating, weakness Investigations • CBC, extended lytes, BUN, Cr, liver enzymes • CXR, U/A +/- blood cultures • Obtain VC, MIP, MEP – 20/30/40 rule Investigations • Repetitive motor nerve stimulation – Stimulate motor nerve at 2-3 Hz and measure CMAP of stimulated muscle – Positive if >er 10% decrement in amplitude of CMAP from the 1st to the 5th potential – Positive in about 75% of patients with generalized MG, if – Proximal & clinically involved muscles are tested – Muscle is warm – More than one muscle is tested • Single fibre EMG • Tensilon test not recommended in pt suspected of being in crisis – False postive, false negative – Risk of worsening muscle weakness in pts with anticholinesterase overdose – Worsening of bulbar and respiratory symptoms in MuSK-MG Management • Monitoring of respiratory status – Recognition of impending resp failure • Tachypnea, inability to count to 20, saliva pooling, nasal voice, NF weakness, paradoxical breathing – Deciding when to intubate • • • • (Code status) 20/30/40 rule If in doubt, intubate ?BiPAP – Limited experience. May reduce prolonged intubatn and trach Management • General – Stop any meds that may be contributing – Treat any infection • Specific – PLEX and IVIG comparable efficacy • Based on clinical evidence, few RTCs • Earlier response seen with PLEX – More likely to extubate at 14 days, better 1-month functional outcome (Qureshi, et al. Neurology, 1999). Management • PLEX – Removal of anti AChR and antiMuSK Abs – 1 session/day x 5 • No superiority of PLEX qd x 5 vs qod x 5 – Rapid onset of action (3-10 days) – Need central line with associated complications • PTX, hemorrhage, line sepsis – Caution in pts with sepsis, hypotension; may lead to increased bleeding and cardiac arrhythmias Management • IVIG – 0.4gm/kg/day x 5 days – Easily administered and widely available – Long duration of action • May last as long as 30 days – Side effects • • • • Anaphylaxis in IgA deficiency Renal failure, pulmonary edema Aseptic meningitis Thrombotic complications and stroke MG – Overall Treatment Summary • 1. Mild weakness: cholinesterase inhibitors • 2. Moderate-marked localized or generalized weakness – Cholinesterase inhibitors, and – Thymectomy for patients under age 50-60 yrs • 3. Symptoms uncontrolled on cholinesterase inhibitors – Prednisone if severe or urgent – Azathioprine • Prednisone failure • Excessive prednisone side-effects • 4. Plasma exchange or IV Ig – Impending crisis; crisis – Pre-operative boost – Chronic disease refractory to drug therapy • 5. If above fails – Search for residual thymus tissue – Cyclosporine or mycophenylate mofetil (Sem. Neurol., 2001;21:425-440) Guillain-Barre Syndrome GBS • Most common cause of acute and subacute generalised paralysis • Incidence of 0.4 to 1.7/100 000 per yr • Worldwide, all ages, both sexes • Preceding mild resp or GI infection in 60% (1-3 wks) – Campylobacter jejuni (26%), – CMV, EBV, VZV – Influenza, cocksackie, hepatitis A and B, HIV • May also be preceded by: – Surgery – Immunisations Typical Symptoms & Signs • Sensory – Paresthesias and slight numbness distally earliest Sx – Reduced proprioception and vibration sense (1 wk) • Motor – Weakness • Evolves symmetrically over days to 1-2 weeks • Usually LE before UE, proximal + distal • +/- trunk, intercostal, neck, cranial muscles – Progresses to total motor paralysis and respiratory failure in 5% of cases Typical Symptoms & Signs • Reflexes – Reduced and then absent • Autonomic dysregulation – Sinus tachycardia/bradycardia, facial flushing, labile BP, excess or loss of sweating, urinary retention – Usually do not persist for >er 1 wk • Other – Myalgias (50%) in hips, thighs, back Variants • Fisher syndrome – Ophthalmoplegia, ataxia, areflexia – +/- bilateral facial nerve paresis – Associated with anti-GQ1b Ab • Acute motor sensory axonal neuropathy (5% of GBS cases) – – – – Severe and diffuse axonal damage Abrupt and explosive onset Severe paralysis, minor sensory features Slow and poor recovery • Pandysautonomia – Severe orthostatic hypotension, anhidrosis, dry eyes and mouth, fixed pupils, arrhythmia, bowel/bladder dysfunction – Areflexia without somatic motor/sensory involvement • Other variants: – Initial cervico-brachial-pharyngeal muscle involvement – Generalised ataxia without dysarthria or nystagmus – Facial and abducens weakness, distal paresthesias, proximal leg weakness Laboratory Findings • Most important: CSF, EMG • CSF – Normal pressure – Protein • Early (1st 2 days): Usually normal (>85%) • Later: High (66% in 1st week, 82% in 2nd week) • Amount not correlated with clinical course or prognosis – Acellular or few lymphocytes • 10% : 10-50 lymphocytes, decreases over 2-3 days; if not: other Dx – Oligoclonal bands (10-30%) Laboratory Findings • EMG – Abnormalities seen within first week of sx – Reduction in motor amplitude – Slowed conduction velocities – Conduction block in motor nerves – Prolonged distal latencies (distal conduction block) – Prolonged/absent F-responses (involvement of proximal parts of nerves and roots) Laboratory Findings • Hematology – Abnormal only with infection or other disorder • Biochemistry – Mild-severe SIADH in 7-26% • Liver enzymes – Elevated <10% reflecting CMV or EBV infection • ESR: Normal unless co-existing process Diagnostic Criteria • • National Institute of Neurological Disorders and Stroke (NINDS) criteria are based on expert consensus. Required features include: – Progressive weakness of more than one limb, ranging from minimal weakness of the legs to total paralysis of all four limbs, the trunk, bulbar and facial muscles, and external ophthalmoplegia – Areflexia. While universal areflexia is typical, distal areflexia with hyporeflexia at the knees and biceps will suffice if other features are consistent. • Supportive features include: – – – – – – – – – Progression of symptoms over days to four weeks Relative symmetry Mild sensory symptoms or signs Cranial nerve involvement, especially bilateral facial nerve weakness Recovery starting two to four weeks after progression halts Autonomic dysfunction No fever at the onset Elevated protein in CSF with a cell count <10 mm3 Electrodiagnostic abnormalities consistent with GBS Differential Diagnosis • Features suggesting another diagnosis: – Sensory level, severe bladder or bowel dysfunction Spinal cord syndrome – Marked asymmetry Mononeuritis multiplex/vasculitis – CSF pleocytosis Infectious disorders: viral, HIV, lyme, poliomyelitis – Very slow nerve conduction velocities, multiple relapses or chronic course -> CIDP – Persistent abdominal pain and psychiatric signs Acute intermittent porphyria Management • General: – Recommend admission for observation • Can deteriorate rapidly in first days of presentation • M&M: Respiratory failure, dysautonomia • 25% will require mechanical ventilation • Respiratory – Measure MIP/MEP/FVC • Decision to intubate should be based on downward trend – Other measures of respiratory status same • Counting to 20, strength of NF Management • Dysautonomia – 10% develop hypotension • Volume, +/- pressors – Hypertension • IV labetolol • Other complications – Adynamic ileus – PE – Aspiration Management • PLEX and IVIG – No difference in efficacy between the two – Indications for prompt initiation • • • • • Respiratory failure Bulbar involvement Inability to walk without assistance Usually see these signs day 5-10 May occur anywhere from day 1 – week 3 • Steroids – No proven benefit PLEX • Regimen: 4-6 treatments on alternate days • Established usefulness in evolving phase • If treated within 2 wks onset – Decrease in LOS, ventilation, time to independent ambulation by approx. half • Value less clear if started later than 2 wks after initial symptoms • Predictors of response – Age – Preservation of motor CMAP amplitudes pre-PLEX IVIG • Dose: 0.4 gm/kg/day x 5 consecutive days • Cheaper, easier to administer • Rare complications – Renal failure, proteinuria, pulmonary edema – Asceptic meningitis – Anaphylaxis in IgA deficiency Course and Prognosis • • • • • Progressive symptoms : 1-4 weeks Plateau: 2-4 weeks Recovery: A few weeks to months Recurrence: 5-10% Mortality – 3-5% – Cardiac arrest, ARDS, PTX, HemoTX, PE • Pronounced disability: 10% – Clinical prognostic indicators • Greater age • Rapid evolution; early and prolonged ventilatory assistance, rapid course • Lack of treatment with IVIG or plasma exchange – Laboratory • EMG: severely reduced CMAP and widespread denervation Pathogenesis • Most evidence points to cell-mediated immunologic reaction directed at peripheral nerve – May be precipitated by antecedent infection • Antibodies against myelin components with complement-mediated damage • T cells and macrophages become involved in process and lead to destruction of myelin/axon THANK YOU