Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Aging brain wikipedia , lookup
Neuroanatomy wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Proprioception wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
National Institute of Neurological Disorders and Stroke wikipedia , lookup
Externalizing disorders wikipedia , lookup
Abnormal psychology wikipedia , lookup
Neurogenomics wikipedia , lookup
C HAP T E R 19 •
Disorders of the Cerebellum and Its Connections Christopher M. Fredericks, PhD
•
•
•
•
Signs and Symptoms oj Cerebellar Damage
Extracerebellar Causes oj Cerebellar Signs and Symptoms
Localization oj Cerebellar DysJunction
Specific Etiologies
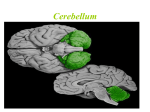
The cerebellum, which lies just dorsal to the pons and medulla, consists of two highly
convoluted lateral cerebellar hemispheres and a narrow medial portion, the vermis. It is
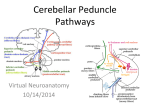
connected to the brain by three pairs of dense fiber bundles called the peduncles. Although
the structure and function of the cerebellum have long been studied, the precise role of the
cerebellum in motor control remains to be fully elucidated.
As discussed in Chapter 8, it is clear that the cerebellum receives a tremendous number
of inputs from the spinal cord and from many regions of both the cortical and subcortical
brain. In this way, the cerebellum receives extensive information from somesthetic, vestibu
lar, visual, and auditory sensory systems, as well as from motor and nonmotor areas of the
cerebral cortex. Although afferent connections outnumber efferent projections by about 40
to 1, the cerebellum has extensive outgoing connections to many areas of the brainstem,
midbrain, and cerebral cortex.
It is evident that while the cerebellum does not serve to initiate most movement, it does
interact with areas of the brain that do. 1 - 3 In doing so, the cerebellum promotes the
synchrony and accuracy of movement required for purposeful motor activity. The cerebellar
mOQlJ,lalion and coordination of muscular activity are important in skilled voluntary
movement, as well as in the movements of posture and equilibrium.
The cerebellum is vulnerable to most of the nonspecific disease processes that affect
other areas of the central nervous system, as well as to certain diseases unique to the
cerebellum (Table 19-1). When the cerebellum or its direct connections are damaged, a
characteristic constellation of symptoms and clinical signs arises. At ·first glance, the motor
deficits produced by such damage are less than one might expect of a structure so centrally
located in the neuraxis and so intimately involved in motor control. Extensive damage to the
cerebellum, for example, does not abolish movement and rarely even causes muscle
weakness. Somesthetic or other sensibilities are not disrupted, nor is cognition. Instead, the
most prominent effects of cerebellar destruction are a type of incoordination or clumsiness
445
Disorders of Central Motor Control
446
Table 19-1. Cerebellar Disorders Organized by Etiology
•
•
•
•
•
•
•
•
•
•
Inherited or idiopathic degenerations
Nutritional disorders
Neoplastic and paraneoplastic disorders
Developmental disorders
Disorders due to infection
Vascular disorders
Intoxications
Physical or mechanical trauma
Metabolic disorders
Demyelinating or dysmyelinating disorders
of movement called ataxia and abnormal muscle tone. Although cerebellar lesions may
delay the initiation of movements and alter their form, they do not prevent their execution.
This is very different from the motor deficits that result from damage to the motor cortex or
to the systems descending from it, in which the strength and speed of contraction are
impaired and the ability to contract individual muscles may be lost altogether. If you recall
that the role of the cerebellum is not to initiate motor activity but to modulate and refine
motor behaviors initiated elsewhere, then the signs and symptoms of cerebellar damage are
not surprising.
Destruction of small portions of the cerebellar cortex rarely causes detectable abnor
malities in motor function. To cause serious and continuing dysfunction, the cerebellar
lesion must be extensive and usually involves one or more of the deep cerebellar nuclei in
addition to the cerebellar cortex. It is interesting that the neurologic signs produced even by
extensive damage tend to gradually diminish with time, assuming that the underlying
disease process does not itself progress. Such improvement is particularly evident following
childhood damage. In experimental animals, even after as much as 50% of the cerebellar
cortex has been removed, if the deep nuclei are left intact, motor function appears normal as
long as the movements are performed slowly.
Signs and Symptoms of Cerebellar Damage
Although the specific neurologic signs associated with cerebellar disease and injury
are numerous,2,4,5 the basic functional deficits producing these signs are relatively few (Table
19-2). Moreover, these basic functional deficits are a logical consequence of the disruption
of the motor functions known to be carried out by the cerebellum.
Incoordination of Movement l ,2,4,5
The cerebellum is responsible for the smoothly integrated coordination of movements.
It is needed for movements that require the concerted, synergistic contraction of multiple
muscle groups, and it permits such movements to be carried out efficiently and accurately.
The most conspicuous and most common result of cerebellar dysfunction is an
incoordination or clumsiness of movement. This incoordination is referred to by clinicians
as ataxia, a term derived from the Greek word meaning "lack of order." Patients with ataxia
have difficulty regulating the force, range, direction, velOcity, and rhythm of muscle
contractions and in maintaining the synergy that normally exists among the various muscles
involved in motor activities. Ataxia is a general term and may be manifested in any number
of specific clinical signs, depending on the extent and locus of involvement. Limb
movements, gait, speech, and eye movements all may be affected.
Disorders of the Cerebellum and Its Connnections
447
Table 19-2. Basic Characteristics of Cerebellar Signs and Symptoms
• Lesions of the cerebellum produce errors in the planning and execution of movements, rather than
paralysis or involuntary movements.
• In general, if symptoms predominate in the trunk and legs, the lesion is near the midline; if symptoms
are more obvious in the arms, the lesion is in the lateral hemispheres.
• If only one side of the cerebellum is affected, the symptoms are unilateral and ipsilateral to the lesion.
• The most severe disturbances are produced by lesions in the superior cerebellar peduncle and the
deep nuclei.
• Many of the symptoms of cerebellar disease improve gradually with time if the underlying disease
process does not itself progress.
• Almost all patients with cerebellar lesions have some type of gait disturbance.
• Speech disturbances occur only with bilateral damage.
• Signs and symptoms similar to those produced by cerebellar lesions can appear with disorders that
affect structures adjacent to the cerebellum or affect the afferent or efferent connections of the
cerebellum.
If the legs and trunk are affected, difficulty in maintaining posture and coordinating
leg movements will result in ataxia of gait. Such patients are unsteady during ambulation
and attempt to improve their stability by walking with a broad-based gait and lower center
of gravity. Their steps are uncertain and irregular, and they may stagger or veer from side to
side. Patients with gait ataxia also have a decrease in the normal, free-flowing arm swing that
normally accompanies ambulation. Walking heel-to-toe or running the heel of one foot
down the shin of the other leg while seated or lying down is difficult and serves as tests for
this deficit. Problems with standing or walking are present in almost all patients with
cerebellar damage, regardless of the site of the damage, and, when severe, may cause
considerable disability.
Ataxia of the arms (limb ataxia) creates its own specific clinical signs. Difficulty in
bringing a limb smoothly and accurately to a specific target in space is called dysmetria. An
involved limb may either overshoot (hypermetria) or undershoot (hypometria) its target.
Complex movements, because of errors in the timing and sequencing of their component
parts, may deteriorate into a series of successive simple movements, rather than one smooth, coordinated movement. This is termed decomposition of movement and is most evident in
movements involVing multiple joints. At the end of such movements, when the patient is
attempting to achieve the greatest precision, a coarse tremor may develop called an intention
tremor. These tremors do not occur at rest nor during postural fixation, but develop while
precise, intentional movements are undertaken. Intention tremors probably reflect impaired
coordina.tion of agonists and antagoniSts, as well as an attempt to correct for overshoot and undershoot.
Dysmetria, decomposition, and tremor all can be demonstrated by simply asking the
patient to point from one stationary target to another, such as in bringing the tip of the finger
of the extended upper extremity to the nose (Fig. 19-1). As the movement is undertaken,
each joint of the shoulder, elbow, wrist, and finger may flex independently ina puppetlike
fashion and large errors in the direction and rahgeof mbvementoccur as the target is
approached. As the finger nears the nose, the hand and finger exhibit a tremor. Limb ataxia
may also be manifested as an impairment of the ability to perform rapidly alternating
movements, such as rapid supination and pronation of the forearm. This is termed
dysdiadochokinesia.
Persistent incoordination of axial muscles may lead to reversible abnormalities of
stance and posture, such as head or body tilt,or to more permanent skeletal abnormali
ties, such as scoliosis. Truncal ataxia may result in swaying of the trunk, staggering gait, and
difficulty in sitting unsupported.
Bulbar muscles may also be affected, leading to slurred speech (dysarthria) and
numerous disturbances of oculomotor activity, including nystagmus.
.j
i
,
~
~
I
I
i!
~,
I
I
,
~
J
I
448
Disorders of Central Motor Control
8
A
•
Go
~
I
~_Normal
/
-------(1
I
Normal
I
i
~-
--------------~I----~
Abnormal
I
I
10lil
I
"I
Finish
Delay
c
Normal
Abnormal
Figure 19-1. Typical Defects in Cerebellar Diseases. (A) A lesion in the right cerebellar hemisphere causes a delay
in the initiation of movement. The patient is told to flex both arms at the same time on a "go" signal. The left arm
is flexed later than the right, as evident in the recordings of elbow position. (8) A patient moving his arm from a
raised position to touch the tip of his nose exhibits dysmetria (inaccuracy in range and direction) and unsmooth
movement with increased tremor on approaching the nose. (C) Dysdiadochokinesia. an irregular pattern of
alternating movements, can be seen in the abnormal position trace. (From Ghez, l p 643, with permission.)
Hypotonia 1 ,2,4-7
Muscle tone refers to the ease with which a muscle may be lengthened by passive
stretch. The normal cerebellum contributes to the maintenance of muscle tone through
facilitatory influences on skeletal muscle stretch reflexes. 7 Cerebellar output increases
gamma input to muscle spindles, making them more sensitive to stretch and thus increasing
overall muscle tone. Without this input, tone diminishes.
Hypotonia refers to a decreased resistance to passive stretch as might occur with passive
limb movement. Although not as common as ataxia, hypotonia may result from cerebellar
damage and lead to a number of distinct clinical signs. Hypotonia is most evident shortly
after acute cerebellar injury and tends to decrease with time. In early and severe cases, a
distinct flabbiness of muscle can be palpated and the muscle accommodates greater stretch
without discomfort. Decreased muscle tone may result in a pendular limb, with pendular
deep tendon reflexes. For example, when the petallar reflex is elicited, the leg will continue
to swing back and forth in a pendular fashion. Hypotonia is often associated with an inability
to stop a rapidly moving limb (Le., lack of check), resulting in an overshoot, followed by
excessive rebound in the opposite direction. If such a patient is asked to pull upward
strongly with his or her arm while the clinician first holds it back and then releases it, the
arm will fly back, unchecked, until it strikes the face instead of being automatically stopped.
Although hypotonia is not as conspicuous as ataxia, it can exacerbate the symptoms
produced by ataxia. Decreased tone in postural muscles, for example, contributes to gait
disturbances and postural asymmetry. Hypotonia in the muscles of speech promotes abnor
malities in pitch and loudness, and in oculomotor muscles results in difficulty in maintaining
the gaze.
Disorders of the Cerebellum and Its Connnections 449
Dysequilibrium and Vertigo 1 ,2,4,5
The most primitive parts of the cerebellum (the floccolonodular lobes) have extensive
connections with both the vestibular nuclei and the vestibular apparatus. It is likely that
even in the human, the cerebellum plays a significant role in the maintenance of equilibrium
and the coordination of head and eye movements.
Lesions in these regions result in disturbances of equilibrium that are particularly
evident during rapid changes in body position or in the direction of movement. Patients
may exhibit unsteadiness of gait or an inability to sit or stand without swaying or falling,
as well as abnormalities of head posture and eye movement (nystagmus). These deficits are
specifically related to an inability to carry out motor activities against the force of gravity.
The principal defect is in equilibrium, not ataxia or abnormal muscle tone. Moreover,
cerebellar infarction and hemorrhage (stroke) have been shown to induce signs and
symptoms such as vertigo, nausea, vomiting, and nystagmus, which mimic damage done to
the vestibular labyrinth itself.
Delays in the Initiation and Termination of Movement 1 ,2,4,5
Lateral portions of the cerebellar hemispheres and the associated dentate nuclei play
important roles in the planning and programming of movement. This is particularly so in
multijoint movements and in those requiring fine dexterity in the distal extremities. Lesions
on either side of the dentate nuclei or the overlying cortex can interfere with this
programming, resulting in delays in both the initiation and the termination of movement.
Intentional movements, such as grasping or pointing, may be slowed in both the buildup
and the relaxation of force. Consequently, the movement of an affected limb is delayed and
slowed.
Nonmotor Deficits
Although the principal physiologic importance of the cerebellum resides in its
contributions to somatic motor control, evidence is accumulating that the cerebellum is also
involved in a variety of nonmotor functions (see Chapter 8).
If this involvement is functionally significant, one would expect evidence of this
involvement to appear among the sequelae of cerebellar damage. In fact, nonmotor deficits
are now beginning to be discussed in the context of human cerebellar disease. Studies
conducted in both animals and humans provide evidence that the cerebellum plays a role in
motor learning. 8 •9 Experimental cerebellar lesions in animals and pathologic lesions in
humans seem to interfere with these learning processes. 10-12 Evidence is also accumulating
through the use of active imaging techniques that the cerebellum is engaged in such mental
functions as shape and word recognition. 13 ,14 Although an association between some
developmental disorders of the cerebellum and retarded intellectual development has been
reported for some time,15 cognitive abnormalitiesare~ri()t~usuallyapparent in patients with
cerebellar disease. Recently, subtle defects in verbaland nonverbal intelligence, in memory,
and in other "higher functions" in cerebellar patients have been reported. 16 - 18 Although
anatomic connections exist between the cerebellum and the areas of the brain involved in
the expression of emotion and although animal experiments suggest involvement of the
cerebellum in various emotion-laden behaviors such as rage, fear, and aggression, little is
known of the role the cerebellum may play in mediating or influencing emotions in hu
mans. In this regard, specific structural abnormalities in the cerebellum of patients with
21 and certain psychological disorders have been revealed by computed tomog
.~ autism 19 raphy (CT) and magnetic resonance imaging (MRI) scans, as well as by pathologic
study. 22-24 As clinical skills and neuroimaging techniques are refined and more attention is
focused on nonmotor deficits, these deficits will undoubtedly be found within the constel
lation of findings associated with cerebellar dysfunction.
Disorders of Central Motor Control
450
Extracerebellar Causes of Cerebellar
Signs and Symptoms
Many of the signs and symptoms associated with cerebellar damage can also be
caused by lesions outside the cerebellum itself. Ataxia, for example, can be caused or
exacerbated by a variety of extracerebellar lesions. Conditions that disrupt the spinocerebel
lar tracts can cause dysmetria and ataxia by depriving the cerebellum of proprioceptive
input. These kinds of defects underlie Friedreich's ataxia (discussed later in this chapter) and
many of the cerebellar findings of multiplesderosis (see Chapter 22). By the same token,
disruption of somatosensory nerves in the peripheral nervous system can impair the
proprioceptive sense enough to cause a sensory ataxia, such as might be observed in
alcoholic or other types of peripheral neuropathy (see Chapter 15). Disorders of the
vestibular system, by interfering with balance and equilibrium, can mimic and exacerbate
the gait problems associated with cerebellar damage.
Localization of Cerebellar Dysfunction
As discussed in Chapter 8, attempts have been made to functionally compartmentalize
the cerebellum into three basic regions, using either phylogenetic or neuroanatomic criteria
(Fig. 19_2).1,2,25 Although not totally congruent, the archicerebellum, paleocerebellum, and
neocerebellum of the phylogenetic scheme correspond fairly well to the vestibulocerebellum,
spinocerebellum, and cerebrocerebellum, which are defined by their primary afferent and
efferent connections. Attempts have been made over the years to organize the various signs
and symptoms that arise from cerebellar disease into distinct syndromes, which reflect the
region of the cerebellum that is damaged. 4 ,5,25,26 Accordingly, three syndromes have been
described, which some consider to be useful models for localizing cerebellar dysfunction.
Vestibulocerebellar, Archicerebellar, or Flocculonodular Lobe Syndrome The flocculonodular lobe is phylogenetic ally the oldest division of the cerebellum and
receives extensive input from the vestibular system. This is why this portion of the
cerebellum is often termed the archicerebellum or vestibulocerebellum. The vestibulocer-
Intermediate
Hemisphere
- - I Spinocerebellum
lateral
Hemisphere} CerebrocerebeUum
Dentate Nucleus - t - - - - - t -
F1occuIUS-}Vestibulocerebellum
I"U'JUI~I;:O
Figun~
19-2.
Major divisions of the cerebellum.
Disorders of the Cerebellum and Its Connnections
451
ebellum receives mossy fiber input chiefly from the vestibular nerve and nuclei and projects
back to the vestibular nuclei, which in tum project to the spinal cord (vestibulospinal tracts)
and the oculomotor nuclei. This system is important for equilibrium and for control of the
axial muscles that are used to maintain balance in the face of gravity. The vestibulocerebel
lum also controls eye movement and coordinates movements of the head and eyes. Because
of the close relationship between the vestibulocerebellum and the vestibular system, damage
to this region of the cerebellum causes clinical findings that mimic vestibular disease
itself. Such disorders cause disturbances of locomotion and equilibrium, with prominent
truncal and gait ataxia. Patients with isolated flocculonodular lesions lose their ability to
stand or walk without swaying or falling and tend to fall even when sitting with their eyes
open. It is interesting that when the effects of gravity are reduced by the patient lying in bed
or being physically supported, movements may be completely normal. Abnormalities of
posture and station (e.g., head tilt) and of eye movements also occur. Tremor is not evident
and muscle tone remains normal.
The most common lesion involving the vestibulocerebellum is a special type of tumor,
a medulloblastoma, which usually occurs in children.
Spinocerebellar or Paleocerebellar Syndrome
Most of the vermal and paravermal(intermediate) regions of the cerebellum receive
extensive somatosensory input from the spinal cord and are thus called the spinocerebel
lum. The spinocerebellum also receives input from the auditory, visual, and vestibular
systems. The vermal and intermediate portions of the spinocerebellum project to different
deep nuclei, controlling different components of the descending motor pathways. The
vermis projects to the fastigial nucleus and from there influences cortical and brainstem
components of the medial descending systems (axial and girdle muscles). The intermediate
part of the cerebellar hemispheres projects to the interposed nucleus to control the lateral
descending systems (distal muscles of extremities). The spinocerebellum receives a
continuous flow of somatosensory information regarding the status of the musculoskeletal
system, as well as concurrent information from cortical areas about motor commands. It
uses this feedback to monitor and refine the execution of movement and to control muscle
tone.
Discrete lesions limited to the spinocerebellum. such as those described in experimental
animals, seldom occur in humans. Damage to the human spinocerebellum is most
commonly seen in the context of a late degeneration and atrophy of the anterior lobes
associated with chronic alcoholism and thiamine deficiency. The cardinal feature of
spinocerebellar disease is involvement of the legs, resulting in abnormal gait and stance.
The gait is wide-based and ataxic, with small hesitant steps. The gait ataxia of spinocerebel
lar damage is different from that arising from vestibulocerebellar (flocculonodular) damage.
Spinocerebellar ataxia reflects a more general deficit in the control of the muscles of
ambulation, whereas vestibulocerebellar ataxia reflects a particular inability to control the
leg muscles in the presence of the force of gravity. In the case of spinocerebellar daIl1age, the
ataxia is not relieved when the .patienLis. freed fromihe effects ofgraVity by being physically
supported or lying in bed, as it would be with vestibulocerebellar damage.
Cerebrocerebellar,Neocerebellar, or Lateral Cerebellar Syndrome The cerebrocerebellum, which occupies the lateral zone of the cerebellar hemi
spheres, is phylogenetically late in developing and is particularly well developed in
primates. This region receives most of its input from sensory, motor, and premotor areas of
the cerebral cortex that project to the cerebrocerebellum via the pontine nuclei. Most of the
output of this area is to the dentate nucleus, which in tum projects back to the cerebral
cortex. Through its extensive connections with the cerebral cortex, the cerebrocerebellum
452
Disorders of Central Motor Control
is thought to function in the planning and initiation of voluntary movements. It is
necessary for achieving precision in rapid limb movements, especially those involving fine
dexterity of the distal extremities and movement at multiple joints. Damage to the lateral
hemispheres and dentate nuclei disturbs skilled coordinated movements and speech.
Errors in direction, deviation from proper course, dysmetria, dysdiadochokinesia, and
intention tremor all may be present, especially in movements of the upper extremities. The
gait may actually be normal, reflecting the relative sparing of the axial muscles and lower
limbs. Intentional movements, such as grasping or pointing, may be delayed in their
initiation and slowed in both the buildup and the relaxation of intended force. Stretch
reflexes and muscle tone are often diminished, resulting in flabbiness, lack of check, and
pendular deep tendon reflexes. Muscle weakness and fatigability, although not that common
in cerebellar disorders, are most prominent in cerebrocerebellar syndrome. Dysarthric
speech may occur with bilateral involvement and can be pronounced. Oculomotor signs may
also occur.
When the damage is unilateral, the ipsilateral limb is affected. With limited damage,
it is sometimes possible to show impairment only of highly trained movements, such as
playing a musical instrument, whereas all other movements appear normaL
Problems with Localization of Dysfunction
Although the divisions of the cerebellum that are based on phylogenetic.. criteria and
comparative anatomic studies (e.g., the archicerebellum, paleocerebellum, and neocerebel
lum) correspond reasonably well to the divisions of the cerebellum defined by the locus of
the termination of the major afferent projections (e.g., the vestibulocerebellum, spinocer
ebellum, and cerebrocerebellum, respectively). This congruence is not total. Considerable
overlap exists between the regions defined by the anatomic sites of afferent terminations.
Moreover, the phYSiologic effects of activating afferent sources project far beyond the
boundaries ascribed to these regions. Accordingly, some authors feel that it is misleading to
define the clinical scenarios arising from cerebellar damage in terms of these phylogenetic or
neuroanatomic regions.
In addition, it should be recognized that many symptoms of cerebellar dysfunction
simply defy limitation to anyone division of the cerebellum. A good example of this is
disturbance of gait, which is the most common def cit seen in cerebellar disease. Gait may be
disturbed as a consequence of the impairml'1t of equilibrium encountered in disorders
involving the; flocculonodular lobes. Gait imp. <rment may also result from anterior lobe
disorders that adversely affect postural control. F. 1ally, posterior lobe lesions can disturb gait
through effects on muscle tone and volitional movement. Accordingly, gait disturbance is to
be expected with practically all cerebellar lesions and by itself does little to localize the site
of cerebellar damage. In addition, gait can be impaired by disorders of the spinal cord or
peripheral nerves that disrupt the flow of proprioceptive information to the cerebellum, as
well as by damage to the vestibular system. Lesions in certain cerebral and brainstem areas
may likewise interrupt the flow of information to or from the cerebellum, causing gait
disturbance similar to that seen in disease of the cerebellum itself.6
Specific Etiologies
Although cerebellar disorders as a whole are not very common, a wide variety of
factors, both inherited and acquired, can adversely affect cerebellar function (see Table
19-1). As with any region of the central nervous system, these conditions may be organized
or classified using a number of different criteria, such as prominent clinical features,
pathologic criteria, or etiologic factors. For the purposes of this discussion, the major
~.
Disorders of the Cerebellum and Its Connnections
453
cerebellar disorders are organized along the lines of what is known of their etiology or
pathogenesis. It should be noted that because of our incomplete understanding of the causes
of many of these disorders, this classification scheme is somewhat arbitrary. Moreover,
disorders may logically fall into more than one category.
Inherited or Idiopathic Degenerations5 ,27-33
For unknown reasons, certain regions of the nervous system are particularly vulnerable
to degenerative disease. Among these are the cerebellum and its connections. Many of these
disorders are genetic or of unknown etiology. These may be distinguished from other
degenerative conditions in which underlying toxic, metabolic, infectious, or neoplastic
conditions have been identified. These are discussed elsewhere in this chapter.
The genetic and idiopathic degenerations constitute a large group of chronic dis
orders in which progressive ataxia, disintegration of gait, and dysarthria are the most
prominent features~7 -33 This is a complex group of disorders, and numerous attempts have
been made to make order of their diversity. Classification schemes have been proposed,
based on various clinical, pathologic, biochemical, and genetic criteria. Unfortunately,
because of our limited understanding of etiologic factors, the variability of clinical features,
and the poor correlation between clinical presentations and pathologic findIngs, none of
these schemes is entirely satisfactory. It is often difficult to discern where one disorder ends
and another begins. A more reliable classification of these disorders ultimately depends on a
better understanding of the genetics of these disorders and the specific biochemical defects
to which they give rise.
Nonetheless, for our descriptive purposes these degenerative diseases may be arbitrarily
divided into large clinicopathologic groupings. The entire cerebellar system is vulnerable;
one way to organize these disorders is to divide them into those with a predilection for the
cerebellum itself and those with a predilection for the pathways to whiehit is connec;ted.
With respect to the latter, both peripheral and spinal neurons may be affected. Disorders that
primarily involve the peripheral nerves, such as the hereditary sensory motor neuropathies;
are discussed in Chapter 15; those with prominent involvement of the spinocerebellar tracts
are discussed below. In either case, disruption of the flow of somatosensory (proprioceptive)
information to the cerebellum can result in an incoordination of movement. These anatomic
distinctions are somewhat arbitrary and although involvement of one particular part of the
cerebellar system may be predominant, other regions may also be involved, particularly with
disease progression.
Spinal Ataxias
In spinal ataxias the pathology involves primarily the spinocerebellar tracts, whereas
the cerebellum itself and the brainstem are relatively spared. Associated degenerative
changes in the peripheral nervous system mayor may not be evident.
~.
Friedreich's ataxia is one of the most common hereditary disorders of the nervous
system. It is also the most common of the early-onset hereditary spinal ataxias, accounting
for at least 50% of these disorders. The symptoms begin to develop in children between 8
and 15 years of age, with clumsiness of gait being the most common presenting symptom. As
the condition develops, it is characterized by relentlessly progressive ataxia, with increas
ing weakness, loss of tendon reflexes, and impaired proprioceptive sensation in the lower
limbs. The ability to walk is usually lost within 15 years of onset. Ataxia, which begins in the
lower limbs, later becomes evident in the arms and then the trunk. Scoliosis is frequent and
may be severe, particularly if the onset is early (Fig. 19-3). This deformity contributes to
454
Disorders of Central Motor Control
Figure 19-3. Friedreichs Ataxia.
Note the foot deformity (pes cavus)
and kyphoscoliosis in these patients.
(From Dow, Kramer, and Robert
son,5 p 56, with permission.)
eventual cardiopulmonary problems. Foot deformities, especially pes cavus, are also
common. Ocular movements are almost always abnormal, and many patients develop a
cerebellar-type dysarthria. Cardiomyopathy with abnormal electrocardiogram (ECG) find
ings is present in most patients with Friedreich's ataxia, and death from heart failure often
occurs late in the disease.
Characteristic pathologic changes are observed in both the peripheral and central
nervous systems, particularly in the sensory systems?3 In the peripheral nervous system,
there is degeneration of sensory fibers, sensory ganglion cells, and posterior roots. In the
central nervous system, the most conspicuous lesions are in the spinal cord, the posterior
columns, and spinocerebellar tracts (Fig. 19_4).33 Although there may be some patchy loss
of cerebellar Purkinje cells and mild degenerative changes in cerebellar nuclei, the ataxia of
movement is largely a result of the loss of proprioceptive sense.
The condition most likely to be confused with Friedreich's ataxia is the peroneal
atrophy syndrome, in which distal wasting and weakness of the lower limbs (and to a lesser
degree the upper limbs) are associated with areflexia. 29 - 31 This clinical syndrome is
associated with type I hereditary sensory and motor neuropathy (see Chapter 15) and distal
spinal muscular atrophies (see Chapter 16). In sporadic cases without skeletal deformity,
distinguishing between Friedreichs ataxia and multiple sclerosis may also be difficult.
455
Disorders of the Cerebellum and Its Connnections
I
1
I
11
I
..~ ~/I\i:.:."
Figure 19-4. Characteristic Appearance of Lower Cervical Cord in Friedreich's Ataxia. In this transverse section
of the cervical spinal cord in which myelin is darkly stained, a loss of myelin is evident in the posterior columns
(Large *), spinocerebellar tracts (Small *), and the crossed (Lateral) and uncrossed (Anterior) corticospinal tracts
(Arrows). (From Oppenheimer, DR: Brain lesions in Friedreich's ataxia. Can J Neurol Sci 6:173, 1979, with
permission.)
Cerebellar Ataxias
In the cerebellar ataxias, the predominant pathologic changes occur in the cerebellum
and its immediate connections, rather than in the spinal cord tracts.
Olivopontocerebellar Atroph r,27 -33,35
~
In this category are a number of similar disorders characterized by a combined
degeneration of the cerebellum, pons, and inferior olives. In general, these disorders are
characterized by progressive ataxia with a later onset than Friedreich's ataxia (e.g., between
the third and fifth decades of life). The gait is affected first, with progressive ataxia of the
trunk and limbs, impairment of equilibrium, slowness of voluntary movement, and
abnormal speech. Although patients often have a pure cerebellar syndrome during the first
few years of their illness, pyramidal tract signs, autonomic disturbances, and parkinso
nian features with mild dementia may develop later in the illness. Autonomic disturbances
may present as urinary incontinence or orthostatic hypotension. Considerable clinical
variability exists among cases of olivopontocerebellar atrophy. Some patients present a
picture of relatively pure cerebellar ataxia indistinguishable from that seen in patients with
atrophy limited to the cerebellar cortex. Others may have more prominent parkinsonian
features and an early dementia.
Pathologic changes are widespread, giving rise to the diverse clinical findings associated
with this syndrome. Gross shrinkage of the pons and medulla may be evident, whereas
neuronal loss in the inferior olives, cerebellar cortex, and basal ganglia is revealed by
microscopic examination. Some degenerative changes may also be evident in the long motor
tracts of the spinal cord and the anterior horn cells?3
456
Disorders of Central Motor Control
Attempts have been made to define various subtypes of this degeneration, based on the
particulars of the mode of inheritance and the predominant clinical features; however, these
explorations are beyond the scope of this discussion.
Pure Cerebellar Degeneration27 -33
In some instances, a relative pure cerebellar syndrome arises, reflecting pathologic
changes restricted to just the cerebellum. Unlike Friedreich's ataxia and other spinocerebel
lar ataxias, there is little evidence of spinal cord involvement. Also, unlike olivopontocer
ebellar degenenl.tion, there is no prominent involvement of other regions. of the brain or
brainstem. Although pure cerebellar degeneration can occasionally occur sporadically, in
most cases it is evidently inh~rited as an· autosomal-dominant trait This disorder is less
common than Friedreich's ataxia. Its age of onset is later, usually oc~urring in the fourth
decade of life or beyond. The patient first develops gait ataxia (with abnormal stance and
instability of gait), progressing to dysarthria and finally to ataxia of the upper extremities and
trunk. This disorder is progressive, but may be so gradual that incapacitation does not occur
.
for decades and does not appreciably shorten the life span.
Pathologic changes include a marked loss of neurons (especially Purkinje cells) from
the cerebellar cortex, most prominent on the superior surface of the vermis and adjacent
parts of the cortex. In advanced cases, atrophy of the cerebellar cortex may be readily
apparent with CT scanning. The deep cerebellar nuclei are relatively normaL
Ataxia-Telangectasias ,27-33,36-38
Ataxia-telangectasia is the most common cerebellar ataxia of infancy and childhood.
This inherited disorder is unusual to the extent that the cerebellar deficits are
accoInpanied by characteristic vascular lesions (telangectasia) and recurrent pulmonary
infections. The first motor symptom is usually truncal ataxia, which is noted when the
child first begins to walk, resulting in an awkward, unsteady gait. When the child reaches
4 or 5 years of age, the limbs become ataxic and dysarthria may be evident. With
progression of the disease, extrapyramidal signs such as dystonia and choreoathetosis may
develop. Telangectasia is a vascular lesion formed by the dilatation of a small group of blood
vessels, which is often observed as a "birthmark." For reasons unknown, these lesions
develop in the skin or conjunctiva of the eye in this disorder.
PatholOgiC changes are noted in many regions of the nervous system, inclUding a severe
loss of Purkinje cells in the cerebellum, as well as atrophy of the posterior columns and
spinocerebellar tracts of the spinal cord?3,36-38 Degenerative changes may also be evident in
anterior horn cells, sensory and autonomic ganglia, and peripheral nerves.
Nutritional Disorders
Adequate nutrition is necessary for both the normal development and ongoing func
tioning of the entire nervous system. Nutritional disorders, particularly certain vitamin
defiCiencies, can adversely affect both the peripheral and central nervous systems, creating a
wide range of neurologic manifestations. 39,40 Depending on the deficiency, such findings may
include changes in mental status (e.g., coma, mental retardation, psychosis), seizures, cer
ebellar ataxias, and peripheral motor and sensory disturbances. The few conditions in which
cerebellar signs and symptoms are most prominent will be discussed in the following
text.5,29,30,39,40
Disorders of the Cerebellum and Its Connnections
457
Vitamin Bl (Thiamine) Dejid ency5,2.9.30.39-45
Of all the vitamin deficiencies, thiamine deficiency is probably the most common in
Western society and produces the most severe cerebellar deficits. This deficiency is most
often seen in association with chronic alcoholism, but may also be seen in patients with
abnonnal gastrointestinal activity.
Chronic alcoholics frequently develop a condition termed the Wernicke-Korsakoff
syndrome. 41 - 45 Wernicke's disease is characterized by oculomotor abnormalities, altered
mental status, and ataxia of stance and gait. This disease is often associated with Korsakoff's
psychosis, a cognitive disorder in which short-term memory is impaired out of proportion to
other intellectual functions.
Prominent cerebellar dysfunction occurs in about one third of all alcoholics, and is
prominent among those with Wernicke's disease. 41 •44 Stance and gait are primarily affected,
the legs being more affected than the trunk or arms. The ataxia may be so severe in the
acute stage of the disease that the patient cannot walk or stand without support. Less severe
degrees of the disease are characterized by a wide-based stance and slow, tentative steps.
Speech disturbances and abnormal eye movements are relatively infrequent. Pathologic
changes in the cerebellum consist of degeneration throughout the cortex, with a striking loss
of Purkinje cells. 4o This is most pronounced in the anterior superior aspects of the
cerebellum (Fig. 19-5). Signs of peripheral neuropathy are found in most patients with
Wernicke-Korsakoff syndrome, but in most cases involvement is mild and does not account
for the gait disturbance.
Despite the well-known acute affects of alcohol directly on the cerebellum, it is
generally thought that the chronic cerebellar syndrome observed in alcoholics is caused by
thiamine deficiency rather than toxicity of the alcohol itself. 29 •30 ,41 Alcoholics with this
Figur-e 19-5. Alcohol-Induced Cerebellar- Atrophy. In this midsaggital section, atrophy is apparent in the anterior
and superior aspects of the cerebellum and is most evident in the shrinkage of the vermal folds (Arrows). Inferior
structures appear grossly normal. (From Victor, M, Adams, RD, and Mancail, EL: A restricted form of cerebellar
cortical degeneration occurring in alcoholic patients. AMA Arch Neurol 1:579, 1959, with permission.)
458
Disorders of Central Motor Control
condition are almost always malnourished. That this is not due to alcohol toxicity itself is
further suggested by the facts that the ataxia may develop during periods of abstinence, that
the symptoms can be relieved by administration of thiamine alone, and that an identical
cerebellar degeneration may occur in other (nonalcoholic) states of poor nutrition.
A cerebellar cortical degeneration may also occur in malnourished alcoholics, which is
distinct from that associated with Wernicke-Korsakoff syndrome. Truncal instability is the
major symptom, often with· incoordination of leg movements. The symptoms of this
cerebellar degeneration may evolve over weeks or months and may eventually stabilize, even
with continued drinking and poor nutrition. In Wernicke's disease, on the other hand, the
symptoms are more likely to appear abruptly.
Alcoholics may also develop a sensorimotor polyneuropathy that stabilizes or improves
with abstinence and an adequate diet. Although this neuropathy is found in most patients
with Wernicke-Korsakoff syndrome, it more often occurs alone. As discussed in Chapter 15,
this polyneuropathy is characterized by degeneration of both axons and myelin.
Vitamin B12 (Cobalamin) Dejiciency5,39,40
Vitamin B12 deficiency, which is due to an inability to absorb this vitamin from the gut
rather than dietary deficiency; produces a condition called pernicious anemia. The spinal
cord, brain, optic nerves, and peripheral nerves all may be involved in pernicious anemia.
The spinal cord is affected first and most often and reveals a diffuse degeneration of the
white matter. Sensory disturbances, muscle weakness, and spastic ataxia are common.
Paresthesias and decreased vibratory and position sense reflect lesions in both spinal and
peripheral sensory pathways. Muscle weakness, spasticity; and abnormal tendon reflexes
result from lesions in corticospinal tracts. Ataxia of gait and limbs probably reflects
degeneration of spinocerebellar tracts and thus impairments of sensory feedback to the
cerebellum.
Vitamin E Dejiciency 5,29,30,39,40,46,47
Vitamin E, a highly fat-soluble vitamin, is essential for normal neurologic function.
Severe and prolonged vitamin E deficiency produces spinocerebellar. degeneration in a
number of inherited and acquired· disorders. The most severe vitamin E deficiency state
that occurs in humans is due to an inherited failure to synthesis apoprotein B, which is
necessary for the intestinal absorption of fat. The result is extremely low levels of circulating
lipids and fat-soluble vitamins. Serum vitamin E may be undetectable from birth. Patients
with vitamin E deficiency may present in adolescence with progressive ataxia, areflexia, and
proprioceptive ·1055, reflecting the degeneration of posterior column and spinocerebellar
tracts in the spinal cord and a loss of large myelinated fibers in the peripheral nervous
system. Vitamin E deficiency and similar neurologic symptoms may also occur in patients
with diseases affecting bile salt concentrations in the small intestine or disturbing the
absorptive surface of the gut.
Neoplastic and Paraneoplastic Disorders
Neoplastic disease, whether located within or near the cerebellum, or at some distant
site, can adversely affect cerebellar function.
Paraneoplastic Cerebellar Degeneration5,29,30,48-S1
All areas of the nervous system are susceptible to the deleterious effects of systemic
carcinoma. In addition to effects on the cerebellum, neoplasm may cause encephalopathy,
peripheral neuropathy, myopathy, and defects of neuromuscular transmission (e.g., Lambert
Eaton myasthenic syndrome; Chapter 14). A nonmetastatic paraneoplastic degeneration of
Disorders oj the Cerebellum and Its Connnections
459
the cerebellar cortex is the most common paraneoplastic syndrome that affects the central
nervous system. Symptoms may develop before or after· discovery of the tumor. They
usually begin with gait ataxia and over a few days or weeks progress to severe truncal and
limb ataxia, with dysarthria and often with abnormal ocular movements. Vertigo is
common and patients frequently complain of diplopia. Symptoms may progress in severity
for several weeks or months and, then stabilize. Unfortunately, by this stage, the patient may
already be severely disabled. Often superimposed upon the cerebellar deficits are manifes
tations of a more diffuse paraneoplastic encephalopathy, including cognitive deterioration,
bulbar palsy, and limb weakness.
Pathologic examination usually reveals a severe loss of Purkinje cells throughout the
cerebellum, with or without evidence of inflammation. 33 ,48,49,52,53 Some patients may have
more widespread pathologic findings, including degeneration of spinocerebellar tracts,
dorsal columns, and corticospinal tracts. Although the pathogenesis of paraneoplastic
cerebellar degeneration is poorly understood, theories proposed to explain these remote
effects of malignancy focus on nutritional deficiency, viral infections, and autoimmune
mechanisms. Evidence such as clinical improvement with plasmapheresis and the presence
of anti-Purkinje cell antibodies supports the notion of disturbed immune activity:52-55
The neurologic status of these patients can improve markedly with treatment of the
underlying neoplasm.
Paraneoplastic cerebellar degeneration occurs most often in association with lung,
breast, or ovarian cancer or Hodgkin's disease. Up to 50% of all patients over the age of 40
presenting with degenerative cerebellar disease may have an underlying neoplasm.
Primary Tumors 5 ,28,29,56,57
The cerebellum and adjacent structures may also constitute the site of primary tumor
development. Posterior fossa tumors represent about one third of all intracranial tumors in
adults and about two thirds in children. As with other regions of the central nervous system,
these tumors may arise from either glial cells (e.g., astrocytomas) or neural cells (e.g.,
medulloblastomas). No particular type predominates in adults, but in children, most are
astrocytomas or medulloblastomas. 56 Lesions limited to just the cerebellum are rare, but are
most often due to the presence of a discrete tumor. Cerebellar signs may occur with tumors
of the cerebellum itself or with those arising in the fourth ventricle or brainstem.
As with any posterior fossa mass, nonspecific signs and symptoms reflecting increased
intracranial pressure or compression of the brainstem may also develop. Headache, nausea,
and vomiting may be accompanied to a variable extent by cranial nerve deficits, pyramidal
tract signs, sensory disturbances, and decreasing consciousness. An expanding cerebellar
mass may compress the medulla and portions of the cervical spine to the extent that
infarction occurs and life-threatening abnormalities of cardiovascular and respiratory
regulation ensue.
Tumors of the cerebellopontine angle, although they may be considered extracerebellar,
are not an uncommon neoplastic cause of cerebellar signs. These tumors damage the inferior
cerebellar peduncle, and the usual resulting complaints are impaired balance, ~t~xi~, v~rtigQ,
and speCific cranial nerve defiCits(ecg~ ,healing loss, .oculomotor disturbances, and facial
paralysis). The most common turoorsin this area are acoustic neuromas, which develop in
the vestibulocochlear nerve.
Metastatic Disease 5 ,IS,29,S7
In adults, metastasis is the most common source of neoplasia in the posterior fossa
(Fig. 19-6). Common primary tumor sites include the lung (about 50%), followed by the
breast, kidney, and melanoma. The effects on the cerebellum reflect the location and extent
of involvement. Focal neurologic deficits include limb or truncal ataxia or cranial nerve
dysfunction. More generalized symptoms such as headache, nausea, or vomiting may result
from obstructive hydrocephalus and elevated intracranial pressure.
460
Disorders of Central Motor Control
Figure 19-6. Cerebellar Metas
tases. Two hemorrhagic metastases
(Arrows) from carcinoma of the lung
are visible in the cerebellar hemi
spheres. (From Hirano, A (ed): Color
Atlas of Pathology of the Nervous
System, ed 2. 19aku-Shoin, Tokyo,
p 62, with permission.)
Developmental Disorders 5 ,29,3o,58-62
Congenital structural anomalies of the cerebellum are not uncommon and probably
reflect both genetic (familial) and teratogenic factors. The cerebellum has the longest
period of embryologic development of any major structure of the brain and is consequently
vulnerable to teratogenic insults longer than most parts of the nervous system. The
developing cerebellum is susceptible to the toxic effects of many drugs, chemicals, viral
infections, radiation, and ischemic-hypoxic insults.
Malformation of the cerebellum may be focal, confined to the cerebellum, or associated
with other brains tern or cerebral abnormalities. Congenital hypoplasia or even the absence
of some or most of the cerebellum may occur. Because the vermis forms after the
hemispheres, it is more likely to be absent or underdeveloped than other parts of the
cerebellum. Although ataxia, hypotonia, tremor, and abnormal eye movements may be
present, marked cerebellar hypoplasia has been shown by imaging studies and autopsy to be
present in totally asymptomatic individuals (Fig. 19-7). A number of other malformations
of the cerebellum have been described. The Dandy-Walker malformation consists of a
ballooning of the posterior half of the fourth ventricle and hypoplasia of the cerebellar
vermis. 60,61 Swelling of the brain due to excessive cerebrospinal fluid (hydrocephalus)
almost always develops and accounts for many of the accompanying clinical manifestations.
Hypotonia, cerebellar deficits, pyramidal signs, and seizures are present to varying degrees in
about 25% of these cases. The Chiari malformations (the most common developmental
abnormality of the posterior fossa) encompass a group of anomalies of the brainstem and
cerebellum, in which there is a herniation of part of the cerebellum, medulla, and sometimes
Disorders of the Cerebellum and Its Connnections
461
!
I
·1
.~
Figure 19-7. Congenital Aplasia of the Left Cerebellar Hemisphere. The left hemisphere was almost totally
lacking in this brain of an asymptomatic adult. (From Dow, Kramer, and Robertson,S p 95, with permission.)
the pons through the foramen magnum into the upper cervical spinal canal. 62 By compress
ing the cerebellum, lower brainstem; and. cervical cord, this herniation may compromise
neural function. The Chiari malformations are frequently associated with other malforma
tions of the nervous system, such as spina bifida and hydrocephalus.
Perinatal hypoxia may produce severe cerebellar cortical atrophy; but signs of cerebellar
dysfunction are usually overshadowed by evidence of damage to the cerebral cortex and
other areas of the brain.
Disorders Due to Infection5 ,29,3o,63
A variety of organisms can infect the central nervous system, and in certain infectious
disorders cerebellar signs and symptoms may be preeminent. Both slow and conventional
viruses may produce a cerebellar syndrome. 63 Creutzfeldt-Jakob disease, for example, is
an encephalopathy resulting from~jnfecti()n with_.a so..called slow virus. It is now thought -
that almost 50% of affected patients may have a cerebellafbr ata.xiC form of this disease, in
which cerebellar deficits dominate-the clinical picture for the first several months. Encepha'::'
litis produced by a wide range of conventional viruses can also give rise to cerebellar
findings. Viral cerebellitis has been associated with polio, mumps, rubella, chickenpox, and
herpesviruses. The most common cerebellar syndrome attributed to viral infection is an
acute cerebellar ataxia that occurs in young children. Children may develop over hours or a
few days severe truncal ataxia, with less prominent limb involveme.nt. Recovery is usually
complete, although it can take up to 6 months. Bacteria, fungi, and other parasites may also
infect the cerebellum. Cerebellitis may accompany bacterial meningitis or be secondary to a
variety of systemiC bacterial infections. Ataxic syndromes, in association with meningitis or
systemic bacterial infection, are usually transient and resolve within weeks. Cerebellar
syndromes as a sole result of fungal infection are rare. Amebas, tapeworms, and other
parasites may create cerebellar cysts or masses.
.
462
Disorders of Central Motor Control
Vascular Disorders5 ,29,30,64-68
Ischemic. dIsease and hemorrhage in the posterior fossa seldom give rise to. cerebellar
signs alone. Cerebellat deficits are usually ~ccompanied by brainstem and cranial nerve
findings, including nausea, vomiting, vertigo, and visual disturbances, which may domiriate
the clinical picture.
Cerebellar hemorrhage is estimated to account for about 10% of all intracranial
hemorrhages and a few percent of all strokes (Fig. 19-8). Cerebellar hemorrhage typically
manifests as an acute onset of headache, repeated vomiting, vertigo and dizziness, and an
inability to walk orstand.64•65 Coma develops over hours or days in about 50% of these
patientsc: In many cases, cerebellar hemorrhage is not suspected until neuroimaging or
autopsy. the typical patient is hypertensive and older than 60 years of age, and frequently
has a prior history of transient neurologic symptoms.
Although cerebellar infarction is more common than cerebellar hemorrhage, it repre
sents only about 1% of all slIOkes (see Chapter 21).66-:-68 Infarction in this region, however,
has one of the highest mortality .rates, estimated to be 20% to 500h. Diagnosis is often
missed because of the wide rallge of clinical presentations. Actually. many patients have few
cerebellar signs, despite radiologic evidence ofcerebellar infarction. Newimaging techniques
have greatly increased the accuracy of diagnosis and suggest that its incidence is greater than
heretofore suspected. The cerebellum is supplied by distal branches of the posterior inferior
cerebellar artery, the anterior inferior cerebellat artery, and the superior cerebellar artery, all
of which are supplied by the basilar artery. Although cerebellar infarction usually involves
multiple vessels, occlusion of anyone of the three principal arteries supplying the
19-8. large hemorrhage
(hematoma) of the cerebellum. From
Hirano, A (ed): Color Atlas of Pathol
ogy of the Nervous System, ed 2.
19aku-Shoin, Tokyo, 1988, p 69, with
permission.)
Figure
Disorders oj the Cerebellum and Its Connnections
463
cerebellum may give rise to specific signs,and symptoms. Many different clinical patterns
may develop, but unsteadiness of gait, dizziness, nausea, and vomiting are common early
symptoms. Cerebellar infarction with edema formation can lead to sudden respiratory arrest
due to increased intracranial pressure in the posterior fossa.
Intoxications29 ,3o,69,70
Cerebellar dysfunction may occur in association with exposure to a wide variety of
toxins, including drugs, solvents, and heavy metals. These toxins may adversely affect the
cerebellum directly or as part of a more generalized encephalopathy.
Practically all drugs given at high enough doses can cause neurologic signs and
symptoms, including those indicating cerebellar dysfunction. 69,70 The drug-induced cerebel
lar syndrome is characterized by transient gait ataxia, dysarthria, and nystagmus.
Symptoms usually subside with discontinuation of the offending agent. The most common
form of this syndrome is that associated with anticonvulsant medications. 71 Certain cardiac
agents, antineoplastic agents, and lithium may produce similar findings.
Recreational or accidental exposure to a wide variety of volatile solvents may cause
ataxia along with other neurologic problems, including psychoses, cognitive impairment,
and pyramidal signs. 69,70,72,73 As with drug toxicity, these deficits are usually reversible
unless exposure has been heavy and prolonged. These volatile chemicals are ubiquitous in
our society and are found in many products, such as adhesives, solvents, aerosols, and fire
extinguishers. Unfortunately, they are increasingly a choice for recreational abuse, with
devastating neurologic consequences.
Poisoning with heavy metals such as mercury, manganese, bismuth, thallium, and lead
can also result in neurologic syndromes, including prominent ataxia. 29,30.69,70
Injury Due to Physical or Mechanical Trauma 5
Direct mechanical trauma to the head, particularly in the area of the occiput, can
produce cerebellar hemorrhage and tissue disruption (see Chapter 20).s In most physical
trauma resulting in closed-head injury, however, cerebellar dysfunction is not particularly
apparent clinically and is overshadowed by the sequelae of the rest of the central nervous
system damage. As some patients emerge from the acute phase of closed-head injury,
cerebellar deficits may become more prominent.
The cerebellum has one of the highest rates of oxygen consumption in the nervous
system and is particularly sensitive to oxygen deprivation. s Following severe brain
hypoxia, however, signs of cerebellar dysfunction may be overshadowed by diffuse cerebral
dysfunction, The cerebellum is also particularly sensitive to thermal injury.s Cerebellar
dysfunction is known to occur following hyperthermia, whether it is due to heat stroke or
prolonged fever. Radiation-induced injury to the cerebellum can result from both therapeutic
and accidental exposure to ionizing radiation, manifested as diffuse atrophy and various
.
functional deficits.
. ..
Metabolic Disorders29 - 31
A number of inherited and acquired metabolic disorders are associated with
cerebellar dysfunction. Disorders of lipids, the urea cycle, pyruvate and lactate metabolism,
and some aminoacidurias are associated with cerebellar symptoms. Some of these disorders
manifest in infancy or early childhood; others are not evident until later in life. They vary
markedly in their severity and the extent to which they are progressive. Genetically
determined metabolic disorders may give rise to either intermittent bouts of ataxia, due to
the accumulation of circulating neurotoxic substances such as ammonia, or to persistent
progressive ataxia?9-31 These metabolic disorders often cause disordered function at
,
!
....6....
Disorders of Central Motor Control
multiple sites in the nervous system. Accordingly, affected patients may present, in addition
to cerebellar signs and symptoms, additional symptoms such as vomiting, headache,
involuntary movements, seizures, confusion, and varying degrees of mental retardation.
Acquired disturbances of liver function, electrolyte balance (e.g., hyponatremia), and
endocrine activity may also produce cerebellar findings. For example, hypothyroidism may
be associated with an ataxic syndrome in both children and adults, as well as an accom
panying peripheral neuropathy described in Chapter 15.
Demyelinating and Dysmyelinating Disorders 74-76
Many of the nerve fibers of both the peripheral and central nervous systems are myeli
nated and depend on this myelin for normal impulse propagation. Myelin is disturbed in a
variety of disorders, both acquired and inherited, with resultant abnormalities in both the
speed and the quality of impulse conduction (see Chapter 22), In some of these disorders,
normal myelin may be damaged or destroyed (demyelinating diseases). In others, myelin is
never properly formed (dysmyelinating diseases), Both the spinocerebellar pathways and the
cerebellum contain abundant myelin and may be damaged by these types of disorders.
The most common of the demyelinating diseases of the CNS is multiple sclerosis (see
Chapter 22), which is characterized by multisystem demyelination and clinical features
encompassing spasticity, visual and oculomotor disturbances, urinary dysfunction, and
cerebellar deficits. 74 - 76 The classic signs of cerebellar dysfunction are common in multiple
sclerosis in a variety of combinations, which may include dysarthria, instability of head and
trunk, intention tremor, and incoordination of voluntary movements and gait. Cerebellar
signs such as nystagmus and ataxia may appear early in the disease. Although most patients
with multiple sclerosis have clinical manifestations referable to damage to many areas of the
nervous system, in a few patients, cerebellar deficits predominate throughout much of the
course of the disease. The cerebellar deficits may be severe and may make a Significant
contribution to patient disability.
Cerebellar dysfunction may result from the direct involvement of the cerebellum or
may be due to involvement of spinocerebellar tracts. Demyelinating lesions (plaques) may
be found randomly distributed throughout the cerebellar hemispheres, the peduncles, in the
vicinity of the dentate nuclei, and in the spinocerebellar tracts.
Certain dysmyelinating diseases are also associated with progressive cerebellar
dysfunction. Although cerebellar deficits are not a predominant component of the leuko
dystrophies, pathologic examination often reveals areas of demyelination throughout the
cerebellar system, as well as in the cerebrum.
RECOMMENDED READINGS
Adams, RD and Victor, M: Principles of Neurology, ed 5.
Chapter 36. Multiple Sclerosis and Allied Demyeli
nating Diseases. McGraw-Hill, New York, 1993.
Brooks, VB: The Neural Basis of Motor Control. Chapter
13. The Cerebellum. Oxford University Press, New
York, 1986.
Conner, KE and Rosenberg, RN: The Hereditary Atax
ias. Chapter 45. In Rosenberg, RN, et al (eds): The
Molecular and Genetic Basis of Neurological Disease.
Butterworth-Heinemann, Boston, 1993.
Dow, RS, Kramer, RE, and Robertson, LT: Disorders of
the Cerebellum. Chapter 37. In Joynt, RJ (ed): Clinical
Neurology, vol 3. JB Lippincott, Philadelphia, 1991.
Ghez, C: The Cerebellum. Chapter 41. In Kandel, ER,
Schwartz, JH, and Jessell, TM (eds): Principles of
Neural Science, ed 3. Appleton &: Lange, Norwalk,
CT,1991.
Gilman, S: Cerebellum and Motor Dysfunction. Chapter
23. In Asbury, AK, McKhann, GM, and McDonald,
WI (eds): Diseases of the Nervous System. Clinical
Neurobiology, ed 2. WB Saunders, Philadelphia,
1992. Gilman, S, Bloedel, JR, and Lechtenberg, R: Disorders of the Cerebellum. FA Davis, Philadelphia, 1981.
Harding, AE: The Hereditary Ataxias and Related Disor
ders. Churchill Livingstone, Edinburgh, 1984.
Harding, AE: Cerebellar and Spinocerebellar Disorders.
Chapter 77. In Bradley, WG, et al (eds): Neurology in
Clinical Practice, vol II. Butterworth-Heinemann,
Boston, 1990.
Harding, AE and Deufel, T (eds): Inherited Ataxias. Adv
Neurol 61:1, 1993.
.~
\
I
Disorders of the Cerebellum and Its Connnections
Ito, M: The Cerebellum and Neural Control. Raven
Press, New York, 1984.
King, JS (ed): New Concepts in Cerebellar Neurobiol
ogy. Alan R. Liss, New York, 1988.
Lechtenberg, R (ed): Handbook of Cerebellar Diseases.
Marcel Dekker, New York, 1993.
465
Matthews, WB, et al (eds): McAlpine's Multiple Sclero
sis, ed 2. Churchill LiVingstone, Edinburgh, 1991.
Stumpf, DA: Cerebellar Disorders. In Rosenberg, RN
(ed): Comprehensive Neurology. Raven Press, New
York, 1991.
REFERENCES 1. Ghez, C: The Cerebellum. Chapter 41. In Kandel,
ER, Schwartz, jH, and jessen, TM (eds): Principles
of Neural Science, ed 3. Appleton &: Lange, Nor
walk, CT, 1991.
2. Gilman, S: Cerebellum and Motor Dysfunction.
Chapter 23. In Asbury, AK, McKhann, GM, and
McDonald, WI (eds): Diseases of the Nervous
tem: Clinical Neurobiology, ed 2. WB Saunders,
Philadelphia, 1992.
3. Ito, M: The Cerebellum and Neural Control. Raven
Press, New York, 1984.
4. Lechtenberg, R: Signs and Symptoms of Cerebellar
Disease. Chapter 4. In Lechtenberg, R (ed): Hand
book of Cerebellar Diseases, Marcel Dekker, New
York, 1993.
5. Dow, RS, Kramer, RE, and Robertson, LT: Disorders
of the Cerebellum. Chapter 37. In joynt, RJ (ed):
Clinical Neurology, vol 3. JB Lippincott, Philadel
phia, 1991.
6. Thompson, PD, and Day, BL: The Anatomy and
PhYSiology of Cerebellar Disease. Adv Neurol
61:15, 1993.
7. Rothwell, JC: Control of Human Voluntary Move
ment. Chapter 9. The Cerebellum. Aspen Publish
ers, Rockville, MD, 1987.
8. laLonde, Rand Botez, MI: The Cerebellum and
Learning Processes in Animals. Brain Res Rev
15:325, 1990.
9. Glickstein, M and Yeo, C: The Cerebellum and
Motor Leaming.j Cogn Neurosci 2:69,1990.
10. Lye, RH, et al: Effects of a Unilateral Cerebellar
Lesion on the Acquisition of Eye-Blink Condition
ing in Man. J Physiol (Lond) 403:58p, 1988.
11. Topka, H: Deficit in Classical Conditioning in Pa
tients with Cerebellar Degeneration. Brain 116(Pt
4):961, 1993.
12. Sanes, jN, Dimitrov; B, and HaUett, M: Motor
Learning in Patients with Cerebellar Dysfunction.
Brain 113(Pt 1):103, 1990.
13. Decety, j, et al: The Cerebellum Participates in
Mental Activity: Tomographic Measurement of Re
gional Blood Flow. 535:313, 1990.
14. Petersen, SE, et al: Position Emission Tomographic
Studies of the Cortical Anatomy of Single-Word
Processing. Nature 331:585, 1988.
15. Samet, HB and Alcala, H: Human Cerebellar Hypo
plaSia. Arch Neuro137:300, 1980.
16. Fiez, JA, et al: Impaired Non-Motor Learning and
Error Detection Associated with Cerebellar Dam
age: A Single Case Study. Brain 115 (Pt. 1):155, 1992
17. Akshoomoff, NA, et al: Contribution of the Cer
ebellum to Neuropsychological Functioning: Evi
dence from a Case of Cerebellar Degenerative Dis
order. Neuropsychologia 30:315; 1992.
18. Ackermann, H, et al: Speech Deficits in Ischaemic
Cerebellar Lesi'ons. j Neurol 239:273, 1992.
19. Murakami, Jw, et al: Reduced Cerebellar Hemi
sphere Size and Its Relationship to Vermal Hypopla
sia in Autism. Arch Neurol 46:689, 1989.
20. Kemper, TL and Banman, ML: The contribution of
neuropathologic studies to the understanding of
autism. Neurol Clin 11:175, 1993.
2l. Holroyd, S, Reiss, AL, and Bryan, RN: Autistic
Features in Jouberts Syndrome: A Genetic Disorder
with Agenesis of the Cerebellar Vermis. Bioi Psy
chiatry 29:287, 1992.
22. Snider, SR: Cerebellar Pathology in Schizophrenia:
Cause or Consequence? Neurosci Biobehav Rev
6:47,1982.
23. Volkow; ND, et al: Low Cerebellar Metabolism in
Medicated Patients with Schizophrenia. Am J Psy
chiatry 149:686, 1992.
24. Sandyk, R, Kay, SR, and Merriam, AE: Atrophy of
the Cerebellar Vermis: Relevance to the SymptOms
of Schizophrenia. Int J Neurosci 57:205, 1981.
25. Martin, JH: Neuroanatomy: Text and Atlas. Apple
ton &. Lange, Norwalk, CT, 1989.
26. Dichgans, j, and Diener, HC: Clinical Evidence for
Functional Compartmentalization of the Cerebel
lum. In Bloedel, JR, Dichgans, J, and Precht, W
(eds): Cerebellar Functions. Springer-Verlag, Berlin,
1985.
27. Chadwick, D, Cartlidge, N, and Bates, D: Medical
Neurology. Chapter 15. Inherited and Degenerative
Disorders of the Central Nervous System. Churchill
Livingstone, Edinburgh, 1989.
28. Conner, KE and Rosenberg, RN: The Hereditary
Ataxias. Chapter 45. In Rosenberg, RN, et al (eds):
The Molecular and Genetic Basis of Neurological
Disease. Butterworth-Heinemann, Boston, 1993.
29. Harding, AE: Cerebellar and Spinocerebellar Disor
ders. Chapter 77. In Bradley, WG, et al (eds):
Neurology in Clinical Practice, vol II. Butterworth
Heinemann, Boston, 1990.
30. Harding, AE: Hereditary Ataxias and Related Disor
ders. Chapter 88. In Asbury, AK, McKhann, GM,
and McDonald, WI (eds): Diseases of the Nervous
System: Clinical Neurobiology, ed 2. WB Saunders,
Philadelphia, .l9~J2.
..
.
. . . ~.
31. Harding, AE: Clinical Features and Classification of
Inherited Ataxias. Adv Neurol 61:1, 1993.
32. Rosenberg, RN and Grossman, A: Hereditary
Ataxia. Neurol Clin 7:25, 1989.
33. Oppenheimer, DR and Esiri, MM: Diseases of the
Basal Ganglia, Cerebellum, and Motor Neurons.
Chapter 15. In Adams, jH and Duchen, LW (eds):
Greenfield's Neuropathology, ed 5. Oxford Univer
sity Press, New York, 1992.
34. Manyam, BV: Friedreichs Disease. Chapter 33. In
Lechtenberg, R {ed}:"Handbook of Cerebellar Dis
eases. Marcel Dekker, New York, 1993.
466
Disorders of Central Motor Control
35. Duvosin, RC and Plaitakis, A (eds): The Olivopon
tocerebellar Atrophies. Adv Neurol 41:1, 1984.
36. Gatti, RA: Candidates for the Molecular Defect in
Ataxia Telangiectasia. Adv NeuroI61:127, 1993.
37. Jeret, JS and Lechtenberg, R: Ataxia-Telangiectasia.
Chapter 40. In Lechtenberg, R (ed): Handbook of
Cerebellar Diseases. Marcel Dekker, New York, 1993.
38. Taylor, AMR, et al: Variant Forms of Ataxia Telan
giectasia. J Med Genet, 24:669, 1987.
39. So, YT and Simon, RP: Deficiency Diseases of the
Nervous System. Chapter 62. In Bradley, WG, et al
(eds): Neurology in Clinical Practice, vol 2.
Butterworth-Heinemann, Boston, 1990.
40. Adams, RD and Victor, M: Principles of Neurology,
ed 4. Chapter 39. Diseases of the Nervous System
Due to Nutritional Deficiency. McGraw-Hill Infor
mation Services, New York, 1989.
41. Womer, TM: Effects of Alcohol. Chapter 46. In
Lechtenberg, R (ed): Handbook of Cerebellar Dis
eases. Marcel Dekker, New York, 1993.
42. Butterworth, RF: Pathophysiology of Cerebellar
Dysfunction in the Wernicke-Korsakoff Syndrome.
CanJ Neurol Sci 20(suppl 3):5123, 1993.
43. Neiman, J, et al: Movement Disorders in Alcohol
ism: A Review. Neurology 40:741, 1991.
44. Lindboe, CF and Loberg, EM: The Frequency of
Brain Lesions in Alcoholics: Comparison Between
the 5-year Periods 1975-1979 and 1983-1987. J
Neurol Sci 88:107, 1988.
45. Pratt, OE, et al: Genesis of Alcoholic Brain Tissue
Injury. Alcoholism 25:217, 1990.
46. Muller, DPR, Lloyd, JK, and Wolff, OH: Vitamin E
and Neurological Function. Lancet 1:225, 1983.
47. Harding, AE: Vitamin E and the Nervous System.
CRC Crit Rev Neurobiol 3:89, 1987.
48. Dropcho, EJ: Paraneoplastic Cerebellar Disorders.
Chapter 15. In Lechtenberg, R (ed): Handbook of
Cerebellar Diseases. Marcel Dekker, New York, 1993.
49. Posner, JB: Paraneoplastic Syndromes. Chapter 83.
In Asbury, AK, McKhann, GM, and McDonald, WI
(eds): Diseases of the Nervous System: Clinical
Neurobiology, ed 2. WB Saunders, Philadelphia,
1992.
50. Waterhouse, DM, Natale, RB, and Cody, RL: Breast
Cancer and Paraneoplastic Cerebellar Degenera
tion. Cancer 78:1835, 1991.
5 l. Posner, JB: Paraneoplastic Cerebellar Degeneration.
CanJ Neurol Sci 20(suppI3):S1l7, 1993.
52. Posner,JB: PathogeneSiS of Central Nervous System
Paraneoplastic Syndromes. Rev Neurol 148:502,
1992.
53. Graus, F and Rene, R: Clinical and PatholOgical
Advances on Central Nervous System Paraneoplas
tic Syndromes. Rev Neurol 148:496, 1992.
54. Anderson, NE, Rosenblum, MK, and Posner, JB:
Paraneoplastic Cerebellar Degeneration: Clinical
Immunological Correlations. Ann Neurol 24:559,
1988.
55. Dropcho, EJ: Autoimmune Aspects of Paraneoplas
tic Cerebellar Degeneration. Prog Neuro Endocrin
Immunol 3:90, 1990.
56. Roberts, RO, et al: Medulloblastoma: A Population
Based Study of 532 Cases. J Neuropathol Exp
Neurol 50:134, 1990.
57. Lechtenberg, R (ed): Handbook of Cerebellar Dis
eases. Part Iv. Neoplastic Disease. Marcel Dekker,
New York, 1993.
58. Lechtenberg, R (ed): Handbook of Cerebellar Dis
eases. Part m. Structural Disease. Marcel Dekker,
New York, 1993.
59. Harding, BN: Malformations of the Nervous Sys
tem. Chapter lO. In Adams, JH, and Duchen, LW
(eds): Greenfield!> Neuropathology, ed 5. Oxford
University Press, New York, 1992.
60. Bordarier, C and Aicardi, J: Dandy-Walker Syn
drome and Agenesis of the Cerebellar Vermis: Diag
nostic Problems and Genetic Counselling. Dev Med
Child Neurol 32:285, 1990.
61. Johanson, CE: The Dandy~Walker Syndrome. In
Myrianthopoulos, N-C (ed): Handbook of Clinical
Neurology, vol 6. Malformations. Elsevier, New
York, 1987, pp 323-336.
62. Banberger, BC: The Chiari II Malformation. In
Myrianthopoulos N-C (ed): Handbook of Clinical
Neurology, vol 6. Malformations. ElseVier, New
York, 1987, pp 403-42.
63. Tateishi, J, Kita Moto, T, and Doh-ura, K: Slow
Transmissible Diseases Affecting the Cerebellum. In
Lechtenberg, R (ed): Handbook of Cerebellar Dis
eases. Marcel Dekker, New York, 1993.
64. Shafer, SQ and Brust, JCM: Cerebellar Hemorrhage.
Chapter 17. In Lechtenberg, R (00): Handbook of
Cerebellar Diseases. Marcel Dekker, New York,
1993.
65. Dunne, JW, Chakera, T and Kermode, 5: Cerebellar
Hemorrhage-Diagnosis and Treatment: A Study of
75 Consecutive Cases. QJ Med 64:739, 1987.
66. Amarenco, P, Hauw, JJ, and Caplan, LR: Cerebellar
Infarctions. Chapter 16. In Leclitenberg, R (ed):
Handbook of Cerebellar Diseases. Marcel Dekker,
New York, 1993.
67. Amarenco, P, Hauw; 11, and Gautier, JC: Arterial
Pathology in Cerebellar Infarction. Stroke 21:1299,
1990.
68. Kase, CS, et al: Cerebellar Infarction. Clinico
Anatomic Correlations. J Neurol 237: 160, 1990.
69. Johnson, LM, Hubble, JP, and Koller, WC: Effect of
Medications and Toxins on Cerebellar Function.
Chapter 45. In Lechtenberg, R (ed): Handbook of
Cerebellar Diseases. Marcel Dekker, New York,
1993.
70. Goetz, CG and Cohen, MM: Neurotoxic Agents.
Chapter 20. In Joynt, RJ (ed): Clinical Neurology,
vol 2. JB Lippincott, Philadelphia, 1992.
71. McLain, LW, Martin,]T, and Allen, JH: Cerebellar
Degeneration Due to Chronic Phenytoin Therapy.
Ann Neurol 7:18, 1980.
72. Lotin, Y: Chronic NeurolOgical Toxicity Associated
with Exposure to Volatile Substances. Hum Toxicol
8:293, 1989.
73. Fomazzari, L, et al: Cerebellar, Cortical, and Func
tional Impairment in Toluene Abusers. Acta Neurol
Scand 67:319, 1983.
74. Troiano, R: Multiple Sclerosis and Other Demyeli
nating Diseases. Chapter 43. In Lechtenberg, R
(ed): Handbook of Cerebellar Diseases. Marcel De
kker, New York, 1993.
75. Matthews, WB, et al (eds): McAlpines Multiple
Sclerosis, 00 2. Churchill Livingstone, Edinburgh,
1991.
76. Adams, RD.and Victor, M: Principles of Neurology,
ed 5. Chapter 36. Multiple Sclerosis and Allied
Demyelinating Diseases. McGraw-Hill, New York,
1993.