Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Perception of infrasound wikipedia , lookup
Cognitive neuroscience of music wikipedia , lookup
Microneurography wikipedia , lookup
Dual consciousness wikipedia , lookup
Aging brain wikipedia , lookup
History of neuroimaging wikipedia , lookup
Diffusion MRI wikipedia , lookup
Circumventricular organs wikipedia , lookup
Neuroanatomy of memory wikipedia , lookup
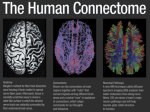
Diffusion-Tensor MR Imaging and Tractography at 3T: Anatomy and Clinical Applications. Poster No.: C-0542 Congress: ECR 2011 Type: Educational Exhibit Authors: M. Recio , L. C. Hernández González , V. Martinez de Vega , 1 2 1 1 1 1 M. Jimenez De La Peña , S. Gil Robles , J. Carrascoso Arranz , 1 1 1 1 R. Cano Alonso , E. Alvarez , L. Herraiz Hidalgo ; Madrid/ES, 2 Oviedo/ES Keywords: Neuroradiology brain, MR-Diffusion/Perfusion, Diagnostic procedure, Pathology DOI: 10.1594/ecr2011/C-0542 Any information contained in this pdf file is automatically generated from digital material submitted to EPOS by third parties in the form of scientific presentations. References to any names, marks, products, or services of third parties or hypertext links to thirdparty sites or information are provided solely as a convenience to you and do not in any way constitute or imply ECR's endorsement, sponsorship or recommendation of the third party, information, product or service. ECR is not responsible for the content of these pages and does not make any representations regarding the content or accuracy of material in this file. As per copyright regulations, any unauthorised use of the material or parts thereof as well as commercial reproduction or multiple distribution by any traditional or electronically based reproduction/publication method ist strictly prohibited. You agree to defend, indemnify, and hold ECR harmless from and against any and all claims, damages, costs, and expenses, including attorneys' fees, arising from or related to your use of these pages. Please note: Links to movies, ppt slideshows and any other multimedia files are not available in the pdf version of presentations. www.myESR.org Page 1 of 45 Learning objectives We review the normal anatomy of the white matter (WM) tracts as they appear on directional diffusion tensor imaging (DTI) color maps and tractography. Anatomic gross dissection photographs are correlated with tractography to review the anatomy of those tracts, which are readily seen in most cases. We describe the principles of diffusion contrast and anisotropy, as well as their main clinical applications in developmental abnormalities, demyelinating disease, ischemic disease, infectious diseases, neurodegenerative disordes, neoplasms and preoperative studies. 2 DTI MR images were obtained with a 3T system and b values of 0 and 1000 s/mm were used. Our imaging protocol consisted of 82 diffusion encoding gradient directions when comparing with anatomic sections from cadavers and 25 diffusion encoding gradient directions when clinical applications were under evaluation. Background Diffusion magnetic resonance (MR) imaging is evolving into a potent tool in the examination of the central nervous system. Although it is often used for the detection of acute ischemia, evaluation of directionality in a diffusion measurement can be useful in white matter, which demonstrates strong diffusion anisotropy. Techniques such as diffusion-tensor imaging offer a glimpse into brain microstructure at a scale that is not easily accessible with other modalities, in some cases improving the detection and characterization of white matter abnormalities. Diffusion MR tractography offers an overall view of brain anatomy, including the degree of connectivity between different regions of the brain. Imaging findings OR Procedure details Diffusion contrast is based on the self-diffusion of water molecules in tissue. Although a variety of sequences are now used to acquire DW images, all DW sequences include two equal and opposing motion-probing gradients. Diffusion is anisotropic (directionally dependent) in WM fiber tracts, as axonal membranes and myelin sheaths represent barriers to the motion of water molecules in directions not parallel to their own orientation. Page 2 of 45 The direction of maximum diffusivity has been shown to coincide with the WM fiber tract orientation . This information is contained in the diffusion tensor, a mathematic model of diffusion in three-dimensional space. The tensor model of diffusion consists of a 3x3 matrix derived from diffusivity measurements in at least six noncollinear directions. Fractional anisotropy (FA) is an index ranging from 0 (isotropic) to 1 (maximally anisotropic)) The direction of maximum diffusivity may be mapped by using red, green, and blue (RGB) color channels with color brightness modulated by FA, resulting in a convenient summary map from which the degree of anisotropy and the local fiber direction can be determined. The convention we used for directional RGB color mapping is red for left-right, green for anteroposterior,and blue for superior-inferior. We employed b value of b 0 and 1000 s/mm2 and 82 encoding gradient directions in the comparative study with anatomic sections from cadavers , meanwhile 25 encoding gradient directions directions were used when evaluating different clinical applications. White matter tracts were estimated with tractography. Tracking was initiated from a start location (or seed point) in both forward and backward directions. The ROIs were chosen to enclose tract cross sections that were visible in any of the axial, sagittal, or coronal directional color maps. Fiber trajectories are displayed with colors superimposed on gray-scale anatomic images in various three dimensional projections. Note that, unlike directional color maps in which directional information is color-coded, individual tractograms are displayed by using fixed colors which are arbitrarily chosen.(Figure 1) on page 9, (Figure 2) on page 10, (Figure 3) on page 11 WHITE MATTER FIBER CLASSIFICATION • Association fibers interconnect cortical areas in each hemisphere. Association fibers typically identified on DTI color maps include: cingulum, superior and inferior occipitofrontal fasciculi, uncinate fasciculus, superior longitudinal (arcuate) fasciculus, and inferior longitudinal (occipitotemporal) fasciculus. • Projection fibers interconnect cortical areas with deep nuclei, brain stem, cerebellum, and spinal cord. There are both efferent (corticofugal) projection fibers (cortico-spinal, cortico-bulbar, and cortico-pontine) and afferent (corticopetal) projection fibers (medial lemniscus; anterior, superior and posterior thalamic radiation; inferior spinocerebellar fascicles or Flechsig's fasciculus, superior spinocerebellar fascicles or Gowers' tract and optic radiation). • Commissural fibers interconnect similar cortical areas between opposite hemispheres (corpus callosum, anterior commissure, posterior commissure, interthalamic gray commissure or intermediate mass and Psalterium or David ´s lyra). ASSOCIATION FIBERS Page 3 of 45 Cingulum:The cingulum begins in the parolfactory area of the cortex below the rostrum of the corpus callosum, then courses within the cingulate gyrus, and, arching around the entire corpus callosum, extends forward into the parahippocampal gyrus and uncus. It interconnects portions of the frontal, parietal, and temporal lobes. Its arching course over the corpus callosum resembles the palm of an open hand with fingertips wrapping beneath the rostrum of the corpus callosum. Superior Occipitofrontal Fasciculus: Whereas the cingulum wraps around the superior aspect of the corpus callosum, the superior occipitofrontal fasciculus lies beneath it. It connects occipital and frontal lobes, extending posteriorly along the dorsal border of the caudate nucleus. Portions of the superior occipitofrontal fasciculus parallel the superior longitudinal fasciculus but they are separated from the superior longitudinal fasciculus by the corona radiata and internal capsule (Figure 4) on page 12. Inferior Occipitofrontal Fasciculus: The inferior occipitofrontal fasciculus also connects the occipital and frontal lobes but is far inferior compared with the superior occipitofrontal fasciculus. It extends along the inferolateral edge of the claustrum, below the insula. Posteriorly, the inferior occipitofrontal fasciculus joins the inferior longitudinal fasciculus, the descending portion of the superior longitudinal fasciculus, and portions of the geniculocalcarine tract to form most of the sagittal stratum, a large and complex bundle that connects the occipital lobe to the rest of the brain. The middle portion of the inferior occipitofrontal fasciculus is bundled together with the middle portion of the uncinate fasciculus. Uncinate Fasciculus Uncinate is from the Latin uncus meaning "hook." The uncinate fasciculus hooks around the lateral fissure to connect the orbital and inferior frontal gyri of the frontal lobe to the anterior temporal lobe. The anterior aspect of this relatively short tract parallels, and lies just inferomedial to, the inferior occipitofrontal fasciculus. Its midportion actually adjoins the middle part of the inferior occipitofrontal fasciculus before heading inferolaterally into the anterior temporal lobe. (Figure 5) on page Superior Longitudinal (arcuate) Fasciculus:The superior longitudinal fasciculus is a massive bundle of association fibers that sweeps along the superior margin of the insula in a great arc, gathering and shedding fibers along the way to connect frontal lobe cortex to parietal, temporal, and occipital lobe cortices. The superior longitudinal fasciculus is the largest association bundle. (Figure 6) on page 14 Inferior Longitudinal (occipitotemporal) Fasciculus: The inferior longitudinal fasciculus: connects temporal and occipital lobe cortices. This tract traverses the length of the temporal lobe and joins with the inferior occipitofrontal fasciculus, the inferior aspect Page 4 of 45 of the superior longitudinal fasciculus, and the optic radiations to form much of the sagittal stratum traversing the occipital lobe. (Figure 7) on page 15 PROJECTION FIBERS: Corticospinal, Corticopontine, and Corticobulbar: The corticospinal and corticobulbar tracts are major efferent projection fibers that connect motor cortex to the brain stem and spinal cord. Corticospinal fibers converge into the corona radiata and continue through the posterior limb of the internal capsule to the cerebral peduncle on their way to the lateral funiculus. Corticobulbar fibers converge into the corona radiata and continue through the genu of the internal capsule to the cerebral peduncle where they lie medial and dorsal to the corticospinal fibers. Corticobulbar fibers predominantly terminate at the cranial motor nuclei. (Figure 8) on page 16 The thalamic fibers (anterior, superior, and posterior thalamic radiations: The anterior thalamic radiation interconnects anterior and medial thalamic nuclei with the frontal lobe (Figure 9) on page 17; the superior thalamic radiation joins ventral group of thalamic nuclei with the motor sensory areas and adjoining parts of frontal and parietal lobes (Figure 10) on page 18.The posterior thalamic radiation joins occipital and posterior parietal cortex with posterior thalamus including pulvinar; it includes optic radiation from lateral geniculate body (Figure 11) on page 19. Geniculocalcarine Tract (optic radiation):The optic radiation connects the lateral geniculate nucleus to occipital (primary visual) cortex. The more inferior fibers of the optic radiation sweep around the posterior horns of the lateral ventricles and terminate in the calcarine cortex; the more superior fibers take a straighter, more direct path. The optic radiation mingles with the inferior occipitofrontal fasciculus, inferior longitudinal fasciculus, and inferior aspect of the superior longitudinal fasciculus to form much of the sagittal stratum in the occipital lobe (Figure 12) on page 20. Medial lemniscus: It is part of the posterior column-medial lemniscus system, which transmits touch, vibration sense, as well as tthe pathway for propioception. Axons of cells within nucleus gracilis and nucleu cuneatus cross as internal arcuate fibers and form the medial lemniscus. The medial lemniscus carries axons from most of the body and synapses in the ventral posterolateral nucleus of the thalamus , at the level of the mamilary bodies. Sensory axons transmitting information from the head and neck via the trigeminal nerve synapse at the ventral posteromedial nucleus of the thalamus. The superior thalamic radiation connect the ventral posterolateral nucleus of the thalamus Page 5 of 45 to the postcentral gyrus (somatosensory cortex) of the cerebral cortex (areas 3, 1, 2) (Figure 13) on page 21. Inferior spinocerebellar fascicles or Flechsig's fasciculus: The inferior spinocerebellar tract conveys inconscient propioceptive information from the body to the cerebellum. Proprioceptive information is taken to the spinal cord via central processes of dorsal root ganglia (first order neurons). These central processes travel throughth the dorsal horn where they synapse with second order neurons of Clarke's nucleus. Axon fibers from Clarke's Nucleus convey this proprioceptive information in the spinal cord in the peripheral region of the posteriolateral funiculus ipsilaterally until it reaches the cerebellum, where unconscious proprioceptive information is processed. Superior spinocerebellar fascicles or Gowers' tract: The superior spinocerebellar tract conveys propioceptive information from the body to the cerebellum. Originates from ventral horn at lumbosacral spinal levels. Axons first cross midline in the spinal cord and run in the ventral border of the lateral funiculi. These axons ascend up to the pons where they join the superior cerebellar peduncle to enter the cerebellum. Middle cerebellar peduncles: The largest of the three paired peduncles, composed mainly of fibers that originate from the pontine nuclei, cross the midline in the basilar part of the pons, and emerge on the opposite side as a massive bundle arching dorsally along the lateral side of the pontine tegmentum into the cerebellum. Via this connection, the cerebellum receives a copy of the information for muscle movement that the pyramidal tract is carrying down to lower motor neurons (Figure 14) on page 22. COMMISSURAL FIBERS: Corpus Callosum: By far the largest WM fiber bundle, the corpus callosum is a massive accumulation of fibers connecting corresponding areas of cortex between the hemispheres. Fibers traversing the callosal body are transversely oriented, whereas those traversing the genu and splenium arch anteriorly and posteriorly to reach the anterior and posterior poles of the hemispheres (Figure 15). on page 23 Anterior Commissure: The anterior commissure crosses through the lamina terminalis. Its anterior fibers connect the olfactory bulbs and nuclei; its posterior fibers connect middle and inferior temporal gyri. Posterior Commissure: The posterior commissure (also known as the epithalamic commissure) is a rounded band of white fibers crossing the middle line on the dorsal Page 6 of 45 aspect of the upper end of the cerebral aqueduct. It is important in the bilateral pupillary light reflex. Interthalamic gray commissure or intermediate mass: The medial surface of the thalamus constitutes the upper part of the lateral wall of the third ventricle, and is connected to the corresponding surface of the opposite thalamus by a flattened gray band, the Interthalamic adhesion. Psalterium or David ´s lyra: The lateral portions of the body of the fornix are joined by a thin triangular lamina, named the psalterium (lyra). This lamina contains some transverse fibers that connect the two hipoccampi across the middle line and constitute the commissure of fornix (hippocampal commissure) (Figure 16) on page 24. ROM A FUNCTIONAL STANDPOINT THE MOST IMPORTANT FASCICULUS ARE: - Pyramidal tract (motor studies). - Medial lemniscus and superior corona radiata (sensory studies). - Meyer´s loop and optical radiations (visual studies). - Arcuate and inferior frontooccipital fasciculilanguage assessment): Arcuate fasciculus lesions cause paraphasia phonetics (conduction aphasia) and inferior longitudinal fasciculus lesions cause semantic paraphasias. CLINICAL APPLICATIONS : There are many pathological processes that affect anisotropic diffusion. The main clinical applications are: Myelination process: In premature newborns, increased anisotropy is found in developing cortical gray matter rather than in unmyelinated white matter, and cortical anisotropy steadily decreases during the first few months of life. DTI can assess the process of myelination. Developmental brain disorders: DT I allows the study of abnormal interhemispheric connections in cases of complete or partial agenesis of the corpus callosum. In lissencephaly, tractography of the grossly abnormal subcortical and deep white matter has demonstrated an incomplete development of the fornix and cingulate tracts. In Page 7 of 45 cases of alobar holoprosencephaly , absence of corticospinal tracts have been observed by means of DTI . Many white matter tract structures, such as the middle cerebellar peduncles, were found to be smaller in alobar holoprosencephaly than in semilobar or lobar holoprosencephaly. Furthermore, the size of the corticospinal tracts and middle cerebellar peduncles in all three variants was found to correlate with neurodevelopmental status. Joubert syndrome shows aberrant connections in abnormal superior cerebellar peduncles (Figure 17) on page 25. Demyelinating disease: Diffusion tensor is an effective tool in the assessment of white matter involvement, specially for the purposes of quanting the anisotropy and to perform to follow up studies in patients with multiple sclerosis. DTI imaging allows to control the degree of cortico-spinal tract involvement (Figure 18) on page 26 (Figure 19) on page 27. on page 26 Hypoxic ischemic disease: Tractography is useful in assessing both the integrity of the different fibers in the ischemic area and prognosis: We use it to establish a prognosis in children with congenital hemiparesis valuing the FA in the cortico-spinal tract. Thus a decrease <3% suggests mild hemiparesis, decreased values ranging from 18%-46% suggest moderate hemiparesis , and values higher than 47% suggest severe hemiparesis. In cases of cystic cavities of encephalomalacia or porencephalic. wallerian degeneration occurs, after stroke, there is a decrease in FA values (Figure 20) on page 28 (Figure 21) on page 29 on page 28 (Figure 22). on page 30 on page 28 Infectious diseases: Encephalitis, particularly herpetic encephalitis causes marked impairment of cortical and white matter with involvement of temporal lobes, limbic system and insular region . affecting inferior fronto-occipital fasciculus ,uncinate fasciculus, inferior longitudinal fasciculus and cingulum (Figure 23). on page 31 Degenerative disease: Parkinson's disease presents reduced FA in the substantia nigra with normal anisotropy in caudate and putamen. lncreased diffusivity and decreased anisotropy were found in the corpus callosum and the frontal, temporal, and parietal white matter in both patients with Alzheimer disease and those with Lewy body dementia, but the occipital lobes were involved only in the latter. Multiple groups have demonstrated decreased anisotropy and increased diffusivity in the internal capsule and cerebral peduncles of patients with amyotrophic lateral sclerosis . In multisystemic atrophy (MSA) we can detect the degree of involvement of the middle cerebellar peduncles and brainstem (Figure 24) on page 32. Tumors: The goal of surgical treatment for cerebral neoplasms is to maximize the extent of tumor resection while minimizing postoperative neurologic deficits resulting from damage to intact, functioning brain. This requires preoperative or intraoperative mapping Page 8 of 45 of the tumor and its relationship to functional structures, including cerebral cortex and WM tracts. Cortical mapping can be accomplished with either functional MR imaging or intraoperative electrocortical stimulation (Figure 25) on page 33 (Figure 26) on page 34 (Figure 27) on page 35 (Figure 28) on page 36 (Figure 29) on page 37 (Figure 30) on page 38 (Figure 31) on page 39 . Preoperative mapping of vascular disease: Surgery of cavernomas is the most common vascular indication (Figure 32) on page 40 (Figure 33) on page 41 . Epilepsy: Tractography is particularly usefull in the assesment of surgical aproach, specially in resections close to Broca and Wernicke areas, as is capable of assessing the integrity of the arcuate and inferior frontooccipital fasciculus. It also allows studying the integrity of optical radiation and Meyer loop in order to prevent visual field defects (figure 34) on page 42. Phychiatric disorders: Various disorders such as attention deficit disorder in obsessive compulsive disorders, autism or schizophrenia show decreased FA in specific locations. Images for this section: Page 9 of 45 Fig. 1: Abbreviations: ACR anterior region of corona radiata, ALIC anterior limb of internal capsule, AF arcuate fasciculus , BCC body of corpus callosum, CBT corticobulbar tract, CG cingulum, CP cerebral peduncle, CST corticospinal tract, DN dentate nucleus, DSCP decussation of superior cerebellar peduncle, GCC genu of corpus callosum, ICP inferior cerebellar peduncle, IFO inferior fronto-occipital fasciculus, ILF inferior longitudinal fasciculus, MCP middle cerebellar peduncle, ML medial lemniscus, OR optic radiation, PCR posterior region of corona radiata, PLIC posterior limb of internal capsule, PTR posterior thalamic radiations, SCC splenium of corpus callosum, SCR superior region of corona radiata, SFO superior fronto-occipital fasciculus, SLF superior longitudinal fasciculus, SN substantia nigra, SRAF short-range association fibers, T tapetum, UF uncinate fasciculus and VOF vertical occipital fasciculus. Page 10 of 45 Fig. 2: Abbreviations: ACR anterior region of corona radiata, ALIC anterior limb of internal capsule, AF arcuate fasciculus , BCC body of corpus callosum, CBT corticobulbar tract, CG cingulum, CP cerebral peduncle, CST corticospinal tract, DN dentate nucleus, DSCP decussation of superior cerebellar peduncle, GCC genu of corpus callosum, ICP inferior cerebellar peduncle, IFO inferior fronto-occipital fasciculus, ILF inferior longitudinal fasciculus, MCP middle cerebellar peduncle, ML medial lemniscus, OR optic radiation, PCR posterior region of corona radiata, PLIC posterior limb of internal capsule, PTR posterior thalamic radiations, SCC splenium of corpus callosum, SCR superior region of corona radiata, SFO superior fronto-occipital fasciculus, SLF superior longitudinal fasciculus, SN substantia nigra, SRAF short-range association fibers, T tapetum, UF uncinate fasciculus and VOF vertical occipital fasciculus. Page 11 of 45 Fig. 3: Abbreviations: ACR anterior region of corona radiata, ALIC anterior limb of internal capsule, AF arcuate fasciculus , BCC body of corpus callosum, CBT corticobulbar tract, CG cingulum, CP cerebral peduncle, CST corticospinal tract, DN dentate nucleus, DSCP decussation of superior cerebellar peduncle, GCC genu of corpus callosum, ICP inferior cerebellar peduncle, IFO inferior fronto-occipital fasciculus, ILF inferior longitudinal fasciculus, MCP middle cerebellar peduncle, ML medial lemniscus, OR optic radiation, PCR posterior region of corona radiata, PLIC posterior limb of internal capsule, PTR posterior thalamic radiations, SCC splenium of corpus callosum, SCR superior region of corona radiata, SFO superior fronto-occipital fasciculus, SLF superior longitudinal fasciculus, SN substantia nigra, SRAF short-range association fibers, T tapetum, UF uncinate fasciculus and VOF vertical occipital fasciculus. Page 12 of 45 Fig. 4: Figure 4 Page 13 of 45 Fig. 5: Figure 5 Page 14 of 45 Fig. 6: Figure 6 Page 15 of 45 Fig. 7: Figure 7 Page 16 of 45 Fig. 8: Figure 8 Page 17 of 45 Fig. 9: Figure 9 Page 18 of 45 Fig. 10: Figure 10 Page 19 of 45 Fig. 11: Figure 11 Page 20 of 45 Fig. 12: Figure 12 Page 21 of 45 Fig. 13: Figure 13 Page 22 of 45 Fig. 14: Figure 14 Page 23 of 45 Fig. 15: Figure 15 Page 24 of 45 Fig. 16: Figure 16 Page 25 of 45 Fig. 17: Figure 17 Page 26 of 45 Fig. 18: Figure 18 Page 27 of 45 Fig. 19: Figure 19 Page 28 of 45 Fig. 20: Figure 20 Page 29 of 45 Fig. 21: Figure 21 Page 30 of 45 Fig. 22: Figure 22 Page 31 of 45 Fig. 23: Figurte 23 Page 32 of 45 Fig. 24: Figure 24 Page 33 of 45 Fig. 25: Figure 25 Page 34 of 45 Fig. 26: Figure 26 Page 35 of 45 Fig. 27: Figure 27 Page 36 of 45 Fig. 28: Figure 28 Page 37 of 45 Fig. 29: Figure 29 Page 38 of 45 Fig. 30: Figure 30 Page 39 of 45 Fig. 31: Figure 31 Page 40 of 45 Fig. 32: Figure 32 Page 41 of 45 Fig. 33: Figure 33 Page 42 of 45 Fig. 34: Figure 34 Page 43 of 45 Conclusion • Diffusion tensor imaging and tractography are a key tool in the anatomical study of white matter fibers and projection, association and commissural fibers that improves conventional magnetic resonance imaging. • Diffusion tensor imaging is able to show abnormalities in a wide variety of diseases such as developmental disorders or psychiatric disorders and is specially useful in the assessment of ischemic disease, multiple sclerosis and tumors. • The use of tensor imaging in conjunction with functional studies (motor, visual, speech or memory), cortical mapping and intraoperative stimulation is a promising trend that helps prevent surgical neural damage. Personal Information Dr. Manuel Recio Rodríguez. Hospital Quirón Madrid. [email protected] References 1. Wakana S, Jiang H, Nagae-Postscher LM et al. Fiber Tract-based Atlas of Human White MatterAnatomy. Radiology.2004; 230:77-87. 2. Jellison BJ, Field AS, Medow J et al.Diffusion Tensor Imaging of Cerebral White Matter: A Pictorial Review of Physics, FiberTract Anatomy, and Tumor Imaging Patterns AJNR.2004;25:356-369. 3. Nucifora PG, Verma R, Lee SK et al. Diffusion-Tensor MR Imaging and Tractography: Exploring Brain Microstructure and Connectivity.Radiology.245;2:367-384. 4. Duque A, Roa E,CastedoJ. White matter anatomy using tensor diffusion tractography.Radiologia.2008;50(2):99-111. 5. Tha KK, Terae S, Yabe I, et al. Microstructural white matter abnormalities of multiple system atrophy: in vivo topographic illustration by using diffusion-tensor MR imaging. Radiology.2010;255(2):563-9. Page 44 of 45 6. Saito Y, Nobuhara K, Okugawa G, et al. Corpus callosum in patients with obsessivecompulsive disorder: diffusion-tensor imaging study. Radiology.;246(2):536-42. 7. Quiu D, Tan LH, Zhou K , et al.Diffusion tensor imaging of normal white matter maturation from late childhood to young adulthood: voxel-wise evaluation of mean diffusivity, fractional anisotropy, radial and axial diffusivities, and correlation with reading development. Neuroimage. 2008;41(2):223-32. 8. SachM, Winkler G, Glauche V, et al. Diffusion tensor MRI of early upper motor neuron involvement in amyotrophic lateral sclerosis. Brain 2004;127:340-350. 9. KearlySM, Kim YJ, Whiting WL, et al. Determination of Multiple Sclerosis Plaque Size with Diffusion-Tensor MR Imaging: Comparison Study with Healthy Volunteers. Radiology. 2008, 249, 955-963. 10. Anjari M, Srinivasan L, Allsop JM, et al. Diffusion tensor imaging with tractbasedspatial statistics reveals local white matter abnormalities in preterminfants. Neuroimage 2007;35:1021-27 11. Rose SE, Hatzigeorgiou X, StrudwickMW,et al. Altered white matter diffusion anisotropy in normal and preterm infants at term-equivalent age. Magn Reson Med 2008;60:761-67 Page 45 of 45