Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
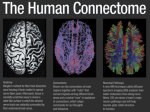
OBSERVATION Agenesis of the Arcuate Fasciculi in Congenital Bilateral Perisylvian Syndrome A Diffusion Tensor Imaging and Tractography Study Byron Bernal, MD; Gustavo Rey, PhD; Catalina Dunoyer, MD; Harshad Shanbhag, MS; Nolan Altman, MD Objective: To describe the absence of the arcuate fasciculi in 2 cases of congenital bilateral perisylvian syndrome (CBPS). Main Outcome Measures: Neuropsychology evaluation; fractional anisotropy, apparent diffusion coefficients, and anatomical aspect of the tracts. Design: Case series. Results: Absence of the arcuate fasciculus was observed in both subjects. Ancillary findings were complete absence of the superior longitudinal fasciculi in 1 case and underdevelopment in the other. Low fractional anisotropy of the left inferior occipitofrontal fasciculus was found in both cases. The same tract was maloriented in 1 of the cases. Setting: Pediatric referral hospital–based study. Patients: Two patients with CBPS, referred to our institution as candidates for surgical treatment of epilepsy. Intervention: Diffusion tensor imaging (1.5-T scanner; 15 encoding directions; b = 800 s/mm2) and deterministic tractography of the main projection and association tracts. T Author Affiliations: Miami Children’s Hospital (Drs Bernal, Rey, Dunoyer, and Altman and Mr Shanbhag) and MCH Brain Institute (Drs Bernal, Rey, and Dunoyer), Miami, Florida. Conclusion: Agenesis of the arcuate fasciculus may accompany CBPS. Arch Neurol. 2010;67(4):501-505 HE CONGENITAL BILATERAL perisylvian syndrome (CBPS) is a type of cortical developmental abnormality characterized by poor operculation of the parietal and frontal lobes, wide lateral sulcus, polymicrogyria, orofacial diplegia, epilepsy, and developmental delay.1,2 Seizures are present in 65% of cases.3,4 To our knowledge, CBPS has not been studied to date with diffusion tensor imaging and fiber tractography. We describe 2 cases with absence of the arcuate fasciculus (as part of agenesis or hypoplasia of the superior longitudinal fasciculus) in CBPS using diffusion tensor imaging and fiber tractography in relation to clinical and neuropsychological findings. To our knowledge, there are no existing reports describing bilateral agenesis of the arcuate fasciculus in this condition. The correlation of this finding with the clinical analysis of the language/ (REPRINTED) ARCH NEUROL / VOL 67 (NO. 4), APR 2010 501 speech deficit may contribute to the understanding of the arcuate fasciculus function. REPORT OF CASES The clinical and neuroradiological findings of 2 cases with CBPS are summarized in the Table. Case 2 has no arcuate fasciculus but has the remnant fibers of the superior longitudinal fasciculus. Normally, the superior longitudinal fasciculus has, in addition to the arcuate fasciculus, a bundle of short fibers connecting the parietal areas (supramarginal gyrus) with frontal areas. In addition, the fractional anisotropy of the left inferior occipitofrontal fasciculus was found to be low in both cases and bilaterally in the cingulum of case 2. A single-shot, spin-echo, echo-planar imaging sequence with diffusion weighting consisting of 15 encoding directions was WWW.ARCHNEUROL.COM ©2010 American Medical Association. All rights reserved. Downloaded From: https://archneur.jamanetwork.com/ on 05/14/2017 Table. Report of Cases Age, y Sex Handedness Main diagnosis Onset of seizures, y Type of seizure General developmental milestones Language developmental milestones Neuropsychology evaluation Overall intellectual functioning Language Prosody Articulatory skills Conduit d’approache c Automatic series Automatic series backward Phonemic fluency Semantic fluency Verbal memory Case 1 13 F Right Intractable epilepsy; CBPS 3 Right side head and eye version Motor: normal; poor attention; deficit executive functions Speech severely delayed; poor language comprehension Moderate to severe impaired range (IQ = 41; VCI score=55; PRI score= 49; WMI score = 50; PSI score=50) a Mildly impaired (IQ = 64; VCI score = 82; POI score=67) b Poor Poor None Normal Normal Severely impaired (standard score ⬍40) d Borderline (standard score = 71) Poor, with relatively preserved delayed recall Poor Poor None (not described) Normal Unable Moderately impaired (standard score = 52) Moderately impaired (standard score = 54) Borderline (scale score = 5) e; good delayed recall (scale score = 6) e Borderline (scale score = 6) b Impaired (scale score = 4) b Borderline (scale score = 5) f; very poor graphomotor skills (VMI standard score = 45) Impaired (digit span, scale score = 3) b Moderately impaired (raw score = 7) g; better for delayed recall (raw score = 10) g Impaired (PSI standard score = 57) Severely impaired: RH standard score ⬍40; LH standard score ⱕ40 h “Multiple cognitive domains impairment with a trend of greater dysfunction of the nondominant hemisphere [with] preserved mesiotemporal regions” Interictal: bilateral temporal spikes and right temporal slow waves; ictal: bilateral centrotemporal sharp slow waves more prominent in the right side Bilaterally poorly formed operculum; cortical thickening, polymicrogyria in opercular and hippocampal regions (Figure 1B); left cerebellar aplasia Color-coded FA map: small and poorly defined SLFs (Figure 5); fiber tractography: absence of the arcuate fibers (Figure 6) Left IOFF: 0.38 i/0.85 Right IOFF: 0.46/0.86 Left ILF and IOFF: 0.47/0.94 Right ILF and IOFF: 0.52/0.90 Left cingulum: 0.39 i/0.82 Right cingulum: 0.35 i/0.81 Left internal capsule: 0.53/0.78 Right internal capsule: 0.51/0.82 Verbal reasoning Nonverbal reasoning Constructional praxis Severely impaired (scale score = 3) a Severely impaired (scale score = 1) a Poor (VMI standard score = 61; scale score = 1) a Auditory working memory Memory for faces Severely impaired (digit span, scale score = 1) a Borderline (scale score= 6) g; normal delayed recall (scale score=9) g Severely impaired (PSI standard score ⬍40) Severely impaired bilaterally: RH standard score ⬍40; LH standard score=unable to perform h “Diffuse cerebral dysfunction, with relatively preserved performance on measures associated with mesiotemporal systems” Interictal: right frontotemporal slowing; ictal: bilateral central epileptiform activity Visual psychomotor speed Fine motor dexterity Neuropsychological global profile EEG MRI DTI/tractography Other associative tracts (FA/ADC) Case 2 18 M Right Intractable epilepsy; CBPS 12 Right side head version, staring, jaw movements Motor: normal, but with sucking and swallowing problems as infant Speech severely delayed; poor language comprehension Bilateral opercular cortical malformation; thick cortex, small gyri, abnormal sulcation (Figure 1A); left cerebellum hypoplasia Color-coded FA map: failure to demonstrate the SLF bilaterally (Figure 4); bilateral abnormal IOFF orientation (curved upward); lack of cerebellar fibers Left IOFF: 0.33 i/0.88 Right IOFF: 0.53/0.81 Left ILF and IOFF: 0.48/0.84 Right ILF and IOFF: 0.47/0.89 Left cingulum: 0.44/0.76 Right cingulum: 0.40/0.80 Left internal capsule: 0.61/0.80 Right internal capsule: 0.55/0.82 Abbreviations: ADC, apparent diffusion coefficients; CBPS, congenital bilateral perisylvian syndrome; DTI, diffusion tensor imaging; EEG, electroencephalography; FA, fractional anisotropy; IOFF, inferior occipitofrontal fasciculus; ILF, inferior longitudinal fasciculus; LH, left hand; MRI, magnetic resonance imaging; POI, Perceptual Organization Index; PRI, Perceptual Reasoning Index; PSI, Processing Speed Index; RH, right hand; SLF, superior longitudinal fasciculus; VCI, Verbal Comprehension Index; VMI, Beery-Buktenica Developmental Test of Visual-Motor Integration; WMI, Working Memory Index. a Wechsler Intelligence Scale for Children–Fourth Edition Spanish Version. b Wechsler Adult Intelligence Scale–Third Edition Full-Scale IQ. c Conscious effort to correct mispronunciations. d Multilingual Aphasia Examination Spanish Version. e Wide Range Assessment of Memory and Learning, Second Edition. f Wechsler Adult Intelligence Scale–Third Edition Block Design. g NEPSY Memory for Faces subtest. h Grooved Pegboard Test. i Values lower than normal range accordingly with in-house standardization. (REPRINTED) ARCH NEUROL / VOL 67 (NO. 4), APR 2010 502 WWW.ARCHNEUROL.COM ©2010 American Medical Association. All rights reserved. Downloaded From: https://archneur.jamanetwork.com/ on 05/14/2017 A B A P Figure 1. T1-weighted axial magnetic resonance images showing main findings of congenital bilateral perisylvian syndrome. A, Case 1. B, Case 2. Notice the distinctive widening of the sylvian fissure with “exposure” of the insula to the cortical surface and abnormal sulcation. A P Figure 2. Normal appearance of the superior longitudinal fasciculus (arrows) in a normal volunteer defined at this level as triangular green shapes lateral to the blue descending fibers of the corticospinal tract. Figure 3. Normal appearance of the superior longitudinal fasciculi and the arcuate fasciculi in a normal volunteer. The superior longitudinal fasciculi (double thin arrows), conformed by parietal fibers (arrowheads), and the arcuate fasciculi (long single arrows). The superior longitudinal fasciculi on the right side does not carry arcuate fibers. Red indicates left side; yellow, right side; A, anterior; P, posterior. COMMENT performed in a 1.5-T scanner (Figure 1). A diffusion weighting (b) of 800 s/mm2 was used. Fractional anisotropy and tractography was performed using VolumeOne software (http://www.volume-one.org/). The superior longitudinal fasciculus containing the arcuate fasciculus fibers was sought in a coronal plane at the level of the rostral aspect of the splenium. The tract appears normally as a green triangle lateral to the blue descending fibers of the corticospinal tracts (Figure 2), from where the arcuate fasciculus can be tracked (Figure 3). This area was contoured bilaterally defining the seeding region of interest (ROI). Tract propagation was terminated when the tract trajectory reached a voxel with fractional anisotropy less than 0.13 or when the angle between 2 consecutive steps was greater than 45°. Fractional anisotropy and apparent diffusion coefficients values were obtained from the inferior occipitofrontal fasciculi, cingulum (single coronal ROIs at the level of the anterior commissure), the inferior longitudinal fasciculi in conjunction with the inferior occipitofrontal fasciculi (single coronal ROI at the level of the retrosplenial surface), and the internal capsules (single axial ROI at the level of the thalamus) (Figures 4, 5, and 6). The superior longitudinal fasciculus consists mainly of the long curved fibers with posterior end points in the temporal cortex and a bundle of rather horizontal fibers whose posterior end points are located in the parietal lobe (Figure 3). The curved fibers correspond to the arcuate fasciculus, a tract considered crucial for the communication between receptive and expressive language brain areas.5-7 Lesions of the arcuate fasciculus result in a deficiency in the capacity to repeat, a syndrome that has been coined “conduction aphasia.” Other authors have proposed that the arcuate fasciculus also plays a role in intelligence8 and nonlanguage cognitive functions.9 The absence of the arcuate fasciculus in our 2 cases provides an opportunity to look into its role. We were more concerned in what has been preserved as opposed to the deficit, since our cases have many other cortical abnormalities that could be the cause of any cognitive or motor deficiency. Looking at what has been preserved gives us an idea of what the arcuate fasciculus is not involved in. Automatized language (eg, reciting automatic series) and delayed recall of verbal and nonverbal material was (REPRINTED) ARCH NEUROL / VOL 67 (NO. 4), APR 2010 503 WWW.ARCHNEUROL.COM ©2010 American Medical Association. All rights reserved. Downloaded From: https://archneur.jamanetwork.com/ on 05/14/2017 A P Figure 6. Tractography of the superior longitudinal fasciculi in case 2. The tracts are color coded for laterality: red, left; yellow, right. Notice the absence of the arcuate fasciculus component in both sides. A indicates anterior; P, posterior. Figure 4. Fractional anisotropy and color-coded directional map of case 1.The coronal cut location is similar to the one used for Figure 2. Notice the absence of the green anteroposterior bundle lateral to the blue corticospinal tract that defines the superior longitudinal fasciculus. Arrows point to the estimated location they should appear. Figure 5. Fractional anisotropy and color-coded directional map of case 2. Rudimentary superior longitudinal fasciculi are observed in both sides (arrows). preserved in both patients. Strikingly, no report of conduction aphasia was mentioned. Therefore, at least for these 2 patients, the arcuate fasciculus was not needed for these functions. The common clinical findings in these cases with arcuate fasciculus agenesis were delayed speech development with poor articulation and poor prosody and other aspects of speech. In addition, both patients showed poor phonemic and semantic word generation, and difficulties in visuospatial, organization/assembly skills, that may prompt a diagnosis of constructional apraxia. The idea to attribute the phonological difficulties of our patients merely to the arcuate fasciculus absence seems supported by a recent report of intraoperative electrophysiological studies that have shown the arcuate fasciculus transmits phonological cues.10,11 However, concomitant cortical and connectivity findings confound this observation. The role of the arcuate fasciculus (and the entire superior longitudinal fasciculus) in speech and language is not completely understood. Normal volunteers show a longer left arcuate fasciculus, with more fibers, and higher fractional anisotropy values. Moreover, in many cases, the right arcuate fasciculus is nonexistent.12-14 Strikingly, left arcuate fasciculus dominance has been reported in subjects with right hemisphere language dominance.15 More recently, lateralization of the arcuate fasciculus has been found correlated with the lateralization index of language determined by functional magnetic resonance imaging on patients with right but not left temporal lobe epilepsy.16 We present for the first time, to our knowledge, 2 cases of CBPS with bilateral absence of the arcuate fasciculi. This finding analyzed in the context of the associated clinical findings may help to understand the clinical presentation of the condition and further expose language organization. Accepted for Publication: June 30, 2009. Correspondence: Byron Bernal, MD, 3100 SW 62nd Ave, Miami, FL 33176 ([email protected]). Author Contributions: Study concept and design: Bernal. Acquisition of data: Bernal, Rey, Dunoyer, and Shanbhag. Analysis and interpretation of data: Bernal, Rey, and Altman. Drafting of the manuscript: Bernal, Rey, and Dunoyer. Critical revision of the manuscript for important intellectual content: Bernal, Rey, Shanbhag, and Altman. Administrative, technical, and material support: Dunoyer. Study supervision: Bernal, Rey, and Altman. Financial Disclosure: None reported. REFERENCES 1. Gropman AL, Barkovich AJ, Vezina LG, Conry JA, Dubovsky EC, Packer RJ. Pediatric congenital bilateral perisylvian syndrome: clinical and MRI features in 12 patients. Neuropediatrics. 1997;28(4):198-203. (REPRINTED) ARCH NEUROL / VOL 67 (NO. 4), APR 2010 504 WWW.ARCHNEUROL.COM ©2010 American Medical Association. All rights reserved. Downloaded From: https://archneur.jamanetwork.com/ on 05/14/2017 2. Kuzniecky R, Andermann F, Guerrini R. The epileptic spectrum in the congenital bilateral perisylvian syndrome: CBPS Multicenter Collaborative Study. Neurology. 1994;44(3, pt 1):379-385. 3. Guerrini R, Carrozzo R. Epileptogenic brain malformations: clinical presentation, malformative patterns and indications for genetic testing. Seizure. 2002; 11(suppl A):532-543. 4. Guerrini R. Genetic malformations of the cerebral cortex and epilepsy. Epilepsia. 2005;46(suppl 1):32-37. 5. Geschwind N. Disconnexion syndromes in animals and man: II. Brain. 1965;88 (3):585-644. 6. Geschwind N. The organization of language and the brain. Science. 1970;170(961): 940-944. 7. Wernicke C. The aphasic symptom complex: a psychological study on a neurological basis. Boston Stud Philos Sci. 1874:4. 8. Jung RE, Haier RJ. The Parieto-Frontal Integration Theory (P-FIT) of intelligence: converging neuroimaging evidence. Behav Brain Sci. 2007;30(2):135154. 9. Sundaram SK, Sivaswamy L, Makki MI, Behen ME, Chugani HT. Absence of arcuate fasciculus in children with global developmental delay of unknown etiology: a diffusion tensor imaging study. J Pediatr. 2008;152(2):250-255. 10. Mandonnet E, Nouet A, Gatignol P, Capelle L, Duffau H. Does the left inferior lon- 11. 12. 13. 14. 15. 16. gitudinal fasciculus play a role in language? a brain stimulation study. Brain. 2007; 130(pt 3):623-629. Duffau H, Peggy Gatignol ST, Mandonnet E, Capelle L, Taillandier L. Intraoperative subcortical stimulation mapping of language pathways in a consecutive series of 115 patients with grade II glioma in the left dominant hemisphere. J Neurosurg. 2008;109(3):461-471. Powell HW, Parker GJ, Alexander DC, et al. Hemispheric asymmetries in languagerelated pathways: a combined functional MRI and tractography study. Neuroimage. 2006;32(1):388-399. Nucifora PG, Verma R, Melhem ER, Gur RE, Gur RC. Leftward asymmetry in relative fiber density of the arcuate fasciculus. Neuroreport. 2005;16(8):791-794. Parker GJ, Luzzi S, Alexander DC, Wheeler-Kingshott CA, Ciccarelli O, Lambon Ralph MA. Lateralization of ventral and dorsal auditory-language pathways in the human brain. Neuroimage. 2005;24(3):656-666. Vernooij MW, Smits M, Wielopolski PA, Houston GC, Krestin GP, van der Lugt A. Fiber density asymmetry of the arcuate fasciculus in relation to functional hemispheric language lateralization in both right- and left-handed healthy subjects: a combined fMRI and DTI study. Neuroimage. 2007;35(3):1064-1076. Rodrigo S, Oppenheim C, Chassoux F, et al. Language lateralization in temporal lobe epilepsy using functional MRI and probabilistic tractography. Epilepsia. 2008; 49(8):1367-1376. Announcement Visit www.archneurol.com. As an individual subscriber, you may elect to be contacted when a specific article is cited. Receive an e-mail alert when the article you are viewing is cited by any of the journals hosted by HighWire. You will be asked to enter the volume, issue, and page number of the article you wish to track. Your e-mail address will be shared with other journals in this feature; other journals’ privacy policies may differ from JAMA & Archives Journals. You may also sign up to receive an e-mail alert when articles on particular topics are published. (REPRINTED) ARCH NEUROL / VOL 67 (NO. 4), APR 2010 505 WWW.ARCHNEUROL.COM ©2010 American Medical Association. All rights reserved. Downloaded From: https://archneur.jamanetwork.com/ on 05/14/2017