Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Biochemical cascade wikipedia , lookup
Radical (chemistry) wikipedia , lookup
Signal transduction wikipedia , lookup
Western blot wikipedia , lookup
Photosynthesis wikipedia , lookup
Basal metabolic rate wikipedia , lookup
Gaseous signaling molecules wikipedia , lookup
Microbial metabolism wikipedia , lookup
Metalloprotein wikipedia , lookup
Adenosine triphosphate wikipedia , lookup
Evolution of metal ions in biological systems wikipedia , lookup
Light-dependent reactions wikipedia , lookup
Biochemistry wikipedia , lookup
Citric acid cycle wikipedia , lookup
Photosynthetic reaction centre wikipedia , lookup
Electron transport chain wikipedia , lookup
NADH:ubiquinone oxidoreductase (H+-translocating) wikipedia , lookup
Mitochondrion wikipedia , lookup
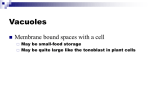
13 January 2011 No. 2 Bioenergetic Failure: Mitochondrial Catastrophe or Survival Coup Colin Mitchell Commentator:S. Kassie Moderator:N. Kalafatis Department of Anaesthetics CONTENTS INTRODUCTION ................................................................................................... 3 SEPSIS RELATED ORGAN DYSFUNCTION ....................................................... 3 THE MITOCHONDRION ....................................................................................... 5 CELLULAR RESPIRATION – ATP PRODUCTION .............................................. 7 Glycolysis ......................................................................................................... 8 Citric Acid Cycle (Krebs Cycle) ....................................................................... 8 Oxidative Phosphorylation .............................................................................. 9 MITOCHONDRIAL INJURY IN SEPSIS ............................................................. 12 Genetic Predisposition .................................................................................. 13 Endocrine Alterations .................................................................................... 13 DO2:VO2 Balance ............................................................................................. 14 Oxidative Stress ............................................................................................. 14 Reactive Oxygen Species ....................................................................................... 14 Reactive Nitrogen Species ..................................................................................... 15 Endogenous Antioxidant Protection ..................................................................... 16 Oxidative Stress Induced Mitochondrial Damage ................................................ 16 MITOCHONDRIAL CATASTROPHE HYPOTHESIS .......................................... 18 BIOENERGETIC FAILURE................................................................................. 19 TREATMENT STRATEGIES .............................................................................. 20 The prevention and reversal of early mitochondrial dysfunction ............... 20 The prevention of energetic failure once mitochondrial dysfunction is established...................................................................................................... 22 The resolution of the mitochondrial dysfunction ......................................... 23 CONCLUSION .................................................................................................... 24 APPENDIX A – NOVEL ANTIOXIDANT THERAPIES ........................................ 25 REFERENCES.................................................................................................... 28 Page 2 of 31 INTRODUCTION Sepsis is the systemic inflammatory response to a confirmed or suspected infection.50 In the critically ill patient, it is the most common cause of both morbidity and mortality. In uncomplicated sepsis, mortality may reach 25% and in patients who develop organ failure this may increase up to 80%.1 Despite ongoing research and an increase in the understanding of sepsis-related pathophysiology as well as the development of novel approaches and treatments to deal with sepsis, the deterioration in the function of various organs – the Multiple Organ Dysfunction Syndrome (MODS) remains the most common cause of Intensive Care Unit (ICU) mortality.1 For some time, the accepted aetiology of sepsis-induced organ dysfunction centred on the role of the inflammatory response and the associated impairment in vascular control, specifically in the micro circulation. It was felt that this would result in impaired delivery of oxygen and other substrates to the tissues resulting in progressive organ dysfunction, failure and ultimately death.25 The organs most commonly affected are the lungs, kidneys and liver and whilst the clinical manifestations including arterial hypoxaemia, azotaemia and cholestatic jaundice may be quite profound, on a histopathological level, fatal sepsis is often much less dramatic. Histological specimens of the affected tissue most commonly only demonstrate areas of focal necrosis or apoptosis and only very rarely is there the massive loss of parenchymal tissue that might be expected as a result of hypoperfusion or tissue anoxia.2 SEPSIS RELATED ORGAN DYSFUNCTION The pathophysiology behind MODS is most certainly multifactorial with systemic inflammation and its associated impairment in vascular and microcirculatory control playing a central role especially in the earlier stages of the disease. They are, however, unable to fully explain the full pathophysiology of this disease process on their own. Ninety years ago Barcroft proposed the mechanisms behind the three classic causes of cellular hypoxia: low arterial oxygen tension (hypoxaemic hypoxia), low circulating haemoglobin concentrations (anaemic hypoxia) and microvasular hypoperfusion (stagnant hypoxia).3 In sepsis each of these mechanisms is potentially occurring either in isolation or more commonly in combination. The factors to ensure adequate oxygen delivery to the tissues are well described by the Oxygen Flux Equation and, through manipulation of PaO2, haemoglobin concentration and cardiac output; it attempts to address the contributors to cellular hypoxia. Page 3 of 31 DO2 = CO x ([Hb] x 1.34g/dl x SaO2 ) + (PaO2 x 0.003) DO2 – Tissue Oxygen Delivery, CO – Cardiac Output, Hb – Haemoglobin (g/dl), SaO2 – Arterial Haemoglobin Saturation, PaO2 – Arterial Partial Pressure of Oxygen (mmHg) However, the well-described observation that MODS is often associated with accelerated anaerobic metabolism despite a supranormal systemic oxygen delivery adds weight to the concept of an additional intrinsic derangement in cellular energy metabolism. This phenomenon has been termed cytopathic hypoxia. And while it has been well described with certain drug toxicities and poisonings, classically cyanide poisoning, there has now been a resurgence in the plausibility of the concept that sepsis-related organ dysfunction may be at least in part be due to a ‘bioenergetic failure’ as a result of mitochondrial dysfunction.4 Other observations in support of this theory include the progressive decrease in total body oxygen consumption as the severity of the sepsis increases,5 tissue oxygen tension measurements are elevated in sepsis but will normalise during recovery6 and the ability of organs with limited reservation ability (such as the kidney) to fully recover to such an extent that organ support may not be required. The debate between the relative contributions of microvascular dysfunction and bioenergetic failure could possibly be explained by a single theory. Shunting in the microvasculature will result in regional tissue hypoxia together with decreased ATP production. In addition further mitochondrial dysfunction (from oxidative stress, decreased expression of mitochondrial proteins and hormonal alterations) may result in an energy demand versus supply imbalance. Should this imbalance continue to a point at which ATP concentrations will fall below a critical level, the cellular death pathways are initiated. This means a combination of shunting and decreased mitochondrial oxygen utilisation may be responsible for the increased venous oxygen saturations seen in resuscitated sepsis. The high oxygen content in tissue beds may be explained by a reduction in metabolic activity in an attempt to match the reduced energy supply (as a result of decreased oxygen delivery or mitochondrial dysfunction).7 Page 4 of 31 THE MITOCHONDRION The mitochondrion is an intracellular organelle that is found in almost all eukaryotic cells. It ranges in size from 0.5 to 10 µm and is enclosed by a double membrane. Unlike other cellular organelles, it possesses its own DNA and it has been postulated that they may once have been free living organisms or developed from endosymbiotic proteobacteria.8 More than 90% of the body’s oxygen utilisation is by the mitochondria in the process of energy production.8 1-inner membrane 2-outer membrane 3-cristae 4-matrix Fig 1: The Mitochondrion9 Mitochondrial Structure The mitochondria consist of a number of different compartments each of which will carry out a number of specific functions. I. The Outer Membrane This is a phospholipid bilayer which is similar in structure to the plasma membrane. It contains transmembranous proteins or porins that form channels to allow for the passive diffusion of small molecules (<5 kD) across the membrane. There is a potential difference across the membrane of approximately 150 to -180mV with respect to the outside. This is formed as a result of proton movement associated with the electron transfer chain. The importance of this electrical gradient is also important for some of the new therapies in which drug delivery is targeted directly to the mitochondrion as discussed later. II. The Intermembranous Space This space is located between the outer and inner membranes. As a result of the relative permeability of the outer membrane to small molecules, it has the same ionic concentrations as the cytosol. Page 5 of 31 Large proteins, on the other hand, require specific transport mechanisms to enter or leave this compartment and as such the protein content will be different from that of the cytosol. Cytochrome C, an essential component of the electron transfer chain, is a protein that under normal conditions is localised to the intermembranous compartment. Disruption of the outer membrane for any reason, will allow leakage of this protein into the cytosol, and is one of the triggers which will result in apoptosis (programmed cell death).10 III. The Inner Membrane This is also a phospholipid bilayer, but with a protein to phospholipid ratio of 3:1 by weight (cf. a ratio of 1:1 in the plasma membrane) i.e. it is highly protein dense. It contains a specific phospholipid, cardiolipin, which is characteristic of mitochondrial and bacterial plasma membranes. It does not contain porins and this results in the inner membrane being totally impermeable to all molecules. Any substance required to enter or leave the mitochondrial matrix therefore requires a specific membrane transporter. The inner membrane contains proteins that will perform one of five specific functions, namely: i. The reduction-oxidation (REDOX) reactions of oxidative phosphorylation ii. ATP Synthase which generates ATP in the matrix iii. Transport proteins that allow passage of molecules into and out of the matrix iv. Protein assembly units v. Fusion and fission proteins IV. Cristae The inner membrane is highly convoluted, which allows for a greater surface area for the production of ATP. Mitochondria in cells with a greater demand for ATP will have more cristae (e.g. hepatic mitochondria may have an inner surface area in excess of 5 times that of the outer membrane) V. Matrix This is the space enclosed by the inner membrane and, together with the membrane- bound ATP Synthase, is the site of ATP production. It also contains the enzymes responsible for the citric acid cycle and lipid oxidisation together with mitochondrial ribosomes, transport RNA and the mitochondrial DNA. Page 6 of 31 VI. Mitochondrial DNA (mtDNA) The mitochondrion has its own genetic material as well as the capability to manufacture its own RNA and proteins. mtDNA has a remarkable similarity to bacterial genomes. Mitochondrial Function The mitochondria are responsible for a wide variety of functions which include 33: Regulation of the cell membrane potential Apoptosis Calcium homeostasis The regulation of cellular proliferation Regulation of cellular metabolism Certain haem synthesis reactions Steroid synthesis However, the mitochondrion is best known for and classically described as being the ‘Powerhouse’ of the cell. This is due to one of its most prominent functionsthat being the production of Adenosine Triphosphate (ATP) which is the primary source of cellular chemical energy. In fact, gram for gram, a mitochondrion generates more energy than the sun. CELLULAR RESPIRATION – ATP PRODUCTION Cellular respiration is the metabolic process that take place within cells in order to convert the biochemical energy found in nutrients (glucose, fatty acids and amino acids) into an energy source that can be used by the cell, namely ATP. These metabolic reactions are catabolic in nature and involve reduction-oxidation (REDOX), with molecular oxygen being the most common oxidising agent under conditions of aerobic metabolism. By accepting electrons, the oxygen itself is being reduced, but it is causing the oxidisation of something else. Cellular respiration is algebraically summarised by the equation: C6H12O6 + 6O2 → 6CO2 + 6H2O + 38ATP In reality, the actual energy yield is in the region of 30 to 32 molecules of ATP per mole of glucose. Cellular respiration consists of three interdependent pathways: Page 7 of 31 Glycolysis Glycolysis is a metabolic process that occurs within the cytoplasm. It involves the conversion of one molecule of glucose into two molecules of pyruvate. It can also occur under anaerobic conditions with a net production of 2 molecules of ATP (4 ATP molecules produced with 2 consumed), as well as 2 molecules of the reduced electron carrier, Nicotinamide Adenine Dinucleotide (NADH). NADH is utilised later to generate ATP during the process of oxidative phosphorylation. Glucose + 2NAD+ + 2Pi + 2ADP → 2Pyruvate + 2NADH + 2ATP + 2H+ + 2H2O Fig 2: The Glycolytic Pathway9 In the presence of oxygen, the pyruvate is transported into the mitochondrion where it is oxidised to the 2-carbon compound, Acetyl CoA. This results in the generation of one molecule of CO2 and one molecule of NADH. In the absence of oxygen, pyruvate fermentation occurs resulting in the formation of waste products including lactate, in skeletal muscle. Citric Acid Cycle (Krebs Cycle) Acetyl CoA will then enter the Citric Acid Cycle within the mitochondrial matrix. This is an 8 step process that utilises some 18 different enzymes. The net energy yield (per molecule of glucose i.e. 2 molecules of Acetyl CoA) is 6 NADH, 2 reduced Flavin Adenine Dinucleotide molecules (FADH2) and 2 ATP with the formation of two waste products, H2O and CO2. Page 8 of 31 Fig 3: The Citric Acid Cycle9 Oxidative Phosphorylation The final step of cellular respiration takes place on the mitochondrial cristae. Energy in the form of ATP is produced from a process that commences with the flow of electrons along 5 inner membrane-bound molecular complexes (a process known as the electron transfer chain). These electrons are generated by oxidising the NADH (and FADH2) produced by the citric acid cycle to NAD+ (and FAD). The subsequent transfer of electrons from complex to complex results in a reciprocal transfer of protons from the mitochondrial matrix into the intermembranous space. This generates the mitochondrial membrane potential that is then used to drive the phosphorylation of ADP by the enzyme ATP synthase, which will result in the formation of ATP. Since this process is potentially the origin of mitochondrial dysfunction, we will look at it in some detail. Page 9 of 31 Fig 4: Schematic Representation of Oxidative Phosphorylation in theMitochondrion.8 Complex I (NADH Dehydrogenase) This is a large enzyme that catalyses the 2 electron reduction of coenzyme Q10 (ubiquinone) to QH2 (ubiquinol) by NADH. The net result of this electron transfer is 4 protons being pumped from the mitochondrial matrix into the intermembranous space. Complex I has been found to be a potent source of superoxide free radicals.11 Page 10 of 31 Fig 5: Complex I (NADH Dehydrogenase)9 Complex II (Succinate Dehydrogenase) This is the only enzyme found in both the electron transfer chain and the citric acid cycle. It oxidises succinate to fumarate and in so doing, also reduces coenzyme Q10 to QH2. This reaction releases less energy that the Complex I oxidisation of NADH and as a result it does not result in proton transport across the membrane. Complex III (Cytochrome C Reductase) The reaction catalysed here is the oxidation of QH2 and the reduction of cytochrome C. This is a complex, two- step process and is the second important source of superoxide free radicals, which are formed via the production of the highly reactive free radical intermediate, ubisemiquinone (Q-). The net effect is 4 protons entering the intermembranous space Fig 5: Complex III (Cytochrome C Reductase)9 Page 11 of 31 Complex IV (Cytochrome c Oxidase) The final protein complex of the electron transfer chain pumps protons across the inner membrane whilst accepting electrons from the reduced cytochrome C onto the terminal electron acceptor, oxygen, which is subsequently reduced to water. . Fig 6: Complex IV (Cytochrome C Oxidase)9 Complex V (ATP Synthase) This protein, whilst not specifically involved in the electron transfer chain, is the final enzyme in the oxidative phosphorlyation pathway. It uses the energy from the proton electrochemical gradient across the inner membrane to drive the formation of ATP from ADP MITOCHONDRIAL INJURY IN SEPSIS There are a number of animal studies that have been able to demonstrate the presence of mitochondrial dysfunction in sepsis.12 Ultra-structural damage has been seen in the hepatic mitochondria of patients who have died as a result of sepsis.13 The depletion of endogenous antioxidants have been associated with mitochondrial dysfunction as well as related to the severity of organ failure and eventual outcome.14 As mitochondria utilise over 90% of the body’s oxygen consumption in the process of ATP production, any abnormalities in oxygen consumption are therefore likely to be as a result of mitochondrial dysfunction. In sepsis there are a number of potential causes for mitochondrial dysfunction. These may include genetic predisposition and down-regulation of mitochondrial protein synthesis, the associated endocrine changes, imbalances between oxygen supply (DO2) and oxygen uptake (VO2)as well as the ubiquitous role of Oxidative Stress. Page 12 of 31 Genetic Predisposition Many studies have demonstrated various genetic polymorphisms that are linked to outcomes in sepsis including increased activation of Nuclear Factor κβ (NF-κβ) which is responsible for regulating many of the proinflammatory mediators. As a result, genetic associations with enhanced NF-κβ activation are associated with poor outcomes.15 There is also evidence that sepsis may result in a decreased synthesis of new mitochondrial proteins, specifically decreased expression of the respiratory chain complex and ATP synthetase genes.16 Endocrine Alterations Following the initial stress response associated with an inflammatory insult, sepsis is associated with adrenal insufficiency, the sick euthyroid syndrome, insulin resistance and hypogonadism.8 Mitochondria have receptors for both adrenocortical and thyroid hormones, with the thyroid being a key modulator of mitochondrial function.27 Hyperthyroidism increases ATP production at the expense of reduced efficiency of production with the opposite being true of hypothyroidism. The ‘sick euthyroid syndrome’ seen in sepsis is associated with a decreased, although more efficient, cellular respiration.27 The effects of corticosteroids on the mitochondria appear to depend on duration of exposure to steroids. Acute stress increases complex IV activity (in a rat model),17 However hypercortisolaemia associated with chronic intermittent stress has resulted in a decrease in mitochondrial functioning.27 Insulin resistance and the associated hyperglycaemia than occurs in septic patients may also contribute to mitochondrial dysfunction through the absence of the permissive effects of insulin on mitochondrial protein synthesis and cellular respiration. The associated hyperglycaemia may also result in the increased production of reactive oxygen species (ROS). This may contribute towards the improved outcomes in critical care patients who have been rendered normoglycaemic with insulin therapy.13 Circulating Leptin, a hormone secreted by adipose tissue involved in the regulation of food intake and energy balance, has been shown to be decreased in non-survivors when compared to survivors.18 The administration of exogenous leptin to diabetic rats has been shown to increase mitochondrial proliferation in white adipose cells.19 A similar effect has been demonstrated by administering oestrogen following trauma haemorrhage which resulted in an increase in mitochondrial protein production, enzyme activity and ATP levels when compared to a control.20 Page 13 of 31 DO2:VO2 Balance Much has been written about the importance of the re-establishment of tissue perfusion and oxygen delivery specifically in the early stages of sepsis. The optimisation of the contributors to tissue oxygen delivery, namely cardiac output, haemoglobin levels and PaO2, remain central to the management of sepsis. Conceptually sepsis may be considered in two distinct phases. Early sepsis (shutdown phase) at which stage the mitochondria have not yet been damaged and resuscitation, in an attempt to re-establish organ perfusion, has been demonstrated to have improved outcomes.21 The stage of late sepsis is characterised by established mitochondrial damage and attempts at aggressive resuscitation at this stage have been shown to have adverse outcomes.27 This opens the door to looking at possible treatment options that may decrease the body’s energy requirements, thereby decreasing VO2, in an attempt to conserve cellular function and energy. Oxidative Stress 33 Reactive Oxygen Species ROS are chemically active substances that contain oxygen. They also include molecules with an unpaired electron (the so-called free radicals) which includes the superoxide anion, as well as strong oxidizing agents such as hydrogen peroxide. Whilst ROS can be formed by exogenous sources such as ionising radiation, they are also naturally-occurring by-products of oxidative phosphorylation formed as a result of the incomplete reduction of oxygen to water. As molecular oxygen is such a strong oxidising agent (readily accepts electrons), its reduction does involve the production of these potentially harmful intermediates. As much as 1% of oxygen may be converted to ROS via a process known as electron leakage in which electrons are transferred directly to oxygen to form superoxide. O2 + e- → O2- + e- → O22O2- = Superoxide O22- = Peroxide ROS have important physiological roles to play in normal cell signalling and as such their production needs to be seen as important for cellular function and survival. Under normal circumstances ROS production is very tightly controlled by a number of endogenous antioxidants because, whilst short-lived, they are also highly reactive and have the potential to interact indiscriminately with surrounding molecules. Therefore, if not controlled, they can be extremely damaging to the same mitochondria in which they are produced. Page 14 of 31 This is a process known as Oxidative Stress and occurs whenever ROS production exceeds the capacity of the body’s regulatory systems. Oxidative stress has been known to contribute to a number of disease processes including Sickle Cell Disease, Alzheimer’s and Parkinson’s as well as the retinopathies and neuropathies cause by diabetes. There is also a well-defined association of the role of oxidative stress in cardiovascular disease. Specifically, oxidised Low Density Lipoprotein (LDL) appears to trigger atherogenesis which ultimately leads to atherosclerosis and ultimately cardiovascular disease.22 Reactive Nitrogen Species Oxidative phosphorylation can also result in the production of Nitric Oxide (NO-) which, by virtue of its unpaired electron, is also a free radical. The NO- in turn has the ability to form by-products known as Reactive Nitrogen Species (RNS). Peroxynitrite, a highly toxic RNS, is formed from the interaction between NO- and the superoxide anion (O2-). Under normal circumstances the superoxide anion would be rapidly converted into Hydrogen Peroxide (H2O2) and then to water by the endogenous antioxidant systems. However, in the presence of increased NO- , the reaction between the superoxide anion and NO- to form peroxynitrite occurs even more rapidly. It is this peroxynitrite that is thought to account for most of the cytotoxic effects of NO-. Nitric oxide is formed via the action of the enzyme Nitric Oxide Synthase (NOS) on L-Arginine. L-Arginine + NADPH + H+ + 2O2 NOS Citrulline + NO- + NADP+ There are a number of different isoforms of the NOS enzyme, including: 1. Neuronal NOS (nNOS or NOS-1), produced by neurons in the central and peripheral nervous systems and involved in cellular communication. 2. Endothelial NOS (eNOS or NOS-3), a constitutive form that is released by vascular endothelium and is involved in the regulation of vascular tone. 3. Inducible NOS (iNOS or NOS-2) is involved in the immune response. Activation by inflammatory mediators including Nuclear Factor κβ (NF κβ) will result in iNOS transcription and the production of large quantities of NO -. The induction of the high output iNOS often occurs in an oxidative environment and as such the high levels of NO- have the ability to interact with superoxide anion producing the toxic RNS peroxynitrite. This has a role in the killing abilities of the macrophage respiratory burst. 4. Whilst as yet unconfirmed, there is growing interest in the potential for there to be a mitochondrial form of NOS (mtNOS).23 This may further support the central role of mitochondrial dysfunction in sepsis. Page 15 of 31 Endogenous Antioxidant Protection ROS and RNS are naturally occurring by-products of oxidative phosphorylation and play an important role in a number of physiological processes within the mitochondria. These include calcium and iron homeostasis and certain cellsignalling pathways. They are also highly toxic and therefore have the potential to cause damage to surrounding molecules and organelles. It stands to reason that there must be some endogenous protective mechanism from these entities. Indeed, under normal circumstances their activity is tightly regulated by an interacting system of antioxidants. This includes the enzymatic pathways Manganese Superoxide Dismutase (MnSOD), Thioredoxin (TRX), Peroxiredoxins, Sulphiredoxins, Cytochrome C, Peroxidise and Catalase, as well as a number of non-enzymatic pathways, such as Glutathione (GSH), Ascorbic Acid (Vit. C), Tocopherol (Vit. E) and Uric Acid. As described earlier, an example of the intricate interaction between the various endogenous pathways is that of the superoxide anion. This ROS is formed within the mitochondrial matrix and as it is unable to cross the impermeable inner membrane, is rapidly converted to H2O2 (itself a ROS), by the action of the enzyme MnSOD. H2O2 is converted to water by mitochondrial GSH or TRX. It appears that GSH is the most abundant antioxidant in mitochondria whilst the TRX system is more efficient. At low levels of oxidative stress both systems appear to keep H2O2 levels under control equally. When oxidative stress increases (e.g. during sepsis) the TRX system appears to become dominant in mitochondrial protection.24 Oxidative Stress Induced Mitochondrial Damage Oxidative stress has been defined as an imbalance with the over-production of ROS and the underproduction of the protective antioxidant systems and has been well described in sepsis. Potential sources for oxidative stress in the critically ill patient include the electron transfer chain, xanthine oxidase activation, neutrophil activation respiratory burst and the metabolism of arachadonic acid.23 The superoxide anion is the ROS initially produced in the mitochondrion. It is formed as a result of electron leak from the oxidative phosphorylation reactions associated mainly with complex I and to a lesser degree with complex III. Page 16 of 31 From in-vivo work with isolated mitochondria, it has been determined that the rate of O2- production is critically dependant on: 1. The proton motive force (∆p) i.e. the mitochondrial membrane potential 2. The NADH/NAD+ ratio 3. The CoQH2/CoQ ratio 4. The local O2 concentration In any situation in which the mitochondria are not producing ATP, they will have an increased ∆p as well as an increased NADH/NAD+ ratio and reduced Coenzyme Q10 pool. All of these factors then promote the formation of O2production. This oxidative stress may then result in damage to lipids, proteins and the nucleic acids of both within the mitochondria as well as the cell by any one of a number of mechanisms 33. Direct toxicity of the ROS to the mitochondrial membrane. The peroxication of the mitochondrial membrane lipid cardiolipin, which is located on the inner membrane, will result in the dissociation of cytochrome C away from the intermembranous space,25 the net effect of which will include decreased ATP synthesis and further increase in ROS production. Nitric oxide competes with oxygen binding to complex IV, thus decreasing the activity of the enzyme. This blocks the electron transfer chain with a resultant overproduction of superoxide. The ROS may also have a direct inhibitory effect on the antioxidant system itself via the oxidisation or peroxidation of the component enzymes. Finally ROS may result in direct damage to mtDNA. This is a very important effect of oxidative stress for the following reasons: 1. The mtDNA is in very close proximity to the electron transport chain, the source of ROS 2. mtDNA encodes for a number of tRNA species, rRNA species as well as proteins that are crucial to the electron transfer chain and energy generation 3. The entire mtDNA encodes for expressed genes (in comparison with the Genomic DNA which has a high proportion of non-coding sequences). Therefore damage to mtDNA is much more likely to result in a functional mutation. Any of these mechanisms will in turn, ultimately result in a self amplifying cycle of more ROS production (aptly named ROS-induced ROS release), until finally the production of ROS will completely overwhelm the antioxidant system with ensuing cell death. This is a concept known as Toxic Oxidative Stress or the Mitochondrial Catastrophe Hypothesis.26 Page 17 of 31 Fig 7: Overview of Mitochondrial ROS Production31 MITOCHONDRIAL CATASTROPHE HYPOTHESIS Under normal circumstances, the inner mitochondrial membrane is impermeable. However there are certain triggers which include oxidative stress, calcium overload and apoptotic protein expression that can result in a concept known as ‘Permeability Transition’ 33. These triggers result in an increase in inner membrane permeability, and the subsequent release of cytochrome C and Apoptosis Inducing Factor. These in turn will activate the caspase cascade. The Caspases (Cysteine-dependent aspartate-directed proteases) are a family of proteases that play an essential role in apoptosis giving them their alternative, somewhat dramatic name of ‘Executioner Proteins’. Page 18 of 31 The critical point of apoptosis appears to be the initial increase in the membrane permeability as once the caspase activators are released the process becomes irreversible. BIOENERGETIC FAILURE To this point, the discussion has been around the progressive deterioration in mitochondrial function which, if not prevented or reversed, will result in a reduction in cellular metabolism to a point at which the organ is no longer able to perform its basic function. An interesting point first raised by Singer in 200427 was the possibility that this bioenergetic failure should possibly not be seen as ‘failure’, at least not initially, but rather as a metabolic shutdown aimed at shifting the cell from normal functioning into a survival mode. Should one subscribe to the theory that mitochondrial dysfunction is not actually mitochondrial failure, then it should be considered to rather be a potential survival mechanism potentially aimed at inducing cellular ‘hibernation’ by triggering a state of suspended animation. This thus possibly protects the organism from the energetic failure until such time as the inflammatory insult has resolved and a recovery can be made. Animals that hibernate or aestivate have the ability to significantly reduce their metabolic energy expenditure. Certain amphibians and reptiles have the ability to withstand periods of hypoxia by suppressing ATP turnover. Whilst humans neither hibernate or aestivate, organs such as the heart have the ability to exhibit abnormalities in contractile function in the face of chronic ischaemia that is potentially reversible once perfusion if re-established, so called myocardial hibernation or stunning, which could represent an adaptive response to hypoxia. Nonetheless, should the mitochondrial dysfunction be persistent, there will be a tipping point at which the minimal threshold level for ATP production is reached and the apoptotic pathways are initiated.27 Page 19 of 31 Fig 8: Postulated progression of mitochondrial dysfunction during sepsis and recovery 28 TREATMENT STRATEGIES Within this model of sepsis-induced MODS, the result of cellular energetic failure, potential treatment strategies may be divided into 3 broad categories: The prevention and reversal of early mitochondrial dysfunction Optimising DO2 – In early sepsis, cellular hypoxia will result in decreased aerobic ATP production and contribute to mitochondrial dysfunction. As a result, the early optimisation of oxygen delivery may prevent bioenergetic failure if instituted whilst the mitochondria are still able to produce ATP. This approach, however, may no longer be beneficial once the mitochondria have already been damaged and energy production has been further affected. It is clear that this dysfunction may also occur even with adequate fluid resuscitation and re-establishment of tissue oxygenation and, in this scenario, failure of oxygen consumption to improve (despite the reestablishment of delivery) has been associated with worse outcomes in septic patients.29 Page 20 of 31 Glucose Control – As discussed previously, both the hyperglycaemia and insulin resistance seen in sepsis pose a threat to mitochondrial functionality. The maintenance of normoglycaemia using insulin was demonstrated by Vanhorebeek to have beneficial effects of hepatic mitochondrial structure and function.13 Antioxidants – The association between sepsis-related organ dysfunction and oxidative stress-mediated mitochondrial dysfunction has opened the door to the possibility of there being a role for the therapeutic administration of antioxidants in critically ill patients. Whilst there is evidence that systemic antioxidant therapy, in particular selenium, glutamine and the Ω-3 fatty acids,30 may improve outcomes in sepsis, systemic antioxidant supplementation has yet to prove specifically successful in critically ill patients.31 It has been postulated that a possible reason for this may be because they did not target the specific intracellular site most affected by oxidative damage, the mitochondria.32 This then has lead to the search for mechanisms in which delivery of the antioxidant directly to the mitochondrion can be achieved consistently and reliably. These approaches are currently undergoing tests in-vitro and in animal models.33 There are a number of methods by which therapeutic delivery to the mitochondrion may be achieved: 1. Delivery of the antioxidant directly to the mitochondria by attaching it to a specific carrier molecule. 2. Administration of an antioxidant that naturally accumulates in or acts on the mitochondrion. 3. Augmentation of the mitochondrial endogenous antioxidant defences via either pharmacological means or by genetic manipulation 33. Currently, in the majority of studies on mitochondrial-targeted antioxidants, treatment has been given prior to the septic insult. This is clearly not congruent with the clinical situation, which would require delaying treatment until sepsis has been established. However, ongoing refinement to these early in-vivo and animal models will allow development of studies that have more relevant applications in humans.26 It should be borne in mind that there are, however, a number of situations in which the timing of the oxidative stress trigger is known in advance, and as such the encouraging trends demonstrated by a number of these studies should not be discounted as entirely clinically irrelevant. Page 21 of 31 Interesting questions that will need to be addressed at some point in the development of this novel treatment modality include the potential ability of the antioxidant to decrease, stop or even reverse established ‘bioenergetic failure’; what the optimal dose and timing of each intervention will be; does the possibility that we may need to target specific modalities to specific organs exist, and what is the place of this modality in other forms of oxidative stress including ischaemia-reperfusion injury, haemorrhagic shock and non-infective SIRS? A more detailed look at the novel treatments currently under investigation can be noted in appendix A. The prevention of energetic failure once mitochondrial dysfunction is established Electron Donors – Succinate dimethyl ester has been shown to reduce hepatic ATP contentin septic models.34 This is achieved by bypassing complex I (which is more significantly affected in sepsis) and allowing the relatively preserved action of complex II to increase the flow of electrons through the electron transfer chain by the oxidation of succinate to coenzyme Q. This will increase ATP generation if there is no rate-limiting inhibition distal to complex II.8 Suspended Animation – Once mitochondrial dysfunction is established, a novel treatment strategy would be to decrease cellular energy expenditure by inducing a state of cellular hibernation.Mice exposed to hydrogen sulphide (H2S) have demonstrated significant decreases in metabolic rate. H2S is a specific, potent, reversible inhibitor of Complex IV (Cytochrome C Oxidase) and exposure in a concentration of 80ppm resulted in body temperature approaching that of the environment and oxygen consumption and carbon dioxide production both decreasing as much as 90% from baseline.35 On reversal of the hydrogen sulphide, this state of suspended animation is reversed with no permanent behavioural or functional sequelae. This radical approach would carry with it a number of complexities; the cooling associated with suspended animation would negate the cytoprotective effects of heat shock proteins which require the hyperthermic response to infection in order to be expressed. A further complication may then be timing of the reversal of ‘hibernation’, with premature stimulation before the mitochondria are ready to resume energy production resulting in cellular compromise.8 β Blockers – Sepsis has also been described as the ‘rude unhinging of metabolism’36 which results in activation of the sympathetic nervous system, hyperglycaemia and insulin resistance, breakdown of proteins and systemic vasodilatation amongst other things. All of these effects would be potentially attenuated with the use of Beta Blockers.37 Page 22 of 31 It may seem reasonable to consider a treatment strategy that deviates from maximising oxygen delivery to one which attempts to minimise oxygen requirements. Whilst controversial, the use of Beta Blockers would potentially fulfil this role in decreasing cardiac workload and VO2 assuming DO2 has been optimised. There are no current human studies that address the issue of Beta Blockade in sepsis, with most of the evidence either being extrapolated from non septic populations (including medical, burns and trauma) or from animal based septic models.38 The resolution of the mitochondrial dysfunction Whilst the trigger for this step has yet to be discovered, the repair and replacement of the damaged and dysfunctional mitochondria are likely to be controlled at the transcriptional level. Nitric Oxide – whilst high quantities of NO- produced during the inflammatory response are cytotoxic and result in mitochondrial dysfunction, it has recently been established that small quantities of cNOS-derived endothelial NO- may be a major trigger in mitochondrial biogenesis.8 Hormone supplementation – Thyroid hormone stimulates mitochondrial activity and has been shown to up-regulate mitochondrial related transcription factors in mice.39 The low circulating T3 seen in chronic illness may be the result of neuroendocrine dysfunction and the correct timing of thyroid hormone supplementation may be a potent stimulant of mitochondrial activity and metabolic rate and may promote early organ recovery. As mentioned preciously, premature stimulation of ‘hibernating’ mitochondria may have detrimental effects on the cell as well. The potential benefits of other hormone supplementation, namely Leptin and Oestrogen,have been mentioned previously. Page 23 of 31 Fig 9: Potential therapeutic Interventions in mitochondrial dysfunction8 CONCLUSION The principles of intensive care are supportive and still almost all interventions undertaken in the critically ill patients including mechanical ventilation, inotropic support, endocrine supplementation and immunonutrition have all been associated with adverse outcomes. The potential causes of ‘bioenergetic’ failure in sepsis are multifactorial and range from genetic predisposition to imbalances between oxygen delivery and oxygen use to mitochondrial damage as a result of oxidative stress. Mitochondrial dysfunction may be as a result of direct or indirect damage from both ROS and NOS (oxidative stress), decreased expression of mitochondrial proteins or as a result of the metabolic and hormonal disruptions that occur in sepsis. As in many of the body’s responses to an insult, sepsis should possibly be viewed not as an uncontrolled, damaging process but possibly as an intricate, multisystemic condition that includes both protective and damaging pathways. Page 24 of 31 Although MODS may be the end result of ‘bioenergetic failure’, it may also represent an adaptive process to the reduced energy supply in an attempt to allow the organ to recover enough function to allow long-term recovery, should the initial insult be controlled. Should this be the case, we need to understand that any treatment or intervention we institute may be deleteriously affecting this adaptive attempt and in so doing, may result in detrimental consequences.7 We should also be aware that as a result of sepsis being a dynamic process, the timing of interventions may be crucial to the outcome. The renewed interest in attempting to address the imbalance between ROS overproduction and antioxidant deficits in sepsis, especially by targeting delivery of antioxidants directly to the source of the ROS production, the mitochondria, may have potential as novel future treatments in MODS- associated sepsis. APPENDIX A – NOVEL ANTIOXIDANT THERAPIES Lipophilic cations Liphophilic cations will accumulate in the mitochondria as a result of its negative membrane potential (-150 to -180mV). By covalently binding a specific antioxidant molecule to the cation, delivery to the mitochondrion can be ensured. A number of different formulations are being utilised e.g. MitoQ attaches the antioxidant coenzyme Q10 (ubiquinone) to the cation triphenylphosphonium (TPP). Accumulation of MitoQ in the mitochondrion is 500 times the levels of those found in the cytoplasm. Once inside, the MitoQ will be absorbed into the inner membrane and recycled into ubiquinol which is then active in the respiratory chain.40 MitoQ is the most well-studied of the mitochondrial targeted antioxidants. Whilst some reservations have been expressed as to the potential efficacy of these cations in septic patients on the basis that the dysfunctional mitochondria may have a reduced ability to accumulate them, MitoQ has been shown to provide better protection to oxidative stress-mediated injury in treated when compared with non treated tissue both in-vitro, and in animal models.41, 30 In addition to its antioxidant effects, MitoQ has anti-inflammatory effects. In conditions of sepsis induced in human epithelial cells, it has been shown to be able to decrease ROS production and offer protection to the mitochondrial membrane. It has also been shown to decrease Interleukin-6 (IL-6) and IL-8 release during in vitro lipopolysaccharide stimulation.42 Sepsis-induced cardiac dysfunction has also been attenuated in rat models following administration of MitoQ.43 Other compounds that have been conjugated to TPP include: Tocopherol (MitoVitE) The peroxidase compound Ebselen (MitoPeroxidase) Plastoquinone (SkQ) Page 25 of 31 Fig 9: The Lipophillic Cations 26 Antioxidant Peptides SS Peptides, so called because they were designed by Szeto and Schiller42 are small, synthetic, positively-charged peptides containing less than 10 amino acids. They are able to freely enter cells by passive diffusion and as a result of their positive charge; they will accumulate within the mitochondria. The peptide sequence is a proprietary formulation and based on ischaemia-reperfusion models of oxidative stress, they appear to have the ability to scavenge a number of different ROS.44 Hemigramacidin–TEMPOL Conjugates TEMPOL is a compound that has the ability to scavenge ROS. Conjugation of this molecule to hemigramacidin (which is part of the antibiotic Gramacidin-S that has a high affinity for the mitochondrial membrane) will result in the compound being targeted directly to the mitochondria. Studies in rat haemorrhagic shock models have shown benefit in TEMPOL treated tissues when compared with nontreated.45 Page 26 of 31 Increasing Endogenous Mitochondrial Antioxidants Glutathione is the most common of the endogenous antioxidant mechanisms. It is synthesised in the cytoplasm from its 3 component amino acids: cysteine, glycine and glutamate. After synthesis it is transported into the mitochondrion. Compounds such as glutathione N-acetyl-L-cysteine choline esters have been shown to be able to increase the availability of endogenous glutathione by acting as a source for the component amino acids. In vitro studies are promising but this has yet to be studied in models of sepsis.46 Genetic Manipulation Novel genetic approaches to increasing endogenous antioxidant production include adenoviral transfection of human MnSOD into rats. This has resulted in increased hepatic MnSOD activity with a reduction in oxidative damage induced by both alcohol and by ischaemia-reperfusion. 47,48 Melatonin Melatonin is synthesised from the amino acid tryptophan. The highest concentrations of melatonin within the cells are found in the mitochondria. Both melatonin and a number of its metabolites have been shown to have profound antioxidant activity. Melatonin has been shown to prevent mitochondrial dysfunction, energy failure and apoptosis as well as attenuating the inflammatory cytokine release in animal models of oxidative injury.49 Page 27 of 31 REFERENCES 1. Marshall JC, Vincent JL, Guyatt G, et al. Outcome measures for clinical research in sepsis: a report of the 2nd Cambridge Colloquium of the International Sepsis Forum. Crit Care Med 2005; 33: 1708–16 2. Mitchell P. Fink MD Cytopathic Hypoxia: Mitochondrial Dysfunction as Mechanism Contributing to Organ Dysfunction in Sepsis Critical Care ClinicsVolume 17, Issue 1, 1 January 2001, Pages 219-237 3 Barcroft J: On anoxaemia. Lancet 2:485, 1920 4 Singer M, Brealey D. Mitochondrial dysfunction in sepsis. Biochem Soc Symp. 1999;66:149-66 5 Kreymann G, Grosser S, Buggisch P, Gottschall C, Matthaei S, Greten H: Oxygen consumption and resting metabolic rate in sepsis, sepsis syndrome, and septic shock. Crit Care Med 1993, 21:1012-1019. 6 Boekstegers P, Weidenhofer S, Kapsner T, Werdan K: Skeletal muscle partial pressure of oxygen in patients with sepsis. Crit Care Med 1994, 22:640-650. 7 Abraham, Singer. Mechanisms of sepsis-induced organ dysfunction. Crit Care Med 2007 Vol. 35, No. 10 8 Protti A, Singer M, Bench-to-bedside review: Potential strategies to protect or reverse mitochondrial dysfunction in sepsis-induced organ failure Critical Care 2006, 10:228 9 Image from www.wikipaedia.com 10 Chipuk JE, Bouchier-Hayes L, Green DR (2006). Mitochondrial outer membrane permeabilization during apoptosis: the innocent bystander scenario". Cell Death and Differentiation.13 (8): 1396–1402 11 Murphy MP. How mitochondria produce reactive oxygen species. Biochem. J. 2009 417 (1): 1–13 12 Brealey D, Karyampudi S, Jacques TS, et al. Mitochondrial dysfunction in a long-term rodent model of sepsis and organ failure. Am J Physiol Regul Integr Comp Physiol 2004; 286: R491–7 13 Vanhorebeek I, De Vos R, Mesotten D, Wouters PJ, De Wolf-Peeters C, Van den Berghe G. Protection of hepatocyte mitochondrial ultrastructure and function by strict blood glucose control with insulin in critically ill patients. Lancet 2005; 365: 53–9 Page 28 of 31 14 Brealey D, Brand M, Hargreaves I, et al. Association between mitochondrial dysfunction and severity and outcome of septic shock. Lancet 2002; 360: 219–23 15 Arnalich F, Garcia-Palomero E, Lopez J, et al: Predictive value of nuclear factor kappaB activity and plasma cytokine levels in patients with sepsis. Infect Immun 2000; 68:1942–1945 16 Calvano SE, Xiao W, Richards DR, Felciano RM, Baker HV, Cho RJ, Chen RO, Brownstein BH, Cobb JP, Tschoeke SK, et al.: A network-based analysis of systemic inflammation in humans. Nature 2005, 437:1032-1037. 17 Callahan LA, Supinski GS: Sepsis induces diaphragm electron transport chain dysfunction and protein depletion. Am J Respir Crit Care Med 2005, 172:861-868. 18 Bornstein SR, Licinio J, Tauchnitz R, Engelmann L, Negrao AB, Gold P, Chrousos GP: Plasma leptin levels are increased in survivors of acute sepsis: associated loss of diurnal rhythm, in cortisol and leptin secretion. J Clin Endocrinol Metab 1998, 83:280-283 19 Orci L, Cook WS, Ravazzola M, Wang MY, Park BH, Montesano R, Unger RH: Rapid transformation of white adipocytes into fat-oxidizing machines. Proc Natl Acad Sci USA 2004, 101:2058-2063. 20 Hsieh YC, Yang S, Choudhry MA, Yu HP, Bland KI, Schwacha MG, Chaudry IH: Flutamide restores cardiac function after trauma-hemorrhage via an estrogen-dependent pathway through upregulation of PGC-1. Am J Physiol Heart Circ Physiol 2006, 290:H416-H423. 21 Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, Peterson E, Tomlanovich M: Early goal-directed therapy in the reatment of severe sepsis and septic shock. N Engl J Med 2001, 345:1368-1377. 22 Aviram M. Review of human studies on oxidative damage and antioxidant protection related to cardiovascular disease. Free Radic Res 2000; 33; S8597 23 Lacza Z, Pankotai E, Csorda´s A, et al. Mitochondrial NO and reactive nitrogen species production: does mtNOS exist? Nitric Oxide 2006; 14: 162–8 24 Lowes DA, Galley HF. Mitochondrial protection by the thioredoxin-2 and glutathione systems in an in vitro endothelial model of sepsis. Biochem J 2011 Feb 28 25 James AM, Murphy MP. How mitochondrial damage affects cell function. J Biomed Sci 2002; 9: 475 Page 29 of 31 26 Fariss MW, Chan CB, Patel M, Van Houten B, Orrenius S. Role of mitochondria in toxic oxidative stress. Mol Interv 2005; 27 Singer M, De Santis V, Vitale D, Jeffcoate W: Multiorgan failure is an adaptive, endocrine-mediated, metabolic response to overwhelming systemic inflammation. Lancet 2004, 364:545-548. 28 Singer M. Mitochondrial function in sepsis: Acute Phase vs Multiple Organ Failure. Crit Care Med 2007;35:S441-S448 29 Hayes MA, Timmins AC, Yau EH, Palazzo M, Watson D, Hinds CJ: Oxygen transport patterns in patients with sepsis syndrome or septic shock: influence of treatment and relationship to outcome. Crit Care Med 1997, 25:926-936. 30 Rinaldi S, Landucci F, De Gaudio AR. Antioxidant therapy in critically ill septic patients. Curr Drug Targets 2009; 10: 872–80 31 Mishra V. Oxidative stress and role of antioxidant supplementation in critical illness. Clin Lab 2007; 53: 199–209 32 Galley HF. Bench-to-bedside review: targeting antioxidants to mitochondria in sepsis. Crit Care 2010; 14: 230 33 Galley HF, Oxidative stress and mitochondrial dysfunction in sepsis BJA 107 (1): 57–64 (2011) 34 Malaisse WJ, Nadi AB, Ladriere L, Zhang TM: Protective effects of succinic acid dimethyl ester infusion in experimental endotoxemia. Nutrition 1997, 13:330-341. 35 Blackstone E, Morrison M, Roth MB: H2S induces a suspended animation-like state in mice. Science 2005, 308:518. 36 Gore, Wolfe: Hemodynamic and metabolic effects of selective b1 adrenergic blockade during sepsis. Surgery 2006;139:686-694 37 Norbury et al. Crit Care Med 2007;35:S616-S620 38 Takeshi Suzuki et al, Infusion of the B-adrenergic blocker esmolol attenuates myocardial dysfunction in septic rats. Crit Care Med 2005 Vol. 33, No. 10 39 Weitzel JM, Radtke C, Seitz HJ: Two thyroid hormone-mediated gene expression patterns in vivo identified by cDNA expression arrays in rat. Nucleic Acids Res 2001, 29:5148-5155. 40 Smith RA, Murphy MP. Animal and human studies with the mitochondriatargeted antioxidant MitoQ. Ann N Y Acad Sci 2010; 1201: 96–103 Page 30 of 31 41 Adlam VJ, Harrison JC, Porteous CM, et al. Targeting an antioxidant to mitochondria decreases cardiac ischemia–reperfusion injury. FASEB J 2005; 19: 1088–95 42 Lowes DA, Thottakam BM, Webster NR, Murphy MP, Galley HF. The mitochondria-targeted antioxidant MitoQ protects against organ damage in a lipopolysaccharide-peptidoglycan model of sepsis. Free Radic Biol Med 2008; 45: 1559–65 43 Supinski GS, Murphy MP, Callahan LA. MitoQ administration prevents endotoxin-induced cardiac dysfunction. Am J Physiol Regul Integr Comp Physiol 2009; 297: R1095–102 44 Szeto HH. Mitochondria-targeted cytoprotective peptides for ischemia– reperfusion injury. Antioxid Redox Signal 2008; 10: 601–19 45 Fink MP, Macias CA, Xiao J, et al. Hemigramicidin-TEMPOL conjugates: novel mitochondria-targeted antioxidants. Crit Care Med 2007; 35: S461–7 46 Sheu SS, Nauduri D, Anders MW. Targeting antioxidants to mitochondria: a new therapeutic direction. Biochim Biophys Acta 2006; 1762: 256–65 47 Wheeler MD, Nakagami M, Bradford BU, et al. Overexpression of manganese superoxide dismutase prevents alcohol-induced liver injury in the rat. J Biol Chem 2001; 276: 36664–72 48 Wheeler MD, Katuna M, Smutney OM, et al. Comparison of the effect of adenoviral delivery of three superoxide dismutase genes against hepatic ischemia–reperfusion injury. Hum Gene Ther 2001; 12: 2167–77 49 Lowes DA, Almawash AM, Webster NR, Galley HF. Role of melatonin and indole-derivatives on endothelial cells in an in vitro model of sepsis (abstract). Br J Anaesth 2010; 104: 525P 50 Mitchell M. Levy, Mitchell P. Fink, John C. Marshall, Edward Abraham, Derek Angus, Deborah Cook, Jonathan Cohen, Steven M. Opal, Jean-Louis Vincent, Graham Ramsay, 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference Crit Care Med 2003 Vol. 31, No. 4 Page 31 of 31