Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Nonsynaptic plasticity wikipedia , lookup
Electrophysiology wikipedia , lookup
Threshold potential wikipedia , lookup
Proprioception wikipedia , lookup
Membrane potential wikipedia , lookup
Haemodynamic response wikipedia , lookup
End-plate potential wikipedia , lookup
Resting potential wikipedia , lookup
Single-unit recording wikipedia , lookup
Pre-Bötzinger complex wikipedia , lookup
Neuroplasticity wikipedia , lookup
G protein-gated ion channel wikipedia , lookup
Synaptic gating wikipedia , lookup
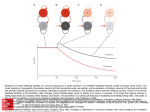
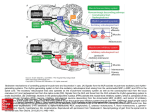
Physiology The History of Physiology • Aristotle emphasized the relationship between structure and function • Galen was the first to perform experiments to understand the function of the body • Muslim physicians, such as Avicenna, started the formal study of physiology by writing books probing the functions of many different parts of the body • In the 17th century William Harvey first describes the circulatory system and its interaction with the body • Many advances in the understanding of physiology came in the 19th century. Between Schleidan and Schwann’s cell theory to Walter Cannon’s development of homeostasis, physiology was being understood faster than ever. The Neuron 3 Types of Neurons Unipolar Neuron • Function: Acts as sensory neurons. • Description: The presence of one Axon that branches at the terminal end. • Location: Absent in adult humans, but common in human embryos and invertebrates Bipolar Neurons • Function: It acts as a sensory neuron. • Description: A single axon and a single dendrite are located at opposite poles of the cell body. • Location: They serve as the sensory neurons within the retina, olfactory, auditory systems. Multipolar Neurons • Function: allows for the integration of information from other neurons • Description: Multiple dendritic processes with a single axon. • Location: Most abundant neuron found in the human body. It is located in the brain, and the peripheral autonomic nervous system and the spinal cord. Transmission of a Nerve Impulse 1.Stimulation of a neuron causes the opening of voltage gated sodium ion channels. This leads to an influx of sodium ions into the cell. 2.After the rush of sodium ions, the membrane becomes depolarized due to the reversal of the resting potential. 3.As a result, the sodium ion channels become inactive for a very short amount of time during this refractory period and the sodium ions are not allowed to travel across the channel. 4.During the refractory period, voltage gated potassium ion channels open and allow potassium ions out of the membrane which restores the resting potential. 5.Hyper polarization may occur to the sudden rush of potassium ions across the membrane. 6.Once the resting potential is fully restored, the voltage gated potassium ion channels close. 7.The refractory period is ended with the opening of the inactivated gate of the voltage gated sodium ion channels. Name Types of Neuroglia Function Location Schwann Cells Myelinate the PNS PNS Oligodendrocyte Myelinate the CNS CNS Microglia Remove debris and pathogens CNS&PNS Astroglia Hold neurons in place in the CNS CNS Epindymal Cells Move CSF in the CNS CNS Satellite Cells Hold neurons in place in the PNS PNS Synonyms Oligodendroglia Star Cells The 12 Cranial Nerves The Major Brain Regions Index of Brain • 1)Cerebrum • • • • • • • • • • • • • • • • • • • • • • • • Communication Remembering Understanding Perceiving Appreciating Initiating voluntary movement Memory Language Sensation awareness Emotional processing Taste Smell Sight Comprehending Visceral sensations Intellectual processing Sound Learning Reasoning Touching Imagination Personality Thought processes Eye and face movement 2) Brain Stem a) Midbrainsound and sight reflex center contains nuclei for cranial nerves 3 & 4 red nuclei-motor center constricts pupil of eye b) Pons contains nuclei for cranial nerves 5-7 together with medullary respiratory centers, helps maintain normal rhythmic breathing. c) Medulla adjust force and rate of heart contraction regulates blood pressure by changing blood vessel diameter controls rate and depth of breathing and maintains respiratory rhythm regulates activities such as vomiting, hiccupping ,swallowing, coughing & sneezing. Cranial nerves 8-12 are housed here Produces state of consciousness 3) Cerebellum Regulates posture Regulates balance Regulates coordination of smooth skeletal muscle 4) Diencephalon a) Thalamus- some memory processing relay center for relay impulses relay center for impulses to and from cerebral motor cortex and lower motor centers b) Hypothalamus -Influences blood pressure rate and force of heart contraction motility of the digestive tract respiratory rate and depth eye pupil size sex drive perceptions of rage ,fear, pain body temperature regulates food intake regulates water balance and taste regulated biological clock controls function of endocrine system c) Epithalamusregulates sleep/wake cycle aspect of mood Flow of CSF Choroid Plexus of the Lateral Ventricle->Foramen of Monroe->3rd Ventricle->Choroid Plexus>Cerebral Aqueduct->4th Ventricle->Central Canal of Cord/Dorsal Subarachoid Space of the Brain/Subarachnoid Space behind the Cerebellum>Arachnoid Granulations->Cerebral Sinus Movement and Motion Anatomical Movement Neurotransmitters NAME EXCITATORY/INH IBITORY REMOVAL Acetylcholine Excitatory AchEase Glutamate Excitatory Transporters GABA Inhibitory Transporters Glycine Inhibitory Transporters Epinephrine Excitatory Transporters, MAO, COMT Norepinepherine Excitatory Transporters, MAO, COMT Dopamine Excitatory Transporters, MAO, COMT Serotonin Excitatory Transporters, MAO Histamine Excitatory Transporters Adenosine Triphosphate Excitatory Hydrolysis to AMP, Adennosine Neuropeptides Excitatory and Inhibitory Proteases Substance P Excitatory Inhibited by Opioids Endorphins Inhibitory Enkephriones Inhibitory Dynorphines Inhibitory Neurotoxins NAME PRODUCER EFFECTS Atropine Bella Donna Increased Heart Rate Scopolomine Henbane Truth Serum Muscarines Red Mushroom (Amenita) Stimulation of the CNS, Vomiting, Nausea, Death, Coma Nicotine Tobacco Plant (Leaves) Stimulation of CNS Tetrotoxin Pufferfish Paralysis Saxitoxin Shellfish (Consumers of Reld Algae) Paralysis Alpha Toxin Scorpions Increased Action Potential Beta Toxin Scorpions Voltage Shift in Na Channels Clostridium Botulinium Clostridium Bacteria Preventions of NT release Clostridium Tenani Clostridium Bacteria Muscle and Skeletal Contractions PAIN Phantom Pain Phantom pain is the pain produced in amputees in a limb that is no longer present. Even though the limb is gone, patients suffer from pain where it used to be. This is possible because the brain still believes the limb is present and tries to prove it still exists. Phantom pain is treatable but if the stump is re-injured the pain may persist. If phantom pain is not treated it may result in chronic pain to the patient. The Gate Theory of Pain The gate theory of pain relates to pain modulation. When you stub your toe, you automatically begin to rub it, and it then soon feels better. This happens because of the brain becomes confused with the signals it receives from the mechanoreceptors in the injured area. When you are injured, the noicoreceptors and mechanoreceptors send a pain impulse to the brain, thus resulting in pain. When you rub the area, the mechanoreceptors pick up your touch and send the impulse to the brain. The simultaneous reception of these senses confuses the brain and it interprets them as a rub, thus subsiding the pain. The area actually becomes momentarily desensitized to pain because the mechanoreceptors confuse the brain. Perception of Pain Pain is senses by nerves called noicioreceptors. These receptors can sense two types of pain, first and second pain. First pain is the pain felt at the onset of an injury. It is sensed with A fibers which are myelinated and can transmit the pain very quickly, thus why is appears almost instantly with an injury. In the case of second pain, pain is more of a dull, slow building, aching pain. This happens because the receptors are unmyelinated C fibers. These fibers slowly transmit pain giving the feeling of an ache or a slow deep pain. Referred Pain Referred pain is pain that is felt outside of an injured area. The body cannot transmit the impulse fast enough through one path so it affects another part of the body to conduct the impulse fasted. An example is with angina. When tightness of the chest and pain in the arm are sensed, it is usually a sign of visceral problems. Since the viscera isn’t innervated as well as the extremities, the body refers the pain to another part of the body to alert the brain faster.