Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gluten immunochemistry wikipedia , lookup
Duffy antigen system wikipedia , lookup
Complement system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Autoimmunity wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Immunocontraception wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Molecular mimicry wikipedia , lookup
Immune system wikipedia , lookup
DNA vaccination wikipedia , lookup
Innate immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Adaptive immune system wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
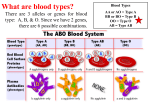
Immunology Basics: I Objectives: Understand What is an immune response ? Jargon; humoral and cellular immune responses Structure and differential specificity of immunoglobulins B lymphocyte life cycle and function Blood transfusion compatibility as a classic example of antibodymediated immune response Indirect and direct Coombs tests Neonatal rhesus disease as a classic antibody-mediated disorder Jargon: Antibody: a globulin that binds more or less specifically to a small number of antigens Antigen: a substance capable of being bound by an antibody, e.g., viral capsid, bacterial cell wall component, specific proteins, etc. Immune response: a biologically observable effect following the interaction of an antigen with antibodies or lymphocytes; usually it is inflammation of some sort Plasma cells: B lymphocytes IMMUNE RESPONSES ‘Afferent’ pathway Antigen challenge presents Initial detection by B or T lymphocytes Small, sometimes undetectable immune response Amplification of T or B lymphocyte population Large, detectable immune response Traditionally… Immune responses have been termed ‘humoral’ when involving B lymphocytes and antibodies Or ‘Cellular’ when involving T lymphocytes, various cytokines and killer T lymphocytes IN FACT - these are not as clearcut and there are many examples of both these ‘systems’ co-operating AIM: Eliminate the abnormal by digesting them Immune responses, one way or other, mark abnormal cells and facilitate digestion Immunoblogulins: classes G: Lightest class, commonest type of B cell A: Found on mucosal linings, especially the gut ( 3 – 5 g / day, more than all others combined, dimers, acid-resistant) M: Pentamers of class G (e.g. most blood group antibodies) E(osinophil): Associated with mast cells and histamine release D: Always found with IgG on lymphocyte surfaces, function unclear (absent in birds, recently detected on basophil membranes) IgG Monoclonal m.w.=150,000Da Aspirin m.w.180 Adapted from US FDA at: http://www.fda.gov/downloads/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/therapeut icbiologicapplications/biosimilars/ucm292463.pdf, accessed 22 Sep 2013 IgG ‘Crystalline fragment’ (Fc); similar in all clones Disulfide bridges ‘Antibody fragment’ (Fab); SPECIFIC to clone. Cartoon of IgM B lymphocyte responses - Germ cells live in lymph nodes, Peyer’s patches, spleen, etc - By a complicated bit of genetics, these cells have INNATE ability to recognise antigens - Some circulate and find antigens, others are presented with antigens by ‘antigen presenting lymphocytes’ (AFFERENT) - B lymphocyte responds by: - Secreting a relevant immunoglobulin - massive reproduction (cloning) - cloned cells depart lymphnode for circulation (EFFERENT) Peyer’s patches Courtesy: Boston University School of Medicine Lymph node DRAINAGE Blood transfusion: a classic antibody-antigen reaction 1900: Landsteiner developed the A,B, AB, O group system 1940: Lansteiner and Weiner identify the first Rhesus epitope Transfusion: adverse reactions 1. Infection 2. Volume overload 3. Fever 4. CLOTTING THEN 5. Haemolysis (DIC) 6. Allergy to excipients 7. Late-onset immune responses 8. Purpura (mismatched platelets) PMNs secreting complement 9. Transfusion associated lung injury (? HLA mismatch) About 10 μm ABO Compatibility: 1 PLASMA (Only antibodies, negligible antigen) DONOR O (anti-A, antiB) RECIPIENT O A B AB OK A (anti-B) OK B (anti-A) OK OK AB (no abs) OK OK OK OK OK RECIPIENT ABO and Rhesus Compatibility: 2 Packed red blood cells DONOR O (anti-A, antiB) A (anti-B) B (anti-A) Rh- Rh+ Rh- Rh+ Rh- Rh+ O+ O- OK OK OK A+ A- OK OK OK B+ B- OK OK OK AB+ AB- OK OK OK OK OK OK OK OK OK AB (no abs) Rh- Rh+ OK OK OK OK OK OK OK OK Blood Groups Rhesus: Five epitopes, Dd, Cc, Ee Aa Bb Numerous alleles; ? A membrane transporter; Short arm Chromosome 1 Rarely allegenic Europe: Roughly 85% D+ (DD or Dd) Asia: dd rarer than Europe The rhesus macaque Macaqua mulatta Declining importance in clinical immunogenicity Blood groups Duffy +/Lewis Le(0) Le(b) Kell (haemolytic disease of newborn) MNS Another 24 systems Mostly Glycoproteins Fucosylproteins Or Lipoproteins Mostly named after index family Coombs test: Direct Are there antibodies on red cells (autoimmune haemolysis) ? Anti-coagulated blood sample Spin and wash RBC sample Challenge with generic anti-Fc human globulin antibody AGGLUTINATION = PRESENCE OF Abs In original sample Coombs test, Indirect (Blood grouping) Are there already soluble antibodies in the plasma that will bind to a proposed red cell transfusion ? Coagulated blood sample Spin for serum Add serum to panel of grouped red cells AGGLUTINATION = PRESENCE OF Abs In original PLASMA sample Add anti-human globulin Cross-matching Rhesus incompatibility mother / foetus: Classic example of early versus amplified immune response Para 1 MOTHER: RHESUS NEGATIVE FOETUS: RHESUS POSITIVE = NORMAL OUTCOME NO afferent: No Foetal / maternal red cell exchange until delivery - insignificant direct challenge to the Rh+ neonate (small volume) = no direct harm - immunization of mother at delivery; about 7 days to full-size clones Para 2 MOTHER: RHESUS NEGATIVE FOETUS: RHESUS POSITIVE Maternal IgM crosses the placenta = PREGNANCY LOSS What is the treatment ? Where does it come from ? SUMMARY Jargon Antibody structure B lymphocyte function Blood transfusion as an example NEXT TIME Radioimmunoassays Auto-immune disease ‘Cellular Immunity’ Immune modulating drugs