Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Zinc finger nuclease wikipedia , lookup
Non-coding DNA wikipedia , lookup
Human genetic variation wikipedia , lookup
Epigenomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Point mutation wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Causes of transsexuality wikipedia , lookup
Public health genomics wikipedia , lookup
Genome evolution wikipedia , lookup
Polymorphism (biology) wikipedia , lookup
Gene desert wikipedia , lookup
Gene expression profiling wikipedia , lookup
Gene nomenclature wikipedia , lookup
Gene expression programming wikipedia , lookup
Gene therapy wikipedia , lookup
Genome (book) wikipedia , lookup
Genome editing wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Genetic engineering wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Helitron (biology) wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
History of genetic engineering wikipedia , lookup
Designer baby wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Microevolution wikipedia , lookup
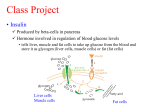
Clinical Science (1999) 96, 659ñ662 (Printed in Great Britain) Insulin gene polymorphism and premature male pattern baldness in the general population Justine A. ELLIS, Margaret STEBBING and Stephen B. HARRAP Department of Physiology, University of Melbourne, Parkville, Victoria 3052, Australia A B S T R A C T Insulin is found in hair follicles and may play a role in the regulation of androgen metabolism and the hair growth cycle, which are relevant to the loss of scalp hair known as male pattern baldness. An excess of dihydrotestosterone on balding scalp indicates that the condition is androgen dependent. Premature male pattern baldness may be the male phenotype of familial polycystic ovary syndrome, a condition characterized by high levels of androgens and insulin that has been linked to insulin gene polymorphism. Therefore, we studied possible associations between relevant insulin gene polymorphisms and premature male pattern baldness in the general community. We examined the distribution of three dimorphic restriction fragment length polymorphisms : HphI, PstI and FokI in cases consisting of 56 men aged 18–30 years with significant baldness, and in 107 control men aged 50 years or more with no indication of baldness. No significant differences between cases and controls in allele, genotype or haplotype frequencies were identified. We conclude that, in the general population, the insulin gene is not associated with premature male pattern baldness. INTRODUCTION Male pattern baldness (MPB) is defined as the genetically predisposed loss of scalp hair which follows a defined pattern and is androgen dependent [1,2]. The mode of inheritance of MPB is often cited as autosomal dominant [3], but a polygenic aetiology appears more likely [4,5]. The genetic defect(s) underlying this condition are unknown, although clues are provided by the excess production of dihydrotestosterone on balding scalp [6]. Dihydrotestosterone is formed from the reduction of testosterone by the action of the enzyme 5α-reductase. The genes encoding the two forms of 5α-reductase were for some time suspected of involvement in MPB, but we have recently shown that common variants of these genes do not appear to be associated with this disorder [5]. Polycystic ovary syndrome (PCOS) is a familial endocrine disorder affecting as many as 10 % of females of reproductive age. It is characterized by hyper- androgenism and hyperinsulinaemia. Peripheral insulin resistance appears to be the main cause of the hyperinsulinaemia, and PCOS patients have a 7-fold increased risk of Type II (non-insulin-dependent) diabetes [7]. In males from families with PCOS, an increase in the prevalence of premature MPB (significant balding before 30 years of age) in an autosomal dominant pattern of inheritance [8,9] has led investigators to suggest that premature MPB is the male phenotype of the disease [9,10]. The genetic disorder(s) underlying PCOS may therefore provide clues for MPB. Recently, linkage and association of familial PCOS with the insulin gene (INS) regulatory variable number of tandem repeats (VNTR) was reported [7]. Apart from their association in PCOS [11–13], androgen and insulin pathways appear to be closely linked in both women and men [14]. There is a strong association between circulating levels of insulin and sex hormonebinding globulin, and possibly between insulin and Key words : androgen, androgenetic alopecia, hair, polycystic ovary syndrome. Abbreviations : MPB, male pattern baldness ; PCOS, polycystic ovary syndrome ; PCR, polymerase chain reaction ; RFLP, restriction fragment length polymorphism ; VNTR, variable number of tandem repeats. Correspondence : Professor Stephen B. Harrap. # 1999 The Biochemical Society and the Medical Research Society 659 660 J. A. Ellis and others testosterone in normal, obese and diabetic men [14–20]. Furthermore, insulin found in hair follicles appears to play a role in the control of the growth cycle of the hair [21]. In view of its linkage with PCOS and potentially important effects on androgen metabolism generally, the INS gene is a good candidate for MPB. Importantly, the INS polymorphism linked to PCOS is thought to have functional effects on INS gene expression [22]. Therefore, we performed a population-based case-control association study of the INS gene in premature MPB using three dimorphic restriction fragment length polymorphisms (RFLPs), one of which is in strong allelic association with the VNTR [7]. METHODS Sampling The details of recruitment and the characteristics of participants have been reported previously [5]. Approximately 3000 Caucasian individuals were recruited as part of the Victorian Family Heart Study. This is a general population survey of coronary risk factors and consists of approximately 800 families, comprising a mother, father and at least one natural offspring. Baldness survey questionnaires were sent to all males (approximately one half of the sample number) asking them to detail their degree of baldness, if any, in terms of the Hamilton baldness scale [2,23]. The survey described all categories of the scale, and provided diagrams to assist in the selfassessment. Validation of this self-reported questionnaire approach has been reported previously [5]. A total of 1073 men returned the completed baldness questionnaires. This group contained 529 sons aged 18 to 30 years and 544 fathers aged 50 years and above. Cosmetically significant baldness of type III or greater [23] was reported by 58 (11.0 %) sons aged 18 to 30 years. These individuals were defined as cases and DNA was available for analysis in 56 of these subjects. A total of 114 fathers aged 50 and above (21.0 %) reported no baldness (Hamilton baldness score of I). Two individuals were identified as fathers of young balding men used in the case group, and were therefore excluded from the study. DNA was available from 107 of the remaining individuals who comprised the control group for our genetic analyses. Analysis of RFLPs of the INS gene DNA was extracted from leucocytes using standard phenol\chloroform techniques. Approximately 50 ng of DNA from each individual was used in polymerase chain reactions (PCRs). The HphI RFLP, located 573 bp distal to the regulatory VNTR and k23 bp from the start site of the INS gene, was detected by amplification of DNA # 1999 The Biochemical Society and the Medical Research Society using primers ins04 (5h-TCCAGGACAGGCTGCATCAG-3h) and ins05 (5h-AGCAATGGGCGGTTGGCTCA-3h) [24]. DNA was added to a mix containing 0.5 µM of each primer, 1iPCR buffer (Perkin–Elmer Applied Biosystems, Norwalk, CT, U.S.A.), 250 µM dNTP (Perkin–Elmer Applied Biosystems), 1.5 mM MgCl (Perkin-Elmer Applied Biosystems) and 1 unit # Amplitaq Gold DNA polymerase (Perkin–Elmer Applied Biosystems), to give a total reaction volume of 20 µl. The thermal conditions required for the reaction were 95 mC for 10 min (for activation of the Amplitaq Gold enzyme), followed by 35 cycles of 95 mC for 1 min, 64 mC for 1 min and 72 mC for 1 min, followed by a final extension time of 72 mC for 10 min. Products were then digested by the addition of 5 units of HphI restriction endonuclease (New England Biolabs, Beverly, MA, U.S.A.) in the presence of 1ibuffer ‘ 4 ’ (New England Biolabs) at 37 mC for 1 h. Digested products were then electrophoresed through a 2 % agarose gel (Type II-A, Sigma, St. Louis, MO, U.S.A.) containing ethidium bromide. DNA was visualized by placing the gel on an UV transilluminator. The PstI RFLP located j1127 bp from the INS start site was detected in a similar manner. Primers ins01 (5hGAAGGAGGTGGGACATGT-3h) and ins02 (5hGCTGGTTCAAGGGCTTTA-3h) were used to amplify DNA [24]. Again, approximately 50 ng of DNA was added to a reaction mixture as described above. Thermal conditions required for the reaction were 95 mC for 10 min, followed by 35 cycles of 95 mC for 1 min, 55 mC for 1 min and 72 mC for 1 min, followed by a final extension of 72 mC for 10 min. PCR products were digested with 5 units of PstI (Boehringer Mannheim, Indianapolis, IN, U.S.A.) in the presence of 1ibuffer ‘ H ’ (Boehringer Mannheim) at 37 mC for 1 h. Similarly, the FokI RFLP located j1428 bp from the INS start site was detected by amplification of DNA with primers ins13 (5h-TAAAGCCCTTGAACCAGC-3h) and DS02 (5h-CAGCCCAGCCTCCTCCCTCCACA-3h) [24]. Thermal conditions required were 95 mC for 10 min, followed by 35 cycles of 95 mC for 1 min, 62 mC for 1 min and 72 mC for 1 min, followed by a final extension of 72 mC for 10 min. PCR products were digested with 5 units of FokI (Boehringer Mannheim) in the presence of 1ibuffer ‘ M ’ (Boehringer Mannheim) at 37 mC for 1 h. Digested products were electrophoresed and visualized as above. RESULTS Lack of association of the INS RFLPs with baldness Table 1 summarizes the distribution of the resulting alleles after digestion of PCR products by HphI, PstI and Male pattern baldness and the insulin gene Table 1 Distribution of INS RFLP alleles in young bald men (cases) and older non-bald men (controls) Values are n (%). A represents the uncut alleles and B represents the cut alleles. Cases Controls Hph I RFLP alleles Pst I RFLP alleles Fok I RFLP alleles A B A B A B 34 (30.4) 63 (29.4) 78 (69.6) 151 (70.6) 84 (75.0) 156 (72.9) 28 (25.0) 58 (27.1) 83 (74.1) 155 (72.4) 29 (25.9) 59 (27.6) Distribution of genotypes for each INS RFLP analysed in young bald men (cases) and older non-bald men (controls) Values are n ( %). A represents the uncut alleles and B represents the cut alleles. Table 2 Hph I RFLP genotypes Cases Controls Pst I RFLP genotypes Fok I RFLP genotypes AA AB BB AA AB BB AA AB BB 8 (14.3) 7 (6.5) 18 (32.1) 49 (45.8) 30 (53.6) 51 (47.7) 35 (62.5) 56 (52.3) 14 (25.0) 44 (41.1) 7 (12.5) 7 (6.5) 34 (60.7) 56 (52.3) 15 (26.8) 43 (40.2) 7 (12.5) 8 (7.5) FokI. No significant differences were found between cases and controls for either allele of each RFLP (HphI : χ# l 0.029, df l 1, P l 0.86 ; PstI : χ# l 0.168, df l 1, P l 0.68 ; FokI : χ# l 0.099, df l 1, P l 0.75). The possible individual genotypes for each RFLP (i.e. AA, AB or BB) were also compared in cases and controls. The distribution of genotypes is shown in Table 2. Again, no significant differences in genotypes were detected between groups (HphI : χ# l 4.33, df l 2, P l 0.11 ; PstI : χ# l 4.89, df l 2, P l 0.087 ; FokI : χ# l 3.26, df l 2, P l 0.20). Finally, we analysed haplotypes of the three INS RFLPs in cases and controls. A total of 27 different haplotypes resulting from combinations of all alleles of the three RFLPs was possible. No significant differences in haplotype distributions were demonstrated between the groups (χ# l 10.26, df l 26, P l 0.997) (results not shown). DISCUSSION We have shown that the INS gene does not appear to play a role in the aetiology of premature MPB in the general population. Our primary interest was in a polymorphism of functional relevance to INS gene expression. The INS VNTR, located within the promoter region of the INS gene, is thought to regulate insulin expression [22] and it is this region which has been linked to PCOS. In our study we utilized the HphI RFLP which is located 573 bp 3h to the VNTR. Our marker has been shown to be in very close allelic association with the INS VNTR and also in strong association with PCOS [7]. Nevertheless, our analysis showed that the distribution of alleles and genotypes relevant to the HphI RFLP was indistinguishable statistically between subjects with premature MPB and controls. Additionally, we analysed two RFLPs 3h to the INS gene (FokI and PstI) [24] to investigate the possibility of functional mutations elsewhere in the INS gene. The FokI and PstI RFLPs were in strong allelic association but were not associated with MPB in our population. Our interest in the INS gene arose because of reported genetic linkage with PCOS. PCOS is reportedly one of the most common female endocrine disorders [12], and may be expressed in males as premature MPB [9,10]. The negative findings in this study might be explained if, in our population, PCOS is not common, premature MPB is not a male phenotype of PCOS or the INS gene is not linked with PCOS. The prevalence of PCOS in the Australian population has not been reported but the generally accepted figure is 5–10 % of women of reproductive age [12]. In comparison, the overall prevalence of premature MPB in our participants was 11 %. In males, the phenotypic expression of PCOS related to hair growth includes premature baldness and excessive hairiness. In firstdegree male relatives of female cases of PCOS, 19.7 % had early baldness and\or excessive hairiness, compared with 6.5 % of first-degree male relatives of controls (P 0.01) [9]. However, when premature balding is separated from excessive hairiness, the percentage of first-degree male relatives of PCOS patients was only 11.1 %. It is possible that the earlier appearance of MPB in firstdegree relatives is secondary to high androgen levels per se rather than sharing a common pathophysiology related to the INS gene. Further independent confirmation of linkage between INS VNTR and PCOS has not yet been reported. # 1999 The Biochemical Society and the Medical Research Society 661 662 J. A. Ellis and others Interestingly, the LOD score achieved by Waterworth et al. [7] was borderline (maximum LOD score l 3.25) [25] and was observed in only 9 of 17 families. It should be noted that there are several limitations to this type of association study, such as the possibility of population stratification between the case and control groups, which we have discussed previously [5]. It is unlikely, however, that such limitations are masking an association of MPB to INS, since population stratification is normally associated with a type I, or false-positive, error. In addition, we have surveyed three separate RFLPs of the INS gene and all produce a similar result. We conclude that the gene encoding insulin does not appear to be associated with premature MPB in the general population. This does not necessarily indicate that MPB and PCOS are not in some way associated. However, given the link between the androgen and insulin pathways, and the role of insulin in hair growth cycle regulation, other genes involved in the insulin pathway may be worthy of investigation. ACKNOWLEDGMENTS We thank Dr John Hopper (Australian NHMRC Twin Registry), Dr Graham Giles (Collaborative Cohort Study, Health 2000), the general practitioners and research nurses for their contributions to subject recruitment and Angela Lamantia for her technical assistance and DNA extraction. This work was supported in part by the Victorian Health Promotion Foundation. REFERENCES 1 Hamilton, J. B. (1942) Male hormone stimulation is a prerequisite and an incitant in common baldness. Am. J. Anat. 71, 451–480 2 Hamilton, J. B. (1951) Patterned loss of hair in man : types and incidence. Ann. N.Y. Acad. Sci. 53, 708–728 3 Osborn, D. (1916) Inheritance of baldness. J. Hered. 7, 347–355 4 Kuster, W. and Happle, R. (1984) The inheritance of baldness : two B or not two B ? J. Am. Acad. Dermatol. 11, 921–926 5 Ellis, J. A., Stebbing, M. and Harrap, S. B. (1998) Genetic analysis of male pattern baldness and the 5α-reductase genes. J. Invest. Dermatol. 110, 849–853 6 Dallob, A. L., Sadick, N. S., Unger, W. et al. (1994) The effect of finasteride, a 5α-reductase inhibitor, on scalp skin testosterone and dihydrotestosterone concentrations in patients with male pattern baldness. J. Clin. Endocrinol. Metab. 79, 703–706 7 Waterworth, D. M., Bennett, S. T., Gharani, N. et al. (1997) Linkage and association of insulin gene VNTR regulatory polymorphism with polycystic ovary syndrome. Lancet 349, 986–990 8 Ferriman, D. and Purdie, A. W. (1979) The inheritance of polycystic ovarian disease and a possible relationship to premature balding. Clin. Endocrinol. 11, 291–300 9 Lunde, O., Magnus, P., Sandvik, L. and Hoglo, S. (1989) Familial clustering in the polycystic ovarian syndrome. Gynecol. Obstet. Invest. 28, 23–30 10 Carey, A. H., Chan, K. L., Short, F., White, D., Williamson, R. and Franks, S. (1993) Evidence for a single gene effect causing polycystic ovaries and male pattern baldness. Clin. Endocrinol. 38, 653–658 11 Dunaif, A., Segal, K. R., Shelly, D. R., Green, G., Dobrjansky, A. and Licholai, T. (1992) Evidence for distinctive and intrinsic defects in insulin action in polycystic ovary syndrome. Diabetes 41, 1257–1266 12 Dunaif, A. (1995) Hyperandrogenic anovulation (PCOS) : a unique disorder of insulin action associated with an increased risk of non-insulin-dependent diabetes mellitus. Am. J. Med. 98 (Suppl. 1A), 33S–39S 13 Norman, R. J., Masters, S. and Hague, W. (1996) Hyperinsulinemia is common in family members of women with polycystic ovary syndrome. Fertil. Steril. 66, 942–947 14 Pasquali, R., Casimirri, F., De Iasio, R. et al. (1995) Insulin regulates testosterone and sex hormone-binding globulin concentrations in adult normal weight and obese men. J. Clin. Endocrinol. Metab. 80, 654–658 15 Birkeland, K. I., Hanssen, K. F., Torjesen, P. A. and Vaaler, S. (1993) Level of sex hormone-binding globulin is positively correlated with insulin sensitivity in men with type 2 diabetes. J. Clin. Endocrinol. Metab. 76, 275–278 16 Ebeling, P., Stenman, U.-H., Seppala, M. and Koivisto, V. A. (1995) Acute hyperinsulinemia, androgen homeostasis and insulin sensitivity in healthy man. J. Endocrinol. 146, 63–69 17 Ibanez, L., Potau, N., Georgopoulos, N., Prat, N., Gussinye, M. and Carrascosa, A. (1995) Growth hormone, insulin-like growth factor-I axis, and insulin secretion in hyperandrogenic adolescents. Fertil. Steril. 64, 1113–1119 18 Haffner, S. M., Shaten, J., Stern, M. P., Smith, G. D. and Kuller, L. (1996) Low levels of sex hormone-binding globulin and testosterone predict the development of noninsulin-dependent diabetes mellitus in men. Am. J. Epidemiol. 143, 889–897 19 Katsuki, A., Sumida, Y., Murashima, S. et al. (1996) Acute and chronic regulation of serum sex hormone-binding globulin levels by plasma insulin concentrations in male non-insulin-dependent diabetes mellitus patients. J. Clin. Endocrinol. Metab. 81, 2515–2519 20 Pasquali, R., Macor, C., Vicennati, V. et al. (1997) Effects of acute hyperinsulinemia on testosterone serum concentrations in adult obese and normal-weight men. Metabolism 46, 526–529 21 Philpott, M. P., Sanders, D., Westgate, G. E. and Kealey, T. (1994) Human hair growth in vitro : a model for the study of hair follicle biology. J. Dermatol. Sci. 7 (Suppl.), S55–S72 22 Kennedy, G. C., German, M. S. and Rutter, W. J. (1995) The minisatellite in the diabetes susceptibility locus IDDM2 regulates insulin transcription. Nat. Genet. 9, 293–298 23 Norwood, O. T. (1975) Male pattern baldness : classification and incidence. South Med. J. 68, 1359–1365 24 Julier, C., Hyer, R. N., Davies, J. et al. (1991) InsulinIGF2 region on chromosome 11p encodes a gene implicated in HLA-DR4-dependent diabetes susceptibility. Nature (London) 354, 155–159 25 Lander, E. and Kruglyak, L. (1995) Genetic dissection of complex traits : guidelines for interpreting and reporting linkage results. Nat. Genet. 11, 241–247 Received 4 January 1999/12 March 1999; accepted 19 March 1999 # 1999 The Biochemical Society and the Medical Research Society