Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Genome evolution wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Genomic imprinting wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Tay–Sachs disease wikipedia , lookup
Medical genetics wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Frameshift mutation wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Public health genomics wikipedia , lookup
Gene expression programming wikipedia , lookup
Saethre–Chotzen syndrome wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Designer baby wikipedia , lookup
Skewed X-inactivation wikipedia , lookup
Y chromosome wikipedia , lookup
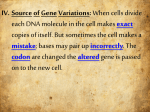
Point mutation wikipedia , lookup
Microevolution wikipedia , lookup
Genome (book) wikipedia , lookup
X-inactivation wikipedia , lookup
BHS 116: Physiology Notetaker: Stephanie Cullen Date: 10/16/12, 1st hour Page: 1 Clicker Question: Which genotype below would you expect to see in a person suffering from a glycogen storage disease? a. Heterozygous b. Homozygous recessive - Have to have both mutant copies c. Homozygous dominant Lecture 34- Genetic Principles and Diseases (continued) Cystic Fibrosis - Most common lethal genetic disorder affecting Caucasians - Carrier frequency of 1 in 25-30 o 1 mutant copy o Can pass it along to offspring genetically if mate with another carrier o Does not have the disease - 2-4% of population are heterozygotes and asymptomatic - Disorder of epithelial transport affecting the secretory process of all exocrine glands and the epithelial lining of all respiratory, GI, and reproductive systems o Exocrine gland secretion is the biggest problem with CF o Epithelial lining of the respiratory tract and GI tract are primarily affected (not as much in the reproductive tract) - A high level of NaCl in the sweat is a consistent and characteristic biochemical abnormality in CF o A proper sweat test is crucial for diagnosis - CF results in production of abnormally thick and sticky mucous in these transport systems leading to chronic lung disease, pancreatic insufficiency, steattorrhea, malnutrition, hepatic cirrhosis, intestinal obstruction, and male infertility o Mucus in respiratory tract = problems breathing and increase infection since the mucus prevents getting rid of infectious agent o Can’t properly digest food to produce amino acids, fatty acids, and carbohydrates the body uses (malnutrition) o The 2 listed directly above are the most dangerous of the possible symptoms - Primary defect in CF results from abnormal function of an epithelial cAMP-dependent chloride channel protein that sits in the epithelial plasma membrane o Encoded for by the CF transmembrane conductance regulator (CFTR) gene on chromosome 7 o Over 800 different mutations that can occur in this one gene that produces CF Not a single mutation to look for o Most common is ∆F-508: deletion (∆ means missing) of 3 nucleotides coding for phenylalanine (F) at position 508 - 6 classes of mutations based on how they affect the gene product: o Class I: defective protein synthesis No normal protein made o Class II: abnormal protein folding, processing, and trafficking (∆F-508) BHS 116: Physiology Notetaker: Stephanie Cullen - - Date: 10/16/12, 1st hour Page: 2 Post-translational problem (occurring after the synthesis process) ∆F-508: synthesized but doesn’t always make it to the membrane o Class III: defective regulation Couple different regulation sites on a protein R (regulatory) domain o Mutated so that the channel can’t function properly Nucleotide binding domain (ATP-dependant chloride channel) o ATP binding site could be mutated so that ATP can’t bind o Class IV: decreased conductance Something improper in the final protein product doesn’t allow for normal flow of Cl through the channel o Class V: reduced abundance Some of the normal channel is produced but not all of it Reduced Cl flow o Class VI: altered regulation of separate ion channels (∆F-508) Affecting another channel/protein CFTR has influence on epithelial-Na channel (ENaC) Mutation isn’t in the ENaC itself but in the CFTR but altered effect of CFTR affects the ENaC functioning Symptoms can manifest themselves from mild to severe depending on the type of mutation o First 3 classes are severe- not producing much of any functional protein whatsoever Number of problems (lungs and pancreas) Correlates to a very positive sweat test More severe = more NaCl in sweat o Classes IV and V are more mild- produce some functional protein (just not the normal amount) so do get some chloride conductance Less severe symptoms Less NaCl in sweat Treatments o Antibiotics High degree of infection in lungs because mucus is preventing expectoration of bacteria o Corticosteroids Reduce inflammation o Mucolytic drugs Help break up the mucus so it can be expectorated o Gene therapy (on the horizon) Insert a normal CFTR in patient so they can have at least some normal functioning CFTR channel BHS 116: Physiology Notetaker: Stephanie Cullen Date: 10/16/12, 1st hour Page: 3 CF Effect on Sweat and Mucus - CFTR channel has different effects in different tissues - Functions of CFTR are tissue specific o Could be inward movement of Cl Cells on luminal surface of sweat ducts take in Cl Normally when sweat is produced in the sweat glands, it is moving up through the sweat duct so that these cells can take up the Cl ENaC inward movement of Na Absorbing NaCl from the sweat before it gets to surface o Could be outward movement of Cl - Impact of a mutation in CFTR will also be tissue specific (as in CF) o No absorption of Cl or Na because it affects ENaC Sweat has high concentrations of NaCl o In airway epithelium, normal function of CFTR is outward movement of Cl From inside to lumen of respiratory tract Get corresponding inward movement of Na into cell followed by water o With CF defect, no longer get outward movement Causes a hyperstimulation of ENaC Get even more Na into the cell (and more water following Na) Dehydrates mucus lining respiratory tract Pulling water out of mucus Leads to a sticky, viscous mucus lining respiratory tract o Hard to get rid of and expectorate Lung with CF (whole lungs) - Excessive mucus plugs and dilation of the bronchial tree (bronchiectasis) o Bacterial infections - Pneumonia: bacteria can propagate and can’t get expectorated Lung with CF (histological section) - Exocrine - Pancreatic ducts are dilated and plugged with mucin o Normally have very small lumens o Mucus expands them - Parenchymal glands are atrophic and replaced with fibrous tissue o Normally produce enzymes o Can’t get through to GI tract o Glandular portion shrivels up - Overall decrease in functionality of pancreas BHS 116: Physiology Notetaker: Stephanie Cullen Date: 10/16/12, 1st hour Page: 4 Ehlers-Danlos Syndromes - Autosomal recessive and dominant syndromes characterized by defects in collagen synthesis or structure - Skin, ligament, and joints are frequently involved in all forms (primary targets due to collagen presence) o Hyperextensible and fragile skin and hypermobile joints Skin is highly susceptible to trauma Joints are vulnerable to dislocation - Serious internal complications o Rupture of the colon and large arteries (vascular EDS) o Ocular fragility that could result in corneal rupture and retinal detachment - 6 different forms o Vascular form (IV): most life threatening as large vessels are susceptible to rupture Aorta rupture is a possibility Autosomal dominant Affects collagen gene directly (mutation in gene itself) o Kyphoscoliosis form (VI): most eye-relevant Autosomal recessive Need 2 mutant copies of gene Lysyl hydroxylase: enzyme involved in post-translational modification of collagen o Don’t get normal collagen fibers forming if mutated Corneal problems, retinal detachment problems X-linked Recessive Disorders - Almost all x-linked diseases are recessive o Females have 2 X chromosomes Need both to be mutant to express the disease If she has 1 mutant X, she is a carrier o Males have 1 X and 1 Y If he has 1 mutant X, he will have the disease because the Y can’t help compensate for it - All sex-linked disorders are x-linked - These disorders are transmitted by heterozygous females primarily to sons who are then hemizygous - Heterozygous females rarely express the full phenotype - Afflicted males don’t transmit to sons but all daughters are carriers o Pass Y on to sons and X to daughters - Sons of heterozygous mothers (carrier) have a 1 in 2 chance of receiving the mutant gene o Daughters could end up being carrier o Sons could end up with disease BHS 116: Physiology Notetaker: Stephanie Cullen - Date: 10/16/12, 1st hour Page: 5 o Mother would have to be a carrier and father would have to be affected to get an affected daughter (extremely rare) If the father is affected, his sons are all unaffected; however his daughters are all carriers Objective: Describe the different X-linked diseases and their pathogenesis (hemophelia, fragile X syndrome). Hemophelia A - Queen Victoria: carrier (1 mutant X) o 1 son had hemophelia o 2 daughters were carriers o Other children were unaffected - Queen Victoria’s daughter, Alice (a carrier) passed disease to her children o 2 carrier daughters o 1 son with hemophelia o Other children were unaffected - 1 of Alice’s carrier daughters married Tsar Nicholas o 4 normal daughters o 1 son (Alexis) with hemophelia - Hereditary disease associated with serious bleeding - Caused by a reduced amount or reduced activity of Factor VIII, an important clotting factor (in clotting cascade) - It occurs in males with a mutant copy or homozygous females (2 mutant copies) - Clinical symptoms develop only in the presence of severe deficiency (<1% factor VIII activity) o Don’t need a lot of enzyme activity in clotting cascade Little bit of enzyme goes a long way o Have to pretty much knock out all of Factor VIII (>99%) to get symptoms - Mild (1-5% activity) to moderate (5-75% activity) deficiencies are usually asymptomatic - In all symptomatic cases there is a tendency toward easy bruising and massive hemorrhage after trauma or surgery o Can bruise from just touching the skin o Once bleeding starts, it won’t stop because missing part of clotting cascade (platelet plug won’t hold) - Spontaneous bleeding into the joints can occur (hemarthroses) o Can lead to progressive deformities that may be crippling o Very restrictive due to build of proteins in the joints - Treatment: infusion of Factor VIII prepared from human plasma or recombinant forms o Now use recombinant Factor VIII primarily o Before 1985 thousands of hemophiliacs received HIV contaminated blood and later developed AIDS BHS 116: Physiology Notetaker: Stephanie Cullen Date: 10/16/12, 1st hour Page: 6 Fragile X Syndrome - Prototype disease in which there is a long repeating trinucleotide sequence - Non-Mendelian single gene disorder o Can have a permutation o Huntington’s: varying stages of the disease until you get to that certain number of repeats where disease actually occurs Can have more than normal without actually having the disease - In most of the cases, the affected sequences share guanosine (G) and cytosine (C) nucleotides in the trinucleotide repeat o CGG repeat - 2nd most common cause of mental retardation after Down Syndrome - - Characterized by an inducible abnormality in the X chromosome and an unusual mutation within the familial mental retardation-1 (FMR-1) gene o Results in loss of function of the FMR protein due to the excess CGG trinucleotides mRNA transporter o Decreased translation of specific neuronal mRNAs Decreased neuronal maturation Decreased connections leading to the mental retardation During chromosome staining analysis, the chromosome appears broken at a site called the fragile site (thus the name) Affected males have an IQ of 20-60 Carrier males are those that carry the mutation (a premutation), but are asymptomatic (20%)- do have some trinucleotide repeats but not enough to cause a full mutation o Can transmit the disease to their grandson through their phenotypically normal daughter where the permutation is converted to a full mutation during oogenesis (doesn’t occur in spermatogenesis) More tinucleotide repeats are produced during oogenesis She is fine but develops the full mutation in her eggs to pass to her sons Can also pass to daughter but she will only be a carrier (not affected) o Can’t pass to sons at all Objective: Describe cytogenetic disorders and the diseases associated with them. Cytogenetic (Chromosomal) Disorders - Numerous chromosomal abnormalities that occur during cell division - Estimated that 1 in 200 newborns has some form of chromosomal abnormality BHS 116: Physiology Notetaker: Stephanie Cullen - Date: 10/16/12, 1st hour Page: 7 50% of 1st trimester miscarriages are due to chromosomal abnormalities o Just not compatible with life Disorders can result from alterations in the number or structure of chromosomes and can effect autosomal or sex chromosomes (X or Y) Normal Karyotype - Karyotype: photographic representation of the chromosomes in metaphase - Stained with Giemsa stain and thus have patterns of G banding - Arranged in order of decreasing length o Chromosome 1 is the longest o Chromosome 22 is the shortest - In the normal condition, each chromosome is paired (diploid) o Haploid = n (1 of each chromosome) = 23 o Diploid = 2n (2 of each chromosome) = 46 - The normal number of chromosomes if 46 (23x2) o Get one of each from each parent o 22 pairs of autosomes o 1 pair of sex chromosomes Objective: Describe aneuploidy vs polyploidy. Polyploidy - Error in meiosis resulting in an extra complete set of chromosomes - Can be triple or quadruple chromosomes (3n or 4n) o Have it from one parent: triploidy o Have it from both parents (very rare): quadraploidy (4 copies) - Generally results in spontaneous abortion - Triploid o Accounts for 17% of all spontaneous abortions Completely incompatible with life o Accounts for 3% of all stillbirths Aneuploidy - Having an extra or missing single or multiple chromosomes (any number of chromosomes that is not a multiple of n) - Down Syndrome (Trisomy 21) o 3 copies of chromosome 21 - Due to an error in meiosis called nondisjunction o Pair of chromosomes fails to separate during meiosis o 1 of the daughter cells get both chromosomes while other daughter cell gets none - 50% of spontaneous abortions are caused by an extra or missing chromosome Surviving Autosomal Aneuploids - Trisomy 8 - Trisomy 9 - Trisomy 13 “Patau syndrome” BHS 116: Physiology Notetaker: Stephanie Cullen - Date: 10/16/12, 1st hour Page: 8 Trisomy 18 “Edward syndrome” Trisomy 21 “Down syndrome” Trisomy 22 Down Syndrome - Most common chromosomal disorder - Leading cause of mental retardation o Retardation is severe (IQ of 25-50) - Alzheimer disease after 40 years old (early onset) o Normally don’t see until 70s - Congenital heart defects in 40% (PSDs, VSDs, ASDs) - Maternal age has a strong influence on the incidence of this disease - Occurs in 1 in 1550 live births of mothers younger than 20 - Occurs in 1 in 25 live births in mothers over 45- Much higher frequency as mother ages - Maternal age factor suggests that nondisjunction occurs in ovum Sex-Linked Cytogenetic Disorders - Turner syndrome (single-X or structural abnormalities of one of the X chromosomes) o Occurs in females o 57% are the single X condition which has the most affects: Amenorrhea: loss of menstrual cycle Infertility Short stature Coarctation of aorta (narrowing) causing heart problems o One normal X and one abnormal X form: Only amenorrhea is a common affect Almost normal appearance Fertility is not an issue - Klinefelter syndrome (XXY) o 1 in 500 males Objective: Describe the various chromosomal structural abnormalities and mitochondrial gene mutations. Chromosome Structural Abnormalities - Translocations - Deletions - Inversion - Isochromosomes - Ring Chromosomes - Gene Duplications Translocations - Occurs between 2 chromosomes - Balanced reciprocal translocation o Broken fragments in each chromosome are exchanged BHS 116: Physiology Notetaker: Stephanie Cullen - Date: 10/16/12, 1st hour Page: 9 o Not harmful to the carrier, but abnormal gametes are formed resulting in abnormal zygotes (carrier has 46 chromosomes) Robertsonian translocation o Breaks occur close to centromere in each chromosome 2 long arms join resulting in 1 very long chromosome 2 short arms join resulting in 1 very short chromosome which is useless and lost o Carrier has 45 chromosomes o Compatible with survival because short arms contain ribosomal RNA which is in abundance elsewhere on the chromosome (not really necessary) o Abnormalities arise in gametogenesis (again doesn’t affect carrier since have the full complement of genes) Deletions - Loss of a portion of the chromosome - A single break may result in the loss of a terminal segment - 2 interstitial breaks with fusion of the 2 ends results in the loss of an internal fragment - Isolated fragment does not have a centromere and is lost o Results in a loss of genetic material - Can produce severe consequences to the carrier or offspring depending on where the break occurs and what genetic material it is carrying Inversions - Occur when there are 2 interstitial breaks in a chromosome and the segment reunites after a complete turn around - Paracentric inversion: only 1 chromosome arm o Same genes are in there just not in original sequence o Carrier and offspring ok - Pericentric inversion: both arms o On each end of centromere o Spins around the centromere - Compatible with normal development o Not losing any genetic material- just flipping the regions around Isochromosomes - Normally, have a vertical division to yield a long arm and a short arm - Results when the centromere divides horizontally instead of vertically - 1 of the 2 arms is lost and the remaining arm is duplicated resulting in a chromosome with only 2 short arms or only 2 long arms - Fine in carrier because all genetic material is there - Offspring would be missing some material when getting either the 2 short arms or 2 long arms Ring Chromosomes - Single chromosome involved - Variation in which the ends are deleted and the arms unite to form a ring BHS 116: Physiology Notetaker: Stephanie Cullen - Date: 10/16/12, 1st hour Page: 10 o 2 fragments are lost These chromosomes do not behave normally in meiosis or mitosis o Can result in serious consequences o Will affect carrier o Can’t be passed to offspring Duplication of Genes - Results in lengthening of 1 or both chromosome arms - Usually no effect on health of carrier or offspring o Deletions are much more dangerous (better to have more genetic material than missing genetic material) Mitochondrial Gene Mutations - Mitochondrial DNA (mtDNA) is inherited from the mother only - Due to the fact that the ovum is a full cell and contains an abundance of mitochondria while the head of the spermatozoa does not o Only get nuclei from spermatozoa - Mothers transmit mtDNA to all of their offspring, but only the daughters can transmit mtDNA to their progeny - mtDNA encodes 37 genes o 24 encode translational proteins involved in translating the genes into proteins o 13 encode enzymes involved in oxidative phosphorylation (ATP production) Though very rare, mutations can be very serious Tend to affect neuromuscular system - Leber Hereditary Optic Neuropathy o If male has mutation, none of offspring (or grandchildren) have the mutation o If female has mutation, all of the offspring have it but only the daughters can pass it on to her children (not sons) o Neurodegenerative disease progressing to bilateral loss of central vision Degeneration of retinal ganglion cells o Visual impairment is noticed between 15-35 years old o Leads to blindness