Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Monoclonal antibody wikipedia , lookup
Rheumatic fever wikipedia , lookup
Immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Sjögren syndrome wikipedia , lookup
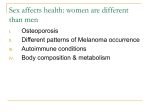
657 Dendritic cells in autoimmune diseases Burkhard Ludewig, Tobias Junt, Hans Hengartner and Rolf M Zinkernagel Subclinical autoimmune responses can be frequently detected in healthy individuals. Sustained activation of autoreactive lymphocytes is, however, required for the development of autoimmune diseases associated with ongoing tissue destruction either in single organs or generalized with multiple manifestations. Clinical and experimental evidence suggests that prolonged presentation of self antigens by dendritic cells is crucial for the development of destructive autoimmune disease. We discuss here a simplified threshold model where the key parameters for the magnitude of the autoimmune response are the amount of previously ignored self peptides presented by dendritic cells and the duration of the antigen presentation in secondary lymphoid organs. Multiple factors influence the threshold for the conversion of an autoimmune response to overt autoimmune disease. Frequent or persistent viral infections of the target organ may favor autoimmune disease by increasing the amounts of released self antigens, generating cytokine-mediated bystander activation of selfreactive lymphocytes and/or sustaining a chronic response via neoformation of lymphoid structures in the target organ. Addresses Institute of Experimental Immunology, Department of Pathology, University of Zürich, Schmelzbergstrasse 12, CH-8091 Zürich, Switzerland Correspondence: Burkhard Ludewig; e-mail: [email protected] against self antigens are sustained. It is therefore important to delineate the mechanisms leading to, and the thresholds influencing, the initial activation of self-reactive lymphocytes and the sustenance of the autoimmune response. Both genetic and environmental components determine the susceptibility to autoimmune diseases. Genetic alterations may influence the general immunoreactivity of the host. Particularly, polymorphism in genes influencing lymphocyte homeostasis may increase the susceptibility to autoimmune disease. However, a large body of evidence shows that the onset of autoimmune diseases is strongly associated with viral or bacterial infections [1]. Epidemiological studies revealed the link between infectious environmental factors and autoimmune diseases such as multiple sclerosis (MS) and insulin-dependent diabetes mellitus (IDDM) [2]. Virus infections, for example, can be the initial trigger for an autoimmune response [3] and/or contribute to the chronicity of autoimmune processes [4]. Alternatively, immune responses against unknown or as-yet unidentified viruses may appear as auto-immunity when the immune system targets mainly viral antigens. It is therefore important to discriminate between genuine autoimmune responses directed against self-antigens and immune responses directed against persisting viral antigens that often mimic autoimmune tissue destruction, but that are in fact virus-induced immunopathology. Current Opinion in Immunology 2001, 13:657–662 0952-7915/01/$ — see front matter © 2001 Elsevier Science Ltd. All rights reserved. Abbreviations APC antigen-presenting cell CTL cytotoxic T lymphocyte DC dendritic cell GP glycoprotein IDDM insulin-dependent diabetes mellitus LCMV lymphocytic choriomeningitis virus mOVA murine ovalbumin RIP rat insulin promotor Introduction Autoimmune responses can arise because the repertoire of both T- and B-cell receptors, which allows recognition of pathogens, may contain receptors recognizing self components. An important mechanism to reduce the numbers of autoreactive lymphocytes is the elimination of self-reactive T cells in the thymus and the deletion of B cells reacting with self-determinants expressed on cellular surfaces in the bone marrow. However, a great number of self-reactive lymphocytes escape these central negative-selection processes and form a peripheral pool of potentially autoimmune-disease-mediating lymphocytes. Destruction of self tissue may lead to release of self antigens and subsequent activation of transient autoimmune responses. However, the pathological consequences of autoimmunity only become manifest when autoimmune responses directed Genuine autoimmune reactions are most likely to be initiated in the course of an infection when target-tissue inflammation is provoked either by direct cytopathic effects or by immunopathological reactions against a persisting microbial agent. Infection-associated inflammation, for example, involves the release of cytokines and chemokines, which attract antiviral effector cells and lymphocytes of other specificities. This ‘bystander effect’ can be sufficient to activate both lymphocytes directed against self antigens [5] and lymphocytes directed against non-related determinants [6], leading to initiation and/or exacerbation of autoimmune disease. A second mechanism that may lead to the initiation of autoimmunity in the course of an infection is the activation of T or B cells via antigenic determinants shared between the pathogen and the host; this has been termed ‘molecular mimicry’ [7]. Cross-reactivities between pathogen-derived and self antigens have been described for human autoimmune diseases such as IDDM [8], MS [9] and Guillain−Barre syndrome [10]. In the situation of molecular mimicry, the trigger for autoimmunity would be eliminated when the pathogen is cleared; recurrent infections could elicit chronic relapsing autoimmune disease. Pathogens frequently enter the body via peripheral tissues and pathogen-derived antigens may reach local secondary lymphoid tissues after encounter with dendritic cells (DCs) [11]. During migration to secondary lymphoid organs and 658 Autoimmunity Figure 1 Number of DCs loaded with antigenic peptides Mechanisms increasing the threshold for autoimmune disease Autoimmune disease Threshold • High regenerative capacity of target organ • Low T cell precursor frequency • Low cross-presentation efficacy • Elimination of DCs by effector T cells Mechanisms decreasing the threshold for autoimmune disease Autoimmune response Duration of self-antigen presention by DCs (weeks, months) • Infections in target organ (bystander cytokines) • Shared antigenic determinants (molecular mimicry) • Formation of lymphoid structures in target organ • T cells with high affinity for self antigens • Genetic predisposition Schematic representation of a simplified threshold model for the induction of autoimmune diseases. The duration of selfantigen presentation by DCs (x) and the number of DCs loaded with antigenic selfpeptides (y) are the key factors determining the strength of an autoimmune response. Presentation of previously immunologically ignored self-antigens by DCs results generally in an autoimmune response. Autoimmune disease, however, develops only if selfreactive T cells are activated by sustained presentation of self-peptides by DCs. Thresholds for the conversion of autoimmune responses to autoimmune disease are usually maintained at high levels by various mechanisms (green arrows; examples of these mechanisms are shown), but may be lowered dramatically (red arrows), for example by persistent infection of the target organ. Current Opinion in Immunology specific homing to T cell areas, DCs upregulate their T-cell-stimulatory properties and function as efficient activators of naïve T cells. Thus, translocation of live pathogens and/or pathogen-derived antigens to secondary lymphoid organs by DCs is most likely to be a key event for the initiation of immune responses against the pathogen and, under certain circumstances, also for the induction of autoimmune sequelae. Accordingly, acquisition of self antigens by DCs and their subsequent presentation to self-reactive lymphocytes crucially contributes to both the initiation and the maintenance of autoimmune responses. We will discuss here the role of DCs in the induction of autoimmune responses and review the recent literature addressing the function of DCs in the pathogenesis of autoimmune diseases. General rules for T cell mediated immune reactivity A number of theories have been put forward to explain how self-reactive lymphocytes become activated and mediate autoimmune diseases; such theories include the involvement of the idiotypic network and suppressor and/or regulatory cells, and cytokine imbalances. Recently, Roncarolo et al. [12] suggested that DCs may be involved in the counter-regulation of potential autoimmune T cell responses. The general motif of these theories is that, once an anti-self response is initiated, negative regulatory mechanisms are required to avoid pathogenic T cell reactions and that autoimmunity is a deviation of normal immune reactivity. Before discussing the specific role of DCs in autoimmune diseases, we should therefore outline the critical parameters for the induction of normal T cell responses, such as the amount and localization of antigen, the quality and duration of antigen presentation, and the tolerance status of the lymphocytes. T cells recognize antigenic peptides in the context of selfMHC and are activated exclusively in secondary lymphoid organs [13]. For the initiation of T cell responses, antigen has to reach lymphoid organs and be presented therein by professional antigen-presenting cells (APCs). It is important that antigens are presented first in a localized fashion before systemic spread occurs in order to avoid exhaustive tolerizing immune responses [14,15]. Likewise, antigen should be present in local lymphoid organs for a minimal time period (probably 4–6 days) to obtain optimal initial activation of T cells. Only T cells that have not been negatively selected in the thymus and are of sufficiently high avidity possess the capacity to elicit autoimmune reactions. These autoreactive T cells are usually directed against immunologically ignored antigens, which are not presented in the thymus or in peripheral lymphoid tissues such as lymph nodes or spleen. Autoreactive T cells recognizing immunologically ignored antigens are usually only activated if their cognate antigen reaches lymphoid organs and is appropriately presented by professional APCs. The repertoire of autoreactive T cells that are not negatively selected in the thymus is extensive, as can be easily demonstrated by administering autoantigens or their immunogenic peptides mixed with strong adjuvants. It is important to note that self-reactive T cells can be activated not only by using sequestered antigens such as myelin basic protein (MBP) or proteolipid protein (PLP), but also by using highly abundant proteins such as collagen type II (found in joints), cardiac myosin, thyroglobin or melanocyte antigens. Similarly, activated autoreactive T cells that recognize widely distributed proteins such as rhesus polypeptides [16] or platelet glycoprotein (GP)IIB−GPIIIa [17] can be found in patients with autoimmune hemolytic anemia or autoimmune thrombocytopenia purpura, respectively. Dendritic cells in autoimmune diseases Ludewig et al. 659 Taken together, the evidence is compelling that the above-mentioned negative regulatory mechanisms — if they exist — are easily over-ruled and that autoimmunity can be induced when immunologically ignored autoantigens are presented in secondary lymphoid organs above a minimal concentration for a sufficient length of time. Therefore, it is conceivable that the default pathway of immune reactivity after loading of previously immunologically ignored autoantigens onto DCs is activation. Accordingly, presentation of autoantigens by DCs to high-avidity self-reactive T cells results generally in autoimmunity. The main parameters for the strength of an autoimmune response and the conversion of an autoimmune reaction into clinically manifest autoimmune disease are the number of DCs presenting self-antigen and the duration of self-antigen presentation by DCs (Figure 1). Importantly, in genetically non-predisposed individuals, the thresholds for shifting autoimmunity to overt autoimmune disease are generally maintained at high levels by mechanisms such as low T cell precursor frequencies, low efficacy of cross-presentation and elimination of DCs by effector T cells (Figure 1). right heart and in arterial smooth-muscle cells [27]. Despite the widespread expression of the transgene in the vascular system, T cells ignore the peripherally expressed antigen but immunization with DCs presenting β-galactosidase peptide elicited cardiovascular immunopathology [28]. Repeated application of peptide-pulsed DCs was required to induce the most severe phenotype of this experimental disease — with arteritis, myocarditis and dilated cardiomyopathy. A less severe, and transient, cardiovascular inflammation was induced when DCs pulsed with β-galactosidase peptide were administered less frequently or in lower numbers (B Ludewig, unpublished data). Considering that DCs have only a short half-life in secondary lymphoid organs [29], particularly in the presence of activated T cells that recognize peptides presented by DCs [29–31], it appears that the continuous replenishment of the DC pool presenting a certain peptide is crucial for the maintenance of T cell activity. In situations where T cell precursor frequencies are low, such as in RIP−GP or SM−LacZ mice, prolonged antigen delivery via DCs is the crucial factor for the conversion from transient autoimmunity to manifest autoimmune disease. Triggering autoimmunity with dendritic cells The usually low frequency (10−5) of self-reactive T cell precursors sets high thresholds for the induction of autoimmune disease. RIP−GP mice, for example, do not develop diabetes after infection with LCMV-GP-recombinant vaccinia virus [26]. However, elevation of CTL precursor frequencies in double-transgenic mice expressing the LCMV-GP in the pancreas and a GP-specific TCR on their CTLs (i.e. RIP−GP x TCR mice) leads to the rapid induction of diabetes after infection with vaccinia virus expressing recombinant LCMVGP [26]. Similarly, elevation of organ-specific T helper cell frequencies using TCR-transgenic models converts DC-induced autoimmune responses to severe autoimmune disease [24,25•]. The importance of controlled proliferation and apoptosis of self-reactive lymphocytes becomes obvious in patients with mutations in Fas or Fas-ligand genes or in autoimmune lymphoproliferative syndrome [32], where high frequencies of self-reactive T cells and their activation may be the cause of systemic autoimmune disease. A number of studies in human autoimmune disorders have indicated that DCs can be found in autoimmune lesions [18,19]. In addition, animal models of spontaneous autoimmune disease have shown that DCs are amongst the first cells to infiltrate the target tissue [20] and are capable of presenting autoantigens to T cells in local draining lymph nodes [21]. The potency of DCs in priming autoreactive T cells that precipitate an autoimmune disease has been shown in a seminal study by Knight et al. [22] using adoptive transfer of thyroglobulin-loaded DCs into genetically susceptible mice. Furthermore, DCs expressing endogenous self-peptides or pulsed ex vivo with immunogenic selfpeptides can induce severe autoimmune disease [23,24,25•]. Mice transgenic for the rat insulin promotor (RIP) and lymphocytic choriomeningitis virus (LCMV) GP (i.e. the RIP−GP model of IDDM) [26] were used to investigate the potential of DCs to induce autoimmune diabetes. RIP−GP mice express the transgene exclusively in pancreatic-islet β-cells; T cells ignore the neoself-antigen until LCMV-GPspecific cytotoxic T lymphocytes (CTLs) are activated either by LCMV infection or by immunization using DCs presenting the immunodominant LCMV-GP epitope endogenously (these cells are termed H8-DC) [23]. Single immunization of RIP−GP mice with H8-DC resulted in transient CTL activation and recruitment of islet-specific CTLs but did not lead to diabetic disease. CTL activity had to be maintained over a period of 10–12 days by repeated H8−DC injections to shift the balance to a more severe phenotype with an incidence of diabetes of >90% [23]. Similar results were obtained in the SM−LacZ model of autoimmune arteritis and myocarditis. These transgenic mice express the β-galactosidase antigen under the control of a smooth-muscle-specific promotor in cardiomyocytes of the A further factor determining the susceptibility to autoimmune disease is the regenerational capacity of the target organ, as demonstrated in the SM−LacZ model of DC-induced cardiovascular immunopathology. As mentioned above, repetitive priming of SM−LacZ mice with DCs presenting β-galactosidase peptide caused acute vascular immunopathology with strong lymphocytic infiltration in lung arteries and in the right heart. Interestingly, cessation of chronic self-antigen delivery by DCs to secondary lymphoid organs after 10–12 days resulted in resolution of the arterial lesions in the lung arteries with only mild histiocytic infiltrates around the vessels, indicating the high capacity of the arterial wall to regenerate after inflammatory injuries. However, in this chronic phase, despite cessation of immunization with β-galactosidase-loaded DCs, SM−LacZ mice showed a severe loss of the poorly regenerating heart tissue and showed fibrosis that eventually led to dilated cardiomyopathy [33•]. Taken together, these results 660 Autoimmunity show that autoimmune damage may resolve if an antigen is no longer presented in lymphoid tissues and that the susceptibility of an organ for autoimmune diseases critically depends on the ability to replace damaged tissue with new functional tissue. Antigen persistence and chronic inflammation Previously ignored, peripheral self-antigens that are released, for example, in the course of infection-induced inflammatory reactions can reach secondary lymphoid organs either via lymph transport or in association with DCs. Since DCs are excellently equipped to process and present exogenous antigens via MHC class II [34], induction of T helper cell responses against self antigen is probably very efficient. It has been suggested that DCs may also process exogenous self antigens via MHC class I for presentation to CTLs, leading to induction of autoimmune disease via a pathway called cross-presentation [35]. Exogenous loading of MHC class I molecules on DCs can be achieved using soluble [36] or cell-associated proteins [37] and can be further enhanced if proteins form immune complexes with antibodies [38]. However, careful titration of exogenous antigen shows that large amounts of protein are required to achieve cross-presentation [36]. Cross-presentation can also be demonstrated in vivo using transgenic mice expressing model antigens in peripheral non-lymphoid tissues [39,40]. In mice transgenic for RIP−mOVA (murine ovalbumin), for example, the widely and highly expressed ‘self’-antigen is presented via MHC class I in draining secondary lymphoid organs by bonemarrow-derived APCs [39]. Brocker and colleagues [41•] have shown that antigen presentation by DCs is sufficient for cross-presentation in this model system. However, spontaneous autoimmune disease that is mediated by cross-presentation in ‘high expresser’ situations, such as RIP−mOVA mice, is only elicited when central tolerance mechanisms are bypassed by transfer of large numbers of naïve TCR-transgenic CTLs [42]. In contrast, when self antigens are expressed at lower concentrations, and in a more localized fashion, spontaneous autoimmune disease does not occur, even in the presence of elevated levels of self-reactive T cells [26,43]. Thus, self-perpetuating autoimmunity due to cross-presentation is most likely to be a phenomenon that is restricted to engineered transgenic models where central tolerance mechanisms can be bypassed and/or T cell frequencies are artificially high. Furthermore, cross-presentation of cellassociated proteins in vivo appears to be a rather inefficient process, because only a very small percentage of the CD8α– lymphoid-DC subset cross-presented OVA, even if large quantities of OVA protein were accessible for DCs [44•]. reduced the incidence of autoimmune diabetes [25•]. In addition, not even a minimal autoimmune response was induced when large amounts of self-antigen in the form of apoptotic or necrotic LCMV-GP-expressing fibroblasts were injected. Only in the presence of high numbers of specific TCR-transgenic T helper cells or in the presence of non-specific immunostimulatory stimuli did a mild autoimmune response develop after injection of necrotic LCMV-GP-expressing fibroblasts [25•]. In addition, Ochsenbein et al. [45••] have shown recently that cross-presentation of tumor antigens is inefficient and, if at all feasible — in terms of antigen quantities — a very demanding process. Thus, high threshold levels for presentation of exogenous self-antigens via MHC class I on DCs are most likely to be a key mechanism in preventing selfperpetuating autoimmune disease and making the successful induction of anti-tumor immunity via cross-presentation rather the exception than the rule. The thresholds for the development of clinically manifest autoimmune disease can, however, be lowered if an inflammatory response in the target organ is maintained. As mentioned above, self-antigen-induced autoimmunity, even if the self antigen is presented by DCs, is usually self-limiting [23,25•,33•]. Inflammatory processes associated with viral infections, such as massive cytokine/chemokine release and immune cell infiltration, may reactivate subclinical autoimmunity and lead to clinical disease. Indeed, expression of inflammatory cytokines in a localized fashion in pancreatic islet cells favored the induction of IDDM by otherwise suboptimal stimuli [46,47]. Interestingly, repeated priming of RIP−GP mice with DCs led to the formation of lymphoid structures in pancreatic islets [23]. Such structures are also seen in autoimmune diseases associated with pronounced autoantibody responses such as Hashimoto’s thyroiditis, Sjögren’s syndrome and rheumatoid arthritis, and usually contain B cell follicles with follicular DCs. However, chronic inflammation of a target organ does not necessarily lead to autoimmune disease, as shown by the pancreatic expression of cytokines [47,48] or chemokines [49] which may even favor the generation of organized lymphoid structures [50,51•,52•]. It is important to note that certain cytokines may also inhibit autoimmune reactions, for example via modulation of the antigen presentation function of DCs [53••]. Thus, it appears that both the timing and dose of self-antigen expression by DCs and the development of lymphoid structures in the target organs are of major importance for the development of clinical autoimmune disease. Conclusions The high thresholds for induction of CTL-mediated autoimmune disease via exogenous loading of self-antigens on MHC class I have been demonstrated in the RIP−GP model. Priming of RIP−GP mice with H8-DC constitutively expressing the self-peptide GP33 elicited clinical manifestation of autoimmune disease, whereas the turnover of exogenously loaded GP33 on DCs led to detectable autoimmune responses, but Multiple factors contribute to the pathogenesis of autoimmune diseases. Presentation of self antigens by DCs is likely to play an important role in the initiation of autoimmunity and the progression to overt clinical autoimmune disease. Self antigens become accessible for DCs when the release of tissue antigens is induced, for example by cytopathic virus infections or by physical trauma. We have Dendritic cells in autoimmune diseases Ludewig et al. presented evidence that the amount of self peptide loaded on MHC molecules of DCs and the duration of their presentation in secondary lymphoid organs are the main factors determining the magnitude of the autoimmune response. A number of fail-safe mechanisms, however, avoid exaggerated autoimmune responses that lead to autoimmune disease; these mechanisms include the generally very low precursor frequency of self-reactive lymphocytes and the rather low efficacy of exogenous loading of MHC class I molecules with self-antigens for the activation of CTLs. The simplified threshold model presented here may help us to understand the relative importance of the multiple factors involved in the conversion of relatively frequent autoimmune responses to the rather rare manifestations of autoimmune diseases. Update A recent study by Kalled et al. [54] revealed the importance of an altered DC turnover for the susceptibility to autoimmune nephritis in the (SWR × NZB)F1 mouse model of systemic lupus erythematosus. (SWR × NZB)F1 mice are genetically highly susceptible to autoantibody-mediated lupus-like nephritis. Increased lymphocyte apoptosis and particularly high apoptosis rates of DCs, leading to an increased DC turnover, may accelerate this B-cell-driven autoimmune disease. It will be important for future studies on this and other autoimmune diseases to delineate how altered DC homeostasis influences the level and/or specificity of self-antigen presentation by DCs and other APCs. Acknowledgements We thank Betsy Metters for helpful discussions and critical reading of the manuscript. This work was supported by the Swiss National Science Foundation and the Kanton Zürich. References and recommended reading Papers of particular interest, published within the annual period of review, have been highlighted as: • of special interest •• of outstanding interest 1. Regner M, Lambert PH: Autoimmunity through infection or immunization? Nat Immunol 2001, 2:185-188. 2. Kurtzke JF: Multiple sclerosis in time and space — geographic clues to cause. J Neurovirol 2000, 6:S134-S140. 3. Miller SD, Vanderlugt CL, Begolka WS, Pao W, Yauch RL, Neville KL, Katz-Levy Y, Carrizosa A, Kim BS: Persistent infection with Theiler’s virus leads to CNS autoimmunity via epitope spreading. Nat Med 1997, 3:1133-1136. 4. Andersen O, Lygner PE, Bergstrom T, Andersson M, Vahlne A: Viral infections trigger multiple sclerosis relapses: a prospective seroepidemiological study. J Neurol 1993, 240:417-422. 5. Horwitz MS, Bradley LM, Harbertson J, Krahl T, Lee J, Sarvetnick N: Diabetes induced by coxsackie virus: initiation by bystander damage and not molecular mimicry. Nat Med 1998, 4:781-785. 6. Gangappa S, Babu JS, Thomas J, Daheshia M, Rouse BT: Virusinduced immunoinflammatory lesions in the absence of viral antigen recognition. J Immunol 1998, 161:4289-4300. 7. Oldstone MB: Molecular mimicry and autoimmune disease. Cell 1987, 50:819-820. 8. Hiemstra HS, Schloot NC, van Veelen PA, Willemen SJ, Franken KL, van Rood JJ, de Vries RR, Chaudhuri A, Behan PO, Drijfhout JW, Roep BO: Cytomegalovirus in autoimmunity: T cell crossreactivity to viral antigen and autoantigen glutamic acid decarboxylase. Proc Natl Acad Sci USA 2001, 98:3988-3991. 9. 661 Wucherpfennig KW, Strominger JL: Molecular mimicry in T cellmediated autoimmunity: viral peptides activate human T cell clones specific for myelin basic protein. Cell 1995, 80:695-705. 10. Oomes PG, Jacobs BC, Hazenberg MP, Banffer JR, van der Meche FG: Anti-GM1 IgG antibodies and Campylobacter bacteria in Guillain-Barre syndrome: evidence of molecular mimicry. Ann Neurol 1995, 38:170-175. 11. Moll H, Fuchs H, Blank C, Rollinghoff M: Langerhans cells transport Leishmania major from the infected skin to the draining lymph node for presentation to antigen-specific T cells. Eur J Immunol 1993, 23:1595-1601. 12. Roncarolo MG, Levings MK, Traversari C: Differentiation of T regulatory cells by immature dendritic cells. J Exp Med 2001, 193:F5-F9. 13. Karrer U, Althage A, Odermatt B, Roberts CW, Korsmeyer SJ, Miyawaki S, Hengartner H, Zinkernagel RM: On the key role of secondary lymphoid organs in antiviral immune responses studied in alymphoplastic (aly/aly) and spleenless (Hox11(-/-)) mutant mice. J Exp Med 1997, 185:2157-2170. 14. Moskophidis D, Lechner F, Pircher H, Zinkernagel RM: Virus persistence in acutely infected immunocompetent mice by exhaustion of antiviral cytotoxic effector T cells. Nature 1993, 362:758-761. 15. Aichele P, Brduscha-Riem K, Zinkernagel RM, Hengartner H, Pircher H: T cell priming versus T cell tolerance induced by synthetic peptides. J Exp Med 1995, 182:261-266. 16. Barker RN, Hall AM, Standen GR, Jones J, Elson CJ: Identification of T-cell epitopes on the Rhesus polypeptides in autoimmune hemolytic anemia. Blood 1997, 90:2701-2715. 17. Kuwana M, Kaburaki J, Ikeda Y: Autoreactive T cells to platelet GPIIb-IIIa in immune thrombocytopenic purpura. Role in production of anti-platelet autoantibody. J Clin Invest 1998, 102:1393-1402. 18. Thomas R, Davis LS, Lipsky PE: Rheumatoid synovium is enriched in mature antigen-presenting dendritic cells. J Immunol 1994, 152:2613-2623. 19. Nestle FO, Turka LA, Nickoloff BJ: Characterization of dermal dendritic cells in psoriasis. Autostimulation of T lymphocytes and induction of Th1 type cytokines. J Clin Invest 1994, 94:202-209. 20. Jansen A, Homo-Delarche F, Hooijkaas H, Leenen PJ, Dardenne M, Drexhage HA: Immunohistochemical characterization of monocytes-macrophages and dendritic cells involved in the initiation of the insulitis and beta-cell destruction in NOD mice. Diabetes 1994, 43:667-675. α in 21. Green EA, Eynon EE, Flavell RA: Local expression of TNFα neonatal NOD mice promotes diabetes by enhancing presentation of islet antigens. Immunity 1998, 9:733-743. 22. Knight SC, Farrant J, Chan J, Bryant A, Bedford PA, Bateman C: Induction of autoimmunity with dendritic cells: studies on thyroiditis in mice. Clin Immunol Immunopathol 1988, 48:277-289. 23. Ludewig B, Odermatt B, Landmann S, Hengartner H, Zinkernagel RM: Dendritic cells induce autoimmune diabetes and maintain disease via de novo formation of local lymphoid tissue. J Exp Med 1998, 188:1493-1501. 24. Dittel BN, Visintin I, Merchant RM, Janeway CA Jr: Presentation of the self antigen myelin basic protein by dendritic cells leads to experimental autoimmune encephalomyelitis. J Immunol 1999, 163:32-39. 25. Ludewig B, McCoy K, Pericin M, Ochsenbein AF, Dumrese T, • Odermatt B, Toes RE, Melief CJ, Hengartner H, Zinkernagel RM: Rapid peptide turnover and inefficient presentation of exogenous antigen critically limit the activation of self-reactive CTL by dendritic cells. J Immunol 2001, 166:3678-3687. This study shows that high thresholds limit the induction of self-reactive CTLs by DCs after acquisition of exogenous peptides or cell-associated antigens. 26. Ohashi PS, Oehen S, Buerki K, Pircher H, Ohashi CT, Odermatt B, Malissen B, Zinkernagel RM, Hengartner H: Ablation of ‘tolerance’ and induction of diabetes by virus infection in viral antigen transgenic mice. Cell 1991, 65:305-317. 27. Moessler H, Mericskay M, Li Z, Nagl S, Paulin D, Small JV: The SM 22 promotor directs tissue-specific expression in arterial but not in venous or visceral smooth muscle cells in transgenic mice. Development 1996, 122:2415-2425. 662 Autoimmunity 28. Ludewig B, Ochsenbein AF, Odermatt B, Paulin D, Hengartner H, Zinkernagel RM: Immunotherapy with dendritic cells directed against tumor antigens shared with normal host cells results in severe autoimmune disease. J Exp Med 2000, 191:795-804. 29. Ingulli E, Mondino A, Khoruts A, Jenkins MK: In vivo detection of dendritic cell antigen presentation to CD4(+) T cells. J Exp Med 1997, 185:2133-2141. 30. Hermans IF, Ritchie DS, Yang J, Roberts JM, Ronchese F: CD8+ T cell-dependent elimination of dendritic cells in vivo limits the induction of antitumor immunity. J Immunol 2000, 164:3095-3101. 31. Ludewig B, Bonilla WV, Dumrese T, Odermatt B, Zinkernagel RM, Hengartner H: Perforin-independent regulation of dendritic cell homeostasis by CD8(+) T cells in vivo: implications for adaptive immunotherapy. Eur J Immunol 2001, 31:1772-1779. 32. Jackson CE, Puck JM: Autoimmune lymphoproliferative syndrome, a disorder of apoptosis. Curr Opin Pediatr 1999, 11:521-527. 33. Ludewig B, Freigang S, Jaggi M, Kurrer MO, Pei YC, Vlk L, • Odermatt B, Zinkernagel RM, Hengartner H: Linking immunemediated arterial inflammation and cholesterol-induced atherosclerosis in a transgenic mouse model. Proc Natl Acad Sci USA 2000, 97:12752-12757. Using a new transgenic mouse model of DC-induced cardiovascular immunopathology, the authors show that the regenerational capacity of different organs — heart tissue versus the vascular wall of arteries — determines the outcome of a chronic CTL-mediated autoimmune reaction. 34. Inaba K, Turley S, Yamaide F, Iyoda T, Mahnke K, Inaba M, Pack M, Subklewe M, Sauter B, Sheff D et al.: Efficient presentation of phagocytosed cellular fragments on the major histocompatibility complex class II products of dendritic cells. J Exp Med 1998, 188:2163-2173. 35. Larsson M, Fonteneau JF, Bhardwaj N: Dendritic cells resurrect antigens from dead cells. Trends Immunol 2001, 22:141-148. 36. Shen Z, Reznikoff G, Dranoff G, Rock KL: Cloned dendritic cells can present exogenous antigens on both MHC class I and class II molecules. J Immunol 1997, 158:2723-2730. 37. Albert ML, Sauter B, Bhardwaj N: Dendritic cells acquire antigen from apoptotic cells and induce class I-restricted CTLs. Nature 1998, 392:86-89. 38. Regnault A, Lankar D, Lacabanne V, Rodriguez A, Thery C, Rescigno M, Saito T, Verbeek S, Bonnerot C, Ricciardi-Castagnoli P, Amigorena S: Fcγγ receptor-mediated induction of dendritic cell maturation and major histocompatibility complex class I-restricted antigen presentation after immune complex internalization. J Exp Med 1999, 189:371-380. 39. Kurts C, Heath WR, Carbone FR, Allison J, Miller JF, Kosaka H: Constitutive class I-restricted exogenous presentation of self antigens in vivo. J Exp Med 1996, 184:923-930. 40. Morgan DJ, Kreuwel HT, Sherman LA: Antigen concentration and precursor frequency determine the rate of CD8+ T cell tolerance to peripherally expressed antigens. J Immunol 1999, 163:723-727. 41. Kurts C, Cannarile M, Klebba I, Brocker T: Dendritic cells are • sufficient to cross-present self-antigens to CD8 T cells in vivo. J Immunol 2001, 166:1439-1442. This study shows that DCs can cross-present exogenous self-antigens and induce antigen-specific cell division of CD8+ T cells. However, the RIP–mOVA mouse is an engineered transgenic model where central tolerance mechanisms have to be bypassed by adoptive transfer of OVA-reactive CTLs. 42. Kurts C, Carbone FR, Barnden M, Blanas E, Allison J, Heath WR, Miller JF: CD4+ T cell help impairs CD8+ T cell deletion induced by cross-presentation of self-antigens and favors autoimmunity. J Exp Med 1997, 186:2057-2062. 43. Kurts C, Miller JF, Subramaniam RM, Carbone FR, Heath WR: Major histocompatibility complex class I-restricted cross-presentation is biased towards high dose antigens and those released during cellular destruction. J Exp Med 1998, 188:409-414. 44. den Haan JM, Lehar SM, Bevan MJ: CD8(+) but not CD8(-) dendritic • cells cross-prime cytotoxic T cells in vivo. J Exp Med 2000, 192:1685-1696. This study shows that splenic DCs can cross-present antigen to CTLs after in vivo priming with large amounts of OVA-loaded β2-microglobulin-deficient splenocytes. Only CD8α+, but not CD8α–, DCs demonstrated the ability to cross-present in vivo. Importantly, only a very small percentage (0.6%–1.0%) of this subpopulation was found to possess cross-presentation capability in vivo. 45. Ochsenbein AF, Sierro S, Odermatt B, Pericin M, Karrer U, Hermans I, •• Hemmi S, Hengartner H, Zinkernagel RM: Roles of tumourlocalisation, second signals and cross-priming in cytotoxic T-cell induction. Nature 2001, 411:1058-1065. This study establishes that the induction of tumor-specific CTLs depends on sufficient tumor cells reaching secondary lymphatic organs and that tumors that stay outside secondary lymphatic organs are immunologically ignored by T cells. In addition, cross-presentation of tumor antigens to CTLs mediated by MHC class I molecules of APCs was found to be inefficient and not protective. 46. Ohashi PS, Oehen S, Aichele P, Pircher H, Odermatt B, Herrera P, Higuchi Y, Buerki K, Hengartner H, Zinkernagel RM: Induction of diabetes is influenced by the infectious virus and local expression α. J Immunol 1993, of MHC class I and tumor necrosis factor-α 150:5185-5194. 47. von Herrath MG, Allison J, Miller JF, Oldstone MB: Focal expression of interleukin-2 does not break unresponsiveness to ‘self’ (viral) antigen expressed in beta cells but enhances development of autoimmune disease (diabetes) after initiation of an anti-self immune response. J Clin Invest 1995, 95:477-485. 48. Picarella DE, Kratz A, Li CB, Ruddle NH, Flavell RA: Insulitis in transgenic mice expressing tumor necrosis factor beta (lymphotoxin) in the pancreas. Proc Natl Acad Sci USA 1992, 89:10036-10040. 49. Grewal IS, Rutledge BJ, Fiorillo JA, Gu L, Gladue RP, Flavell RA, Rollins BJ: Transgenic monocyte chemoattractant protein-1 (MCP-1) in pancreatic islets produces monocyte-rich insulitis without diabetes: abrogation by a second transgene expressing systemic MCP-1. J Immunol 1997, 159:401-408. 50. Kratz A, Campos Neto A, Hanson MS, Ruddle NH: Chronic inflammation caused by lymphotoxin is lymphoid neogenesis. J Exp Med 1996, 183:1461-1472. 51. Fan L, Reilly CR, Luo Y, Dorf ME, Lo D: Ectopic expression of the • chemokine TCA4/SLC is sufficient to trigger lymphoid neogenesis. J Immunol 2000, 164:3955-3959. Previous studies (e.g. [48–50]) had shown that the ectopic expression of inflammatory cytokines may induce the formation of organized lymphoid structures in peripheral non-lymphoid organs. This study, along with [52•], established that the ectopic expression of a chemokine normally regulating constitutive lymphocyte homing to lymph nodes and spleen is sufficient to induce lymphoid neogenesis in the pancreas. 52. Luther SA, Lopez T, Bai W, Hanahan D, Cyster JG: BLC expression • in pancreatic islets causes B cell recruitment and lymphotoxindependent lymphoid neogenesis. Immunity 2000, 12:471-481. See annotation to [51•]. 53. King C, Mueller HR, Malo CM, Murali-Krishna K, Ahmed R, King E, •• Sarvetnick N: Interleukin-4 acts at the locus of the antigenpresenting dendritic cell to counter-regulate cytotoxic CD8+ T-cell responses. Nat Med 2001, 7:206-214. This study shows that IL-4 may influence the activity of DCs by blocking the differentiation of CTL precursors. The underlying molecular mechanism is the alteration of the expression ratio of the costimulatory ligands B7.1/B7.2 on DCs. Whereas B7.2 induces expansion of CD8+ T cells, B7.1 regulates the acquisition of cytolytic activity. IL-4 influences DC function by eliciting qualitative differences in T cell responses and changes, thereby affecting the abililty of DCs to stimulate autoimmune responses. 54. Kalled SL, Cutler AH, Burkly LC: Apoptosis and altered dendritic cell homeostasis in lupus nephritis are limited by anti-CD154 treatment. J Immunol 2001, 167:1740-1747. Dendritic cells in autoimmune diseases Ludewig et al. 663