Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Gene therapy wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Gene desert wikipedia , lookup
Genome evolution wikipedia , lookup
Gene nomenclature wikipedia , lookup
Behavioural genetics wikipedia , lookup
History of genetic engineering wikipedia , lookup
Quantitative trait locus wikipedia , lookup
Epigenetics of human development wikipedia , lookup
Medical genetics wikipedia , lookup
Gene expression programming wikipedia , lookup
Human genetic variation wikipedia , lookup
Genomic imprinting wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Population genetics wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Hardy–Weinberg principle wikipedia , lookup
Gene expression profiling wikipedia , lookup
Public health genomics wikipedia , lookup
Genome (book) wikipedia , lookup
Polymorphism (biology) wikipedia , lookup
Designer baby wikipedia , lookup
Genetic drift wikipedia , lookup
Pharmacogenomics wikipedia , lookup
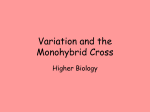
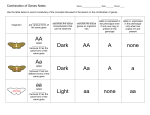
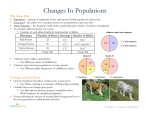
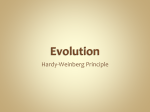
Molecular Psychiatry (1998) 3, 50–60 1998 Stockton Press All rights reserved 1359–4184/98 $12.00 ORIGINAL RESEARCH ARTICLE Correlation of length of VNTR alleles at the X-linked MAOA gene and phenotypic effect in Tourette syndrome and drug abuse R Gade1, D Muhleman1, H Blake1, J MacMurray2, P Johnson3, R Verde3, G Saucier4 and DE Comings1 1 Department of Medical Genetics, City of Hope Medical Center, Duarte, CA; 2Department of Psychiatry, Loma Linda University, Loma Linda, CA; 3Jerry L Pettis VA Hospital, Loma Linda, CA; 4Department of Psychology, California State University, San Bernardino, CA, USA Abnormalities in monoamine oxidase (MAO) levels have been implicated in a wide range of psychiatric disorders. We have examined a VNTR polymorphism at the X-linked MAOA gene to test two hypotheses: (1) Do variants of the MAOA gene play a role in any of the behavioral disorders associated with Tourette syndrome or drug abuse? (2) If so, is there any correlation between the length of the alleles and the phenotypic effect? We examined two independent groups: 375 TS patients, relatives and controls, and 280 substance abusers and controls. The alleles were divided into four groups of increasing size. There was a significant association between the MAOA gene and behavioral phenotypes in both groups, and in both the longest alleles were associated with the greatest phenotypic effect. The strongest effect was for the diagnosis of drug dependence (P = 0.00003). The VNTR allele groups were in significant linkage disequilibrium with the Fnu4H1 polymorphism previously shown to be associated with MAO-A activity. While these results are consistent with the possibility that different-sized alleles of the short-repeat polymorphisms themselves may play a role in gene regulation, further studies directly linking these alleles with enzyme levels need to be done. Keywords: minisatellites; polygenic inheritance; attention deficit hyperactivity disorder; alcoholism Introduction Monoamine oxidase is one of the major enzymes responsible for the degradation of neurotransmitters in the synapses of the brain. Significant improvement in mood and other behaviors can occur by the administration of medications that inhibit MAO activity. The MAOA and MAOB genes are X-linked at Xp11.4–11.31–3 and produce two different forms of the enzyme, both under strong genetic control. Both genes contain 15 exons, span at least 60 kb, and exhibit identical exon– intron organization.4 MAO A has a higher affinity for endogenous neurotransmitters, is present in catecholaminergic neurons and is irreversibly inactivated by clorgyline. MAO B has a higher affinity for dietary amines, is present in astrocytes and serotonergic neurons, and is irreversibly inhibited by pargyline and deprenyl.5 Prior to the availability of genetic markers, studies of the potential role of MAO in behavior involved examination of platelet MAO enzyme levels. Many such studies have suggested a correlation between low Correspondence: Dr R Gade, Department of Medical Genetics, City of Hope Medical Center, Duarte, CA, USA Received 17 January 1997; revised 7 April and 22 July 1997; accepted 22 July 1997 MAO levels and alcoholism;6–9 schizophrenia;10 depression;11,12 manic depressive disorder;13 suicide;7,11,14–16 attention deficit hyperactivity disorder (ADHD);17 and risk-taking, sensation seeking or externalizing personality traits.9,14,18–20 Other studies have failed to find associations with one or more of these traits.21–23 Because of the potential effect of age,8 alcohol, antidepressants, drugs, gender, laboratory technique, diet, and other variables, on platelet enzyme levels,24 the use of genetic polymorphisms at the MAO genes may give more reproducible results than enzyme levels. The cloning and sequencing of the MAOA and -B genes and identification of associated polymorphisms now allow such genetic studies. Hotamisligil and Breakefield25 examined the Fnu4H1 polymorphism, associated with a T→C variant at position 1460, and the EcoRV polymorphism, associated with a T→G variant at position 941, of the MAO-A cDNA. Since both involved substitutions in the third base of a codon, they were not associated with amino acid substitutions. They examined 40 cell lines of known MAO-A activity. All lines that carried the Fnu4H1 C variant also carried the EcoRV G variant. When the sample was divided into two groups on the basis of lower vs higher MAO-A activity, the less common Fnu4H1 C or + allele (our 2 allele), present in 25% of the cell lines, was significantly (P = 0.028) MAO genes R Gade et al associated with the higher activity group. Lin et al26 reported a significant increase in the more common MAOA Fnu4HI T or 1 allele,26 associated with lower MAO levels25 in manic depression, while Craddock et ¨ al27 and Nothen et al,28 were unable to confirm this. Brunner et al29,30 reported a Dutch family where many males had problems with impulsive, aggressive and hypersexual behaviors due to a hemizygous chain termination mutation in the MAOA gene. This was consistent with the numerous other studies suggesting a correlation between low MAO levels and impulsive, risk-taking, externalizing behaviors. Because of these prior findings with the MAOA gene we have focused on this gene in the present studies. Vanyukov et al31 examined the MAOA gene in 23 male and 34 female alcoholics compared to 31 male and 78 female controls, using a CA repeat polymorphism.32 There was a trend in males (P = 0.17) but not in females (P = 0.8) for an association between higher molecular weight alleles (.115 bp) in young substance abusers, and a marginal association of the .115 bp alleles with age of onset (P = 0.03). Tourette syndrome (TS) and ADHD are related, hereditary impulse disorders that are also associated with a wide range of externalizing, risk-taking, aggressive33 and hypersexual behaviors,34 substance abuse,35,36 and other behaviors.37,38 To determine if genetic variants at the MAOA gene were associated with TS or ADHD, we have examined the MAOA VNTR polymorphism39 in a series of controls, TS probands and their relatives, using the techniques reported previously for our studies of the DRD2, DbH and DAT1 genes in TS.40 Since a simple comparison of the frequency of the different alleles in controls vs TS probands might miss the possibility that the MAO genes were only associated with a few specific behaviors not present in all cases, we tested for the possible role of these genes in 27 different behavioral variables. Based on our prior published41–43 and unpublished44–46 studies using short repeat polymorphisms, we have become interested in the hypothesis that the length of the alleles per se might be related to phenotypic effect. The rationale for this, reviewed in the companion manuscript,47 is that the sequence of most simple repeats result in the formation of Z-DNA with the amount being dependent upon the length of the repeat.48 The Z-DNA conformation opens the DNA helix and exposes the individual bases, making it uniquely capable of interacting with nuclear proteins.49 For these and other reasons Z-DNA has been implicated in gene regulation.50,51 We anticipated that if the mini- and microsatellite polymorphisms do play a role in the variations in gene function involved in polygenic inheritance, their effect must be subtle, since if the effects were major, they would result in single gene rather than polygenic disorders. X-linked genes form a unique vehicle to examine this hypothesis and search for subtle effects since, at least in males, each allele is hemizygously present thus eliminating the confounding factor of heterozygosity, which can be extensive when multiple alleles of differ- ent size are present. To test the hypothesis that repeat length might be related to phenotypic effect we divided the VNTR alleles into four groups of increasing length. This allowed us to determine if the shorter or longer alleles were preferentially associated with a greater phenotypic effect. Methods Group I: the TS group The subjects included 57 controls, 229 TS probands most of whom were severely affected with multiple associated behavioral disorders,52 and 90 affected and unaffected relatives of TS probands. All subjects were non-Hispanic Caucasians and over 90% were of Western European origin. The controls for the TS group consisted of adopting and step parents of TS probands, subjects with non-psychiatric disorders from other clinics at the City of Hope, and professional and nonprofessional hospital staff from the City of Hope Medical Center. Both the TS subjects and the controls have been described in detail elsewhere.37,40,53 Behavioral scores Each TS control and TS proband or relative was required to fill out a questionnaire based on the Diagnostic Interview Schedule54 or DSM-III-R55 criteria. This provided a structured review of a wide range of psychiatric symptoms. These symptoms were grouped into 27 different behaviors including ADHD, substance abuse, mood, anxiety, school performance, stuttering, tics and others. The questions used for these behavioral scores have been described in detail elsewhere.33–35,37,40,54,56 Two behavioral scores were used to assess ADHD. The first, called ADHD, was based on the presence of at least half of a series of 22 ADHD variables from DSM-III and DSM-III-R criteria. The second, ADHD-R was based on the DSM-III-R diagnostic criteria. Three QTVs not used previously were inattention, impulsivity and hyperactivity. These were the three subscores that cumulatively produced the ADHD score. QTV abbreviations include CD for conduct disorder, ODD for oppositional defiant disorder,33 and MDE for major depressive episode56 symptoms. The rationale for examining comorbid behaviors is the prior observation that certain genes may be more strongly associated with specific comorbid behaviors present in TS than with the diagnosis per se.40 This questionnaire is not meant to provide DSM-III-R or DSM-IV diagnoses but rather to provide a highly structured method of producing QTVs for different areas of behavior. The advantage of continuous traits is that they provide a greater range of severity than dichotomous diagnoses. The accuracy, utility and sensitivity of a questionnaire-based approach to symptom evaluation has been demonstrated by others57,58 by comparing the use of such an instrument to an interviewer administration of the same structured instrument. Our review of the questionnaires with many hundreds of subjects has indicated that they accurately reflect the information obtained by personal interview. 51 MAO genes R Gade et al 52 Group II: the substance abuse group The patients consisted of 120 non-Hispanic Caucasian males from an inpatient Addiction Treatment Unit (ATU) of the Jerry L Pettis Veterans Administration Hospital in Loma Linda, California. Since October 1994, all new admissions to the ATU who give informed consent, were entered into a National Institute of Drug Abuse sponsored study of genetic factors in drug abuse/dependence. Assessments All ATU subjects were assessed with the Michigan Alcoholism Severity Test,59 a 24-item selfadministered questionnaire revised to include drug abuse (MAST-R), the clinician-administered Diagnostic Interview Schedule (DSM-III-R version),54 to diagnose the presence of substance dependence disorders, and the clinician-administered Addiction Severity Index Fifth Edition (ASI),60 to evaluate a range of alcohol and drug use variables. ASI We utilised the Drug/Alcohol use and the legal status sections of the ASI. The areas covered were the following: a) b) c) d) e) f) g) Specific substances used. To assess the use of specific substances, questions were asked about the lifetime use (in years) of alcohol use to intoxication, heroin, other opiates/analgesics, barbiturates, other sedatives/hypnotics/tranquillizers, cocaine, amphetamines, cannabis, hallucinogens, and inhalants. Route of administration. For each of the above, where relevant, the subjects were asked about the route of administration. The options were oral, nasal, smoking, and IV injection. The continuous variable #IV drugs used was calculated by adding up the total number of different drugs injected IV. The variable IV drug use was a dichotomous variable of 0 for no IV drug use and #1 for use of one or more drugs IV. Problems. ‘How many times have you had alcohol DTs? Overdosed on drugs?’ ‘How many days in the past 30 days have you experienced alcohol problems? Drug problems?’ Money spent. ‘How much would you say you spent during the past 30 days on alcohol? On drugs?’ Severity. An interviewer-based severity assessment for the need for treatment ranged from 0 (no treatment necessary) to 9 (treatment needed to intervene in a life-threatening situation). Alcohol abuse? Drug abuse? Legal status. Questions were also asked about various legal aspects of drug and alcohol abuse. ‘How many times in your lifetime were you charged with driving while intoxicated?’ ‘How many times in your lifetime were you arrested and charged with drug charges? How many of these charges resulted in convictions?’ Summary scores. When the responses could range from 0 to any number, they were scored as a ‘0’ for a 0 and a ‘1’ for any other number. Those questions relevant to alcohol use were summed for a total alcohol score and those relevant to drug use were summed for the drug score. Substance abuse control group The controls for the substance abuse group were independent of the controls for the TS patients. They consisted of two sets. The first were 45 older male, non-Hispanic Caucasian students from the California State University at San Bernardino (mean age of 30.1 years). Those with significant problems with substance abuse were excluded on the basis of the MAST-R test. The second set consisted of the male parents of twins from the Minnesota Twin Family study. Since these are ascertained from the entire state simply on the basis of having had twins 11 or 17 years of age, they represent a more random set of all socioeconomic and educational groups than the college students. Although all the controls were scored as negative on the substance abuse variables, since the results of substance abuse assessments were not yet available on the twin controls, some may have been positive. However, since this is a random crosssection of a predominately rural state we assume the number of false negatives in this group is small. Polymorphisms The MAOA VNTR polymorphism The rationale for choosing the VNTR polymorphism at the MAOA gene is as follows. A short tandem repeat polymorphism was chosen to specifically examine the hypothesis that the length of the repeat might be associated with a phenotypic effect. An X-linked gene was chosen since, at least when males are studied, the complication of how to interpret heterozygotes is avoided. An MAO gene was chosen because it is X-linked. The MAOA gene was chosen because two different repeat polymorphisms have been reported to be associated with it. We chose the VNTR polymorphism39 because it gave a wider spread in allele size (40+ bp) than the (CA)n repeat (16 bp). This complex polymorphism consists of a GT microsatellite directly adjacent to an imperfectly duplicate novel 23-bp VNTR motif, with alleles differing in both the number of dinucleotide repeats and VNTR repeats. The VNTR polymorphism was present in a 2.9kb SalI-EcoRI fragment from phage 6.12 which contained the first exon of the MAOA gene.39 DNA was extracted from whole blood by standard procedures. Target DNA was amplified by PCR.61 To label the PCR products, 0.1 mM of each primer labeled with fluorescent HEX or FAM Amidite (Applied Biosystems, Foster City, CA, USA) primers were used in the reactions (Table 1). Two microliters of the 10-fold diluted PCR product were added to 2.5 ml deionized formamide and 0.5 ml of ROX 500 standard (Applied Biosystems) and denatured for 2 min at 92°C and loaded on 6% polyacrylamide gel in an Applied Biosystems 373 DNA sequencer. The gel was electrophoresed for 5 h at 1100 V and constant 30 W. The gel was laser scanned MAO genes R Gade et al Table 1 MAOA VNTR polymorphism: comparison of the different behavior scores by ANOVA for the different allele groups. (Mean and standard deviation) (n = 287) Behavior Allele groups by size in bp ,320 (n = 82) Mania OCD Sexual Sleep Grade school Gambling Stuttering Learn Inattention ADHD ADDR Impulsivity Shopping MDE CD Hyperactivity Phobia Schizoid Gen. anxiety Somatization Drugs Read ODD Tics Alcohol Panic Smoking 1.43* 2.18 0.62* 0.36 2.60 0.13* 0.13 0.52* 6.69 19.43 4.63 5.74 0.58 3.00 2.78 6.91 2.00 1.31 0.21 2.13 0.36 1.86 3.07 2.81 0.51 2.91 0.07 1.8 2.8 1.1 0.7 1.7 0.9 0.3 0.9 5.2 14.9 4.9 4.9 1.3 2.8 2.4 5.6 2.7 2.3 0.4 3.0 1.2 1.9 3.3 3.7 2.3 2.0 0.3 320–333 (n = 43) 1.36* 2.18 0.47* 0.38 2.90 0.27 0.11 0.65 7.37 20.95 4.84 6.30 1.00 3.29 2.90 7.27 2.15 0.68* 0.18 1.58 0.45 1.36 3.02 3.04 0.81 3.09 0.11 1.9 2.4 0.9 0.8 2.0 0.8 0.3 1.0 4.9 13.5 4.6 4.8 2.2 3.1 2.1 5.2 3.0 1.3 0.3 2.4 1.6 1.8 2.7 3.4 2.9 2.1 0.3 334 (n = 110) 1.59* 2.80 0.66* 0.49 2.98 0.22 0.25 0.54* 7.67 21.18 5.18 6.49 1.32 3.45 2.97 7.00 2.45 1.34 0.28 2.17 0.40 1.78 3.16 2.84 0.31 3.18 0.05 2.27 2.8 1.2 0.9 2.1 0.8 0.4 0.9 4.7 13.9 4.7 4.7 2.8 3.1 2.2 5.4 2.7 2.2 0.4 3.0 1.3 2.1 3.1 3.5 1.8 2.2 0.2 F-ratio P F2 3.59 2.16 3.91 2.31 1.89 2.49 2.23 3.32 1.42 1.53 1.57 1.35 1.61 1.01 1.15 1.59 0.71 2.26 0.85 1.16 0.81 1.75 0.57 0.55 1.41 0.27 0.53 0.014 0.093 0.009 0.075 0.131 0.060 0.084 0.020 0.235 0.206 0.196 0.257 0.186 0.385 0.328 0.190 0.548 0.081 0.463 0.325 0.489 0.156 0.633 0.642 0.241 0.845 0.662 6.39a 5.89a 5.82a 5.56a 5.14a 4.82a 4.41a 4.37a 4.15a 3.74a 3.74a 3.68a 3.23 2.90 2.54 2.29 2.10 1.92 1.60 1.34 1.28 1.27 1.02 0.73 0.45 0.20 0.10 $335 (n = 52) 2.59 3.31 1.25 0.76 3.46 0.61 0.23 1.00 8.48 24.80 6.42 7.46 1.09 3.92 3.54 8.86 2.65 1.84 0.29 2.90 0.75 2.34 3.73 3.57 1.11 2.98 0.77 2.8 3.2 1.6 1.1 2.1 1.6 0.4 1.1 5.3 15.3 5.2 5.0 2.4 3.1 2.6 5.9 3.3 2.3 0.4 3.7 2.0 2.5 3.4 4.1 3.2 2.2 0.3 a Significant at ,0.05, F2 = F-ratio for linear ANOVA. *Significantly less than .335 at a = 0.05 by Tukey. and analyzed using the internal ROX 500 standards. The peaks were recognized by Genotyper (version 1.1) (Applied Biosystems) based on the color fragments sized by base pair length. Complete information for each sample was printed from every gel file and the compiled data were submitted for analysis. Allele groups To examine the hypothesis that the length of the MAOA alleles might correlate with a phenotypic effect, the alleles were divided into four groups (see Results). These were labeled 1 to 4, shortest to longest to form the MAOA genotype variable. Females were utilized only in the TS group. Only those that were homozygous for a given allele group were included in the analysis. We used two rules for bining: a) there must be enough groups to examine a range of lengths; and b) to maximize statistical power the number of subjects should be similar in each group. Thus, if there was a single peak of allele frequencies the division would have been into the shortest 1/3, the middle 1/3 and the longest 1/3. However, the distribution of allele sizes for the MAOA VNTR was into two peaks. For males only, the smaller peak contained 32% of the alleles and ranged in size from 299 to 314 bp in length. The larger peak contained 68% of the alleles ranging in size from 323 to 338 bp in length. Since the majority of the alleles were in this peak we divided it as if there was a single peak (ie shorter, middle, and longer group of alleles). The center of this peak contained a single 334bp group consisting of 31% of the alleles that could not be subdivided. The application of these rules resulted in four bins ,320 bp, 320–333 bp, 334 bp and $335 bp consisting of 32, 23, 31 and 14% of the alleles. It was not possible to use the binning described by Hinds et al39 because three of their five groups had a very low allele frequency. In fact, we had no subjects in any of these three minor groups. Fnu4H1 polymorphism The test for this polymorphism was based on the procedure of Hotamisligil and Breakefield.25 We have termed their ‘–’ as our 1’ allele and their ‘+’ as our ‘2’ allele. In their study the + allele had the higher MAOA activity. Statistical analyses For the Tourette syndrome group, ANOVA was used to examine the relative magnitude of each QTV for the four different allele groups. 53 MAO genes R Gade et al 54 Linear ANOVA was used to test for a significant progressive increase in means across the four allele groups. The SPSS (SPSS, Inc, Chicago, IL, USA) statistical package was used. For linear ANOVA the subcommand polynomial was set to 1. MANOVA was used to determine if any of the QTVs were significant when all the variables were examined simultaneously. Multivariate linear regression analysis was used as a second approach to determine if any of the QTVs was significant when all the variables were examined simultaneously. The MAOA genotype was set as the dependent variable and the 27 QTVs were entered stepwise as the independent variables. Chi square The above studies indicated that the group with the longest alleles had the highest means for the majority of the QTVs. The potential progressive decrease in frequency of the $335 bp allele group was compared across four groups with progressively fewer TS symptoms: TS probands with ADHD, TS probands without ADHD, relatives with TS and relatives without TS. For the Substance Abuse Group, MANOVA was used to determine if there was a significant association between the four MAOA allele groups and the two summary variables, the alcohol and the drug score. ANOVA was used to examine the means of the alcohol and drug scores for the four allele groups. Linear chi square was used to examine the potential progressive increase in the frequency of the $335 bp group across three groups: controls, the substance abusers without the behavior (ATU without), and the substance abusers with the behavior (ATU with). The ATU without group was included to rule out the possibility that this allele group might be increased in frequency in the substance abusers because of comorbidity for a different behavior. To help exclude this, the frequency of the allele group had to be at least 20% higher in the substance abusers with the behavior than without the behavior. Since the hypothesis was that the frequency of these alleles would progressively increase across these three groups, the linear chi square statistic was used. Regression analysis To determine the maximum percent of the variance of drug-related variables accounted for by the MAOA gene, regression analysis was performed in which subjects carrying the ,335 bp alleles were scored as 1, and those carrying the $335 alleles scored as 2. This was performed for the drug dependence variable (controls = 1, ATU without scored 2, and ATU with scored 3) since this was the chi square variable most highly associated with the MAOA gene. Results VNTR allele groups The distribution for the alleles for both groups is shown in Figure 1. Since this was a complex VNTR the alleles did not fall into a clear-cut pattern of even or odd numbers of base pairs. The results are shown exactly as they were generated by the Genotyper program. There were no alleles between 316 bp and 323 bp, thus producing two clear major groups of ,320 and .320 bp. However, to allow an examination of the hypothesis that phenotypic effects might be related to size, the alleles of the larger 323–339 bp group were divided into three sub-groups consisting of alleles shorter than the main peak 320–333 bp, the main peak of 334 bp, and alleles longer than the main peak of $335 bp. There were 219 males and 156 females for a total of 375 subjects in the TS group. Of the females, 88 were heterozygotes. When these were removed it left 287 subjects in the study of whom 36 were controls. In this final group, there were no significant differences in the frequency distribution of the four allele groups in males vs females. The TS group The ANOVA results for each of the QTVs vs the four allele groups are shown in Table 1. The results for regular ANOVA are shown under F-ratio and P value. The F-ratio for linear ANOVA is shown under the F2 column, with a superscript of a for those that were significant at ,0.05. The QTVs are ordered by the decreasing magnitude of the F-ratio in the F2 column. Those allele groups where the means were significantly less than for the $335 bp group, as determined by the Tukey test with a set at #0.05, are shown by an asterisk. With the exception of stuttering, shopping and panic (which gave the lowest F-ratio), for the remaining 24 QTVs the means were highest for those subjects carrying the $335 alleles. This is diagramatically illustrated for the three ADHD subgroups of inattention, impulsivity and hyperactivity and 13 other QTVs with the highest Fratios, in Figure 2. MANOVA The results of MANOVA for all 27 QTVs were significant for sexual (P = 0.012), learning problems (P = 0.023), gambling (P = 0.025), and mania (P = 0.025). Multivariate regression analysis When all 27 QTVs were examined simultaneously in a stepwise multivariate regression analysis, the variable grade school problems (P = 0.012) and gambling (P = 0.038) were significant. Based on the r2 values, the MAOA gene accounted for only 3.9% of the variance of these QTVs. Chi square analysis There was a significant progressive decrease in the percent of subjects that carried the $335 alleles, progressing from TS probands with ADHD (24%, n = 129), to TS probands without ADHD (20.0%, n = 50), to relatives with TS (12.5%, n = 16) to non-TS relatives (5.6%, n = 56) (P = 0.003). Substance abuse group Controls vs ATU subjects. For the 160 combined controls, the distribution of the four allele groups was as follows: ,320 34.4%, 320–333 38.1%, 334–335 21.3%, $335 6.3%. For the 120 ATU subjects, the frequencies were as follows: ,320 39.2%, 320–333 18.3%, 334 MAO genes R Gade et al 55 Figure 1 Distribution of the alleles of the MAOA VNTR polymorphism (total number of alleles = 768). 20.8%, $335 21.7%. These were significantly different, x2 = 22.17, P = 0.00006. The frequency of the $235 bp group was comparable in the two control groups, 8.9% for the San Bernardino group and 5.2% for the parents of the twins (x2 = 0.744, P = 0.38). MANOVA for the alcohol and drug score indicated that while both showed a significant association with the MAOA gene VNTR alleles, this was more significant for the drug score (P = 0.001) than for the alcohol score (P = 0.012) (Table 2). The result for the combined MANOVA was also significant (P = 0.007). The n of 257 is smaller than the total of 160 controls + 120 ATU or 280, because only 97 ATU subjects had completed the ASI. By contrast, all 120 completed the DIS for verification of the DSM diagnosis of alcohol and/or drug dependence. ANOVA for the two scores showing the means for each allele group, are shown in Table 3, and illustrated in Figure 3. As for the TS group, the highest means were present in the $335 bp allele group. For the drug score, the three other allele groups were significantly lower than for the $335 bp group by the Tukey test. Chi square To determine if the MAO gene was preferentially associated with certain types of substance abuse, 14 of the variables relevant to the type of substance used were examined. The frequency of the $335 bp allele group in the controls vs ATU subjects without the behavior (ATU without) vs ATU subjects with the behavior (ATU with), is shown in Table 4. Since 14 types of substance use variables were examined only those with a P of less than 0.0036 (0.05/14) are considered significant with a Bonferroni correction. Only those with a P of ,0.01 are shown. The exception is alcohol dependence only. This is shown to illustrate the fact that there was little increase in frequency of the $335 bp alleles in subjects with alcohol dependence only compared to those with drug dependence, or drug and alcohol dependence. By contrast, the drug dependence only variable gave the highest value (x2 = 17.4, P = 0.00003). Regression analysis The results of regression analysis of the allele group (,335 vs $335) vs the diagnosis of drug dependence gave the following results: r = 0.25, r2 = 0.0625, T = 4.305, and P = 0.0001. Fnu4H1 polymorphism To examine the potential linkage disequilibrium between the VNTR and Fnu4H1 alleles, we genotyped 273 males that were also genotyped at the VNTR polymorphism. We restricted our analysis to males since the results were clearer than in females. There was a highly significant non-random association of the alleles at the two polymorphisms (x2 = 132.91, P ,0.000001). The results are shown in Figure 4. The ,320 VNTR allele group was associated with the less common Fnu4H1 2 allele, while the MAO genes R Gade et al 56 Table 2 MANOVA for alcohol and drug scores for the substance abuse group vs the MAOA allele groups. (n = 257 males only) Variable Alcohol score Drug score Total (Wilks) F-ratio P 3.72 5.85 2.99 0.012 0.001 0.007 Table 3 ANOVA for alcohol and drug scores of the substance abuse group vs MAOA allele groups Allele group n Mean s.d. F-ratio P Alcohol score ,320 320–333 334 $335 94 81 56 26 2.27 1.49a 1.94 3.73 3.1 3.0 2.7 3.52 3.72 0.012 Drug score ,320 320–333 334 $335 94 81 56 26 3.59a 1.94a 3.34a 6.42 5.2 3.8 4.9 6.2 5.85 0.0007 Significantly lower than the mean for #335 allele group at a = 0.05 by the Tukey test. a remaining three VNTR groups were associated with the Fnu4H1 1 allele. Based on the comparison of Figures 2 and 4 it would be anticipated that if the VNTR alleles were divided into ,320 bp and .320 bp it should give results similar to the Fnu4H1 polymorphism with the Fnu4H1 2 < ,320 and Fnu4H1 1 allele < .320. For the TS group there were 71 subjects genotyped at both polymorphisms. Since mania gave the most significant results (Table 1) this variable was used for the comparison. The mean for the 53 subjects carrying the Fnu4H1 1 allele was 2.01 (s.d. 2.17) and for the 2 allele was 1.55 (s.d.). The comparable figures for the VNTR were 1.94 (s.d. 2.12) for the .320 bp, and 1.75 (s.d. 1.98) for the ,320 bp group. (The mean for the 16 $335 subjects was 2.43 (s.d. 2.42).) Because of the relatively small numbers neither grouping was significant. Since the Hotamisligil and Breakefield study25 showed the Fnu4H1 allele (our 1 allele) was associated with lower MAOA activity, we assume the $335 VNTR allele group was associated with the lowest MAOA activity. Discussion Figure 2 Distribution of the means of 14 of the Tourette syndrome group QTVs across the four allele groups of the MAOA VNTR polymorphism. There has been a great deal of interest in the possible role of MAO A and B in psychiatric disorders. Until recently the relevant studies were limited to an examination of platelet enzyme levels. The cloning and sequencing of the MAO A and B genes, and the identification of marker polymorphisms have made it pos- MAO genes R Gade et al with a wide range of impulsive, aggressive, affective, hypersexual and other behaviors. In a previous study40 we found that identifying a role of three dopaminergic genes (DRD2, DbH and DAT1) was best determined by an examination of a relatively large number of TS subjects, their relatives and controls. We have suggested that TS and related disorders are polygenically inherited and that each gene contributes only a small percent of the variance of any behavior score.40,51,62,63 The present results suggest that the MAOA gene is one of the genes playing a modest role in the etiology of a number of the associated behaviors in TS. Substance abuse Prior studies using both enzyme levels6–9 and genetic variants31 have suggested a role of the MAOA gene in substance abuse. The present results are consistent with those conclusions, especially for drug dependence. While MANOVA showed a significant association between the MAOA alleles and both the alcohol and drug scores, there is a great deal of comorbidity of these two forms of substance abuse. As shown in Table 4, when drug dependence and alcohol dependence were examined separately the association was much greater with drug than with alcohol dependence. Male predominance ADHD, Tourette syndrome, conduct disorder, ODD, dyslexia, learning disorders, stuttering, drug dependence and alcoholism all show a male predominance. The molecular genetic studies of the DRD2, DbH, DAT,40 and clinical genetic studies,35–38,64 suggest these are etiologically related spectrum disorders. While the predominance in males is probably due in part to hormonal and environmental factors, X-linked genes could also be a factor. For the TS group, determination of r2 using a regression coefficient, indicated that for the different QTVs the MAOA gene accounted for at most 2.5% or less of the variance of any QTV suggesting that the X-linked MAOA gene does not account for the male predominance of TS, ADHD or related disorders. By contrast, the r2 for the absence or presence of the $335 bp alleles vs the diagnosis of drug dependence, suggested that up to 6.2% of the variance could be due to the MAOA gene. This could play a modest role in the male predominance of drug dependence. Figure 3 Distribution of the means of alcohol, drug and IV drugs (number of drugs used IV) from the ATU group, across the four allele groups of the MAOA VNTR polymorphism. sible to examine these associations using molecular genetic techniques. Tourette syndrome is uniquely suited for such studies because it is highly heritable and is often associated Microsatellites and the regulation of MAO genes Tivol et al65 have recently sequenced the exons of 40 control males who showed a .100-fold variation in MAO A enzyme activity. There was remarkable conservation of the coding sequence. Only five polymorphisms were found. Of these, four involved the third codon position with no change in the amino acid sequence. The other was a neutral lys → arg substitution. For the reasons given in the introduction, we have begun to suspect that the different length alleles of micro- and minisatellite polymorphisms might play a role in the regulation of the genes with which they are associated.47 While the association of the longer mini- 57 MAO genes R Gade et al 58 Table 4 Linear chi square analysis of the number of subjects carrying the $335 bp alleles in the controls vs the ATU subjects without the behavior vs the ATU subjects with the behavior Behavior Drug dep. only IV drug use ODed Barbiturate use DUIs Amphetamine use OSH usea Cocaine use Marijuana use Heroin use Opioid use Alcohol dep. only Controls ATU without ATU with n % n % n % 160 160 160 160 160 160 160 160 160 160 160 160 6.3 6.3 6.3 6.3 6.3 6.3 6.3 6.3 6.3 6.3 6.3 6.3 58 56 71 61 34 19 67 25 14 68 58 98 15.5 14.3 12.7 13.1 8.8 5.3 14.9 12.0 7.1 14.7 15.5 24.5 62 27 25 32 62 77 26 67 82 28 38 22 27.4 29.6 28.0 25.0 21.0 19.5 23.1 19.4 18.3 21.4 18.4 9.1 Chi sq. P 17.4 13.5 11.00 10.56 9.92 9.37 8.96 8.86 8.35 8.05 6.88 non-linear 0.00003 0.00022 0.0009 0.0011 0.0016 0.0022 0.0027 0.003 0.004 0.004 0.009 OSH = other opiates (than heroin or methadone), sedatives and hypnotics. a satellite alleles with specific QTVs in the Tourette syndrome group was modest, as shown in Table 2 and Figure 2, there was a remarkable degree of uniformity in the trends across all the QTVs. Since this could have been a chance, random association, we sought to determine if we could replicate these results in a totally separate group of subjects and controls. This group (the substance abuse group) showed an even stronger association between the longer alleles of the MAOA VNTR, especially the $335 bp alleles, than was observed in the TS group. As shown in Figure 3, the pattern for the two groups is remarkably similar, with the highest scores for $335 bp alleles, modestly higher scores for the lowest size alleles (,320), and intermediate scores for the 334–335 bp alleles. To gain some insight into whether the $335 bp alleles might be associated with a higher or lower MAO-A activity we also genotyped 273 of our males for the Fnu4H1 polymorphism. The linkage disequilibrium with the VNTR allele groups was highly significant (P ,0.000001). As shown in Figure 4, the less common Fnu4H1 2 allele was associated with the ,320 VNTR group while the more common 1 allele was associated with the 320–333, 334 and .335 VNTR groups. Since others (see Introduction) have shown that a range of behavioral disorders are associated with low MAOA activity, and since we observed that the greatest phenotypic effect of the VNTR polymorphism was associated with the $335 bp group, this suggests that this group is also associated with the lowest MAO-A activity. These results indicate that when the subjects carrying the Fnu4H1 1 allele are placed into subgroups on the basis of the VNTR polymorphism, it is the subjects carrying the $335 bp alleles that are driving the Fnu4H1 results. While the ultimate proof of these suggestions will require studies of the VNTR allele in subjects tested for serum or fibroblast MAO-A activity, the findings are consistent with the possibility that the reason the Fnu4H1 polymorphism is associated with differences in MAO-A activity is that the 1 allele is in linkage disequilibrium with the $335 VNTR allele, and the large difference in number of repeats between the ,320 alleles (associated with high MAO-A activity) vs the $335 bp alleles (presumably associated with lowest MAO-A activity) plays a role in the regulation of the MAO-A gene. This correlation with the size of the repeat alleles is consistent with the possibility that the minisatellites themselves might play a role in the regulation of the MAO genes, as reviewed in more detail elsewhere.47 However, it is clear that this does not prove the hypothesis since linkage disequilibrium with another as yet unidentified site could still be occurring. Studies with expression vectors, and the possible interaction of the longer alleles with transcription factors, is needed to prove the case for the MAOA gene. As reviewed in the companion manuscript,47 a number of these studies have been completed with micro- and minisatellites associated with other genes. Polygenic inheritance and small effects It is easy to dismiss the results for the TS group on the basis of the relatively low magnitude of the effect of the MAOA gene on a range of behaviors. Although four variables were significant by MANOVA, two were significant by multivariate regression analysis, and 12 of the 27 were significant by linear ANOVA, one could object that when a complete Bonferroni correction is applied to the ANOVA results none are significant at 0.05/27 or 0.0018. However, this is exactly the point, ie that despite the large literature implicating MAO in different behaviors, when examined at the level of a specific gene polymorphism, the MAOA gene appears to make only a modest contribution to a wide range of behavioral variables. While the effect was much stronger in drug abuse, even here the percent of the variance accounted for by the MAOA alleles was still modest. Replication is an important aspect of associ- MAO genes R Gade et al Acknowledgements Supported in part by the National Institutes of Drug Abuse grant RO1-DA08417 and Tobacco Related Research Disease Program grant 4RT-0110. References Figure 4 Linkage disequilibrium in males only between the MAOA VNTR polymorphism and the Fnu41H polymorphism. Upper panel, number of subjects in the four VNTR groups that carry the Fnu41H 1 or 2 allele. Lower panel, percent of subjects in the four VNTR groups that carry the Fnu41H 1 or 2 allele. ation studies, and these results were found in two completely different sets of subjects. These findings are consistent with the concept of polygenic inheritance in which a number of genes are involved in various behaviors, each with a small effect; and with the hypothesis that the minisatellite polymorphisms themselves may play a role in providing the functional allelomorphic variants fundamental to polygenic inheritance. 1 Ozelius L, Hus Y-PP, Bruns G, Powell JF, Chen S, Weyler W, Utterback M et al. Human monamine oxidase gene (MAOA): chromosome position (Xp21-p11) and DNA polymorphism. Genomics 1988; 3: 53–58. 2 Kochersperger LM, Parker EL, Sicillano M, Darlington GJ, Denney RM. Assignment of genes for human monamine oxidase A and B to the X chromosome. J Neurosci Res 1986; 16: 601–619. 3 Lan CL, Heinzmann C, Gal A, Klisak I, Orth U, Lai E, Grimsley J, Sparkes RS, Mohandas T, Shih JC. Human monamine oxidase A and B genes map to Xp11.23 and are deleted in a patient with Norrie disease. Genomics 1989; 4: 552–559. 4 Grimsby J, Chen K, Wang LJ, Lan N, Shih JC. Human monamine oxidase A and B genes exhibit identical exon-intron organization. Proc Natl Acad Sci USA 1991; 88: 3637–3641. 5 Weyler W, Hsu Y-PP, Breakefield XO. Biochemistry and genetics of monamine oxidase. J Pharmacol Ther 1990; 47: 391–417. 6 Wiberg A, Gottfries CG, Oreland L. Low platelet monoamine oxidase activity in human alcoholics. Med Biol 1977; 55: 181–186. 7 Gottfries CG, Oreland L, Wiberg A, Winblad B. Lowered monoamine oxidase activity in brains from alcoholic suicides. J Neurochem 1975; 25: 667–673. 8 Devor EJ, Cloninger CR, Hoffman PL, Tabakoff B. Association of monoamine oxidase (MAO) activity with alcoholism and alcoholic subtypes. Am J Med Genet 1994; 48: 209–213. 9 Vonknorring AL, Hallmann J, Vonknorring L, Oreland L. Platelet monoamine oxidase activity in type-1 and type-2 alcoholism. Alcohol Alcohol 1991; 26: 409–416. 10 Wyatt RJ, Potkin SG, Murphy DL. Platelet monamine oxidase activity in schizophrenia: a review of the data. Am J Psychiatry 1979; 136: 377–385. 11 Sherif F, Marcusson J, Oreland L. Brain gamma-aminobutyrate transaminase and monoamine oxidase activities in suicide victims. Eur Arch Psychiatry Clin Neurosci 1991; 241: 139–144. 12 Pandey GN, Sharma RP, Janicak PG, Davis JM. Monamine oxidase and cortisol response in depression and schizophrenia. Psychiatry Res 1992; 44: 1–8. 13 Pandey GN, Dorus E, Shaughnessy R, Gaviria M, Val E, Davis JM. Reduced platelet MAO activity and vulnerability to psychiatric disorders. Psychiatry Res 1980; 2: 315–321. 14 Buchsbaum MS, Coursey RD, Murphy DL. The biochemical highrisk paradigm: behavioral and familial correlates of low platelet monoamine oxidase activity. Science 1976; 194: 339–341. 15 Buchsbaum MS, Haier RJ, Murphy DL. Suicide attempts, platelet monamine oxidase and the average evoked response. Acta Psychiatr Scand 1977; 56: 69–79. 16 Meltzer HY, Arora RC. Platelet markers of suicidality. Ann N Y Acad Sci 1986; 487: 271–280. 17 Skekim WO, Davis LG, Bylund DB, Brunngraber E, Fikes L, Lanham J. Platelet MAO in children with attention deficit disorder and hyperactivity: a pilot study. Am J Psychiatry 1982; 139: 936–938. 18 Schooler C, Zahn TP, Murphy DL, Buchsbaum MS. Psychological correlates of monoamine oxidase activity in normals. J Nerv Ment Dis 1978; 166: 177–186. 19 Shekim WO, Bylund DB, Frankel F, Alexson J, Jones SB, Blue LO, Kirby J, Corchoran C. Platelet MAO activity and personality variations in normals. Psychiatry Res 1989; 27: 81–88. 20 Vonknorring L, Oreland L, Winblad B. Personality traits treated to monoamine oxidase activity in platelets. Psychiatry Res 1984; 12: 11–26. 21 Mann JJ, Stanley M. Postmortem monoamine oxidase enzyme kinetics in the frontal cortex of suicide victims and controls. Acta Psychiatr Scand 1984; 69: 135–139. 22 Propping P, Rey ER, Friedl W, Beckmann H. Platelet monoamine oxidase in healthy subjects: the ‘biochemical high-risk paradigm’ revisited. Arch Psychiatr Nervenkr 1981; 230: 209–219. 59 MAO genes R Gade et al 60 23 Tabakoff B, Hoffman PL, Lee JM, Saito T, Willard B, Leon-Jones FD. Differences in platelet enzyme activity between alcoholics and nonalcoholics. New Eng J Med 1988; 318: 134–139. 24 Fowler CJ, Tipton KF, MacKay AVP, Youdin BH. Human platelet monoamine oxidase—a useful enzyme in the study of psychiatric disorders. Neuroscience 1982; 7: 1577–1594. 25 Hotamisligil GS, Breakefield XO. Human monoamine oxidase A gene determines levels of enzyme activity. Am J Hum Genet 1994; 49: 383–392. 26 Lin LCC, Powell JF, Murray R, Gill M. Monoamine oxidase A gene and bipolar affective disorder. Am J Hum Genet 1994; 54: 1122– 1124. 27 Craddock N, Daniels J, Roberts E, Rees M, McGuffin P, Owen MJ. No evidence for allelic association between bipolar disorder and monoamine oxidase A gene polymorphisms. Am J Med Gen (Neuropsych Genet) 1995; 60: 322–324. ¨ 28 Nothen MM, Eggerman K, Albus M, Borrmann M, Rietschel M, ¨ Korner J, Maier W, Minges J, Lichtermann D, Franzek E, Weigelt B, Knapp M, Propping P. Association analysis of the monamine oxidase A gene in bipolar affective disorder by using family-based internal controls. Am J Hum Genet 1995; 57: 975–977. 29 Brunner HG, Nelen MR, van Zandvoort P, Abeling NGGM, van Gennip AH, Wolters EC, Kuiper MA, Ropers HH, van Oost BA. Xlinked borderline mental retardation with prominent behavioral disturbance: phenotype, genetic localization and evidence for disturbed monoamine metabolism. Am J Hum Genet 1993; 52: 1032–1039. 30 Brunner HG, Helen M, Breakefield XO, Ropers HH, van Oost BA. Abnormal behavior linked to a point mutation in the structural gene for monamine oxidase A. Psychiat Genet 1993; 3: 122. 31 Vanyukov MM, Moss HB, Plail JA, Blackson T, Mezzich AC, Tarter REI. Antisocial symptoms in preadolescent boys and in their parents: associations with cortisol. Psychiatr Res 1993; 46: 9–17. 32 Black GCM, Chenz Y, Craig IW, Powell JF. Dinucleotide repeat polymorphism at the MAOA locus. Nucleic Acids Res 1991; 19: 689. 33 Comings DE. The role of genetic factors in conduct disorder based on studies of Tourette syndrome and ADHD probands and their relatives. J Dev Behav Pediatr 1995; 16: 142–157. 34 Comings DE. The role of genetic factors in human sexual behavior based on studies of Tourette syndrome and ADHD probands and their relatives. Am J Med Gen (Neuropsych Genet) 1994; 54: 227– 241. 35 Comings DE. Genetic factors in substance abuse based on studies of Tourette syndrome and ADHD probands and relatives. I. Drug abuse. Drug and Alcohol Dependence 1994; 35: 1–16. 36 Comings DE. Genetic factors in substance abuse based on studies of Tourette syndrome and ADHD probands and relatives. II. Alcohol abuse. Drug and Alcohol Dependence 1994; 35: 17–24. 37 Comings DE. Tourette syndrome: a hereditary neuropsychiatric spectrum disorder. Ann Clin Psychiatry 1995; 6: 235–247. 38 Biederman J, Newcorn J, Sprich S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am J Psychiatry 1991; 148: 564–577. 39 Hinds HL, Hendricks RW, Craig IW, Chen ZY. Characterization of a highly polymorphic region near the first exon of the human MAOA gene containing a GT dinucleotide and a novel VNTR motif. Genomics 1992; 13: 896–897. 40 Comings DE, Wu H, Chiu C, Ring RH, Dietz G, Muhleman D. Polygenic inheritance of Tourette syndrome, stuttering, ADHD, conduct and oppositional defiant disorder: the additive and subtractive effect of the three dopaminergic genes—DRD2, DbH and DAT1. Am J Med Gen (Neuropsych Genet) 1996; 67: 264–288. 41 Comings DE, MacMurray JP, Gade R, Muhleman D, Peters WR. Genetic variants of the human obesity gene: association with psychiatric symptoms and body mass index in young women, and interaction with the dopamine D2 receptor gene. Mol Psychiatry 1996; 1: 325–335. 42 Johnson JP, Muhleman D, MacMurray J, Gade R, Verde R, Ask M, Kelley J, Comings DE. Association between the cannabinoid recep- 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 tor gene (CNR1), and the P300 wave of event-related potentials, and drug dependence. Mol Psychiatry 1997; 2: 169–171. Comings DE, Muhleman D, Gade R, Johnson P, Verde R, Saucier G, MacMurray J. Cannabinoid receptor gene (CNR1): association with IV drug use. Mol Psychiatry 1997; 2: 161–168. Comings D, Gade R, Muhleman D, MacMurray J. Role of the HTR1A serotonin receptor gene in Tourette syndrome and conduct disorder. Psychiat Genet 1996; 6: 166. MacMurray J, Saucier G, Muhleman D, Gade R, Chiu C, Wu S, Blake H, Ferry L, Johnson J, Comings DE. Polygenic prediction of parity: GABAA-b3 and dopamine DRD4 gene markers. Psychiat Genet 1996; 6: 161. Gade R, Blake H, MacMurray J, Muhleman D, Johnson J, Verde R, Comings D. Relationship of the GABRB3 gene to adult ADHD and personality traits in Caucasian and African-American samples. Psychiat Genet 1996; 6: 164–165. Comings DE. Polygenic inheritance and micro/minisatellites. Mol Psychiatry 1998; 3: 21–31. Schroth GP, Chou P-J, Ho PS. Mapping Z-DNA in the human genome. J Biol Chem 1992; 267: 11846–11855. Rich A, Nordheim A, Wang AJ. The chemistry and biology of lefthanded Z-DNA. Annu Rev Biochem 1984; 53: 791–856. Comings DE. Polygenic inheritance and minisatellites. Psychiat Genet 1996; 6: 157–158. Comings DE. Polygenic inheritance of psychiatric disorders. In: Blum K, Noble EP, Sparks RS, Sheridan PJ (eds). Handbook of Psychiatric Genetics. CRC Press: Boca Raton, FL, 1996, pp 235–260. Comings DE. Tourette Syndrome and Human Behavior. Hope Press: Duarte, CA, 1990, pp 1–828. Comings DE, Gade R, Wu S, Chiu C, Dietz G, Muhleman D, Saucier G, Ferry L, Burchete R, Johnson P, Verde R, MacMurray JP. Studies of the potential role of the dopamine D1 receptor gene in addictive behaviors. Mol Psychiatry 1997; 2: 44–56. Robins LN, Helzer J, Croughan J, Ratclif KS. National Institute of Health diagnostic interview schedule. Arch Gen Psychiatry 1981; 38: 381–389. Diagnostic and Statistical Manual of Mental Disorders. 3rd edn, revised. American Psychiatric Association: Washington, DC, 1987. Comings DE. Genetic factors in depression based on studies of Tourette syndrome and Attention Deficit Hyperactivity Disorder probands and relatives. Am J Med Gen (Neuropsych Genet) 1995; 60: 111–121. Gadow KD, Sprafkin J. Child Symptom Inventories Manual. Checkmate Plus Ltd: Stony Brook, NY, 1994, pp 1–115. Grayson P, Carlson G. The utility of a DSM-III-R based checklist in screening child psychiatric patients. J Am Acad Child Adolesc Psychiatry 1991; 30: 669–673. Davis LL, Hurt RD, Morse RM, O’Brien PC. Discriminant analysis of the self-administered alcoholism screening test. Alcoholism: Clinical & Experimental Research 1987; 11: 269–273. Hodgins DC, Guebaly N. More data on the Addiction Severity Index. Reliability and validity with the mentally ill substance abuser. J Nerv Ment Dis 1992; 180: 197–201. Mullis K, Faloona F, Scharf S, Saiki R, Horn G, Erlich H. Specific enzymatic amplification of DNA in vitro: the polymerase chain reaction. Cold Spring Harbor Symp Quant Biol 1986; 51: 263–272. Comings DE, Muhleman D, Gade R, Chiu C, Wu H, Dietz G, WinnDean E, Ferry L, Rosenthal RJ, Lesieur HR, Rugle L, Sverd J, Johnson P, MacMurray JP. Exon and intron mutations in the human tryptophan 2,3-dioxygenase gene and their potential association with Tourette syndrome, substance abuse and other psychiatric disorders. Pharmacogenetics 1996; 6: 307–318. Comings DE. Search for the Tourette Syndrome and Human Behavior Genes. Hope Press: Duarte, CA, 1996. Comings DE, Comings BG. A controlled study of Tourette syndrome. I. Attention-deficit disorder, learning disorders, and school problems. Am J Hum Genet 1987; 41: 701–741. Tivol EA, Shalish C, Schuback DE, Hus Y-P, Breakefield XO. Mutational analysis of the human MAOA gene. Am J Med Gen (Neuropsych Genet) 1996; 67: 92–97.