Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of beta-blockers wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
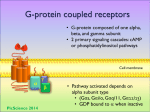
Prescription costs wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Drug design wikipedia , lookup
Toxicodynamics wikipedia , lookup
NMDA receptor wikipedia , lookup
Pharmacognosy wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug discovery wikipedia , lookup
Drug interaction wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Psychopharmacology wikipedia , lookup
Nutrition and Pharmacology Lecture 1 Pharmacology = study of the effects of drugs on living systems, aiming to improve their functioning Primary aim: To study and evaluate effects of bio-active compounds in the diet with the purpose of improving health and preventing or curing disease Secondary aims: To study the relation and interactions between food and drugs from a clinical and public health perspective & To translate expertise, models and techniques between the two disciplines Naproxen-sodium = a medicine (drug) = “Any substance or combination of substances which may be administered to human beings with a view to making a medical diagnosis or to restoring, correcting or modifying physiological functions in human beings” (Substantie of samenstelling van substanties, welke is bestemd te worden gebruikt of op enigerlei wijze wordt aangeduid of aanbevolen als zijnde geschikt voor: 1. Het genezen, lenigen of voorkomen van enige aandoening, ziekte, ziekteverschijnsel, pijn, verwonding of gebrek bij de mens, 2. Het herstellen, verbeteren of wijzigen van het functioneren van organen bij de mens, 3. Het stellen van een medische diagnose door toediening aan of aanwending bij de mens) = a drug is a substance of known structure, other than a nutrient or an essential dietary ingredient, which when administered to a living organism, produces a biological effect Indications: Headaches, Toothaches, Menstrual cramps, Muscular pains, Backache (lumbago), For relief of the signs and pain in influenza and after vaccination Medicines need approval: by national authorities (=CBG in NL) or European (EMA). Each medicine allowed to be sold in NL should have a unique registration code: Nationally approved (RVG code), Homeopathic medicines (RVH code) and European registration (EU code). 1 * Nonsteroidal anti-inflammatory drug (NSAID) bind to cyclooxygenase (=prostaglandin endoperoxide H synthase PGHS) * Analgesic and antipyretic properties What are cyclooxygenases and what are they doing? Phospholipase A2 Omega 6 Prostaglandins: inflammatory mediators PGE2 causes fever, headache, vasodilation, vasoconstriction = symptoms of inflammation. TxA2 causes platelet aggregation you want to inhibit that if you’re at risk for CVD. COX 1 is always there (in mucus layer of stomach) = constitutively expressed COX 2 is only there when there‘s inflammation. 2 When taking medicines like ibuprofen etc. you can have problems with your stomach; because of the inhibition of the protective prostaglandins. There’s a difference in the active site of COX 1 and COX 2 that allowed the design of selective inhibitors (but that went wrong…) The spectrum of selectivity for COX inhibition The lower the IC50, the more potent the inhibition is. So Diclofenac is a very potent COX-1 and COX-2 inhibitor Diclofenac is very active. Together with these medicines, you have to take gastrointestinal protector medicines. Dosage form Drug substances are rarely administered alone, but as a part of a formulation or dosage form. Formulation can have varied and specialized pharmaceutical functions. Formulation: “Coated tablet” and here: “enteric coated” Coating protects core in the stomach. Drug released in the upper GI tract after the stomach; so by coating you protect the drug from the stomach’s acid. 3 Different process phases in pharma: Intravenous injection Intramuscular injection Subcutaneous injection The easiest way to apply a drug into the blood is via the i.v. injection. Other ways have an extra barrier and thus take some extra steps. Basics of oral drug absorption: - Mostly in duodenum - Drug should be in dissolved state - Often by passive diffusion (.....polarity, pKa etc.) - Sometimes active transport involved - Lipid soluble compounds (partly) with lipids - Metabolism in intestinal wall can be considerable It has to be in a solution to be absorbed. The speed at which the tablet disintegrates (in water) can be a rate limiting step. ‘Een ketting is niet sterker dan de zwakste schakel’ 4 Naproxen is disintegrated, gets into your gut and will be absorbed. It can bind to i.e. fibres in the stomach (food-drug interactions). It can be metabolized by the gut wall. Then it gets in the liver. The liver gets biotransformation (first pass effect). Then it gets into the systemic circulation. Naproxen in three different doses. => Typical absorption curve (it takes a while before you get a maximum) (It’s not i.v. because it would start high from beginning) Tmax=time at which you get max. plasma conc (Cmax) MTC=minimum toxic concentration MEC=minimum effective concentration You want to stay as long as possible above the MEC and not above the MTC. Biotransformation Phytotherapeutics: In NL mostly regulated as “food supplements” Food supplements, “functional” foods, but also “normal” food products may carry Nutrition and/or Health claims (or indirectly like ‘Slankie’ = not allowed). 5 Lecture 2 Pharmacodynamics - The molecular action of a drug / bioactive is often explained by- and predicted from a receptor concept - Receptors : macromolecules including enzymes, transporters, structures on cell membranes, transcription factors, nucleotides etc. - Receptors are mostly normal regulatory structures playing a role in the physiology of the organism. - Natural ligands: neurotransmitters, hormones or other signalling molecules. - Drugs just bind by coincidence or by design to these receptors. Receptors and ion channels are ‘real’ receptors. Different classes of receptors: * Multi-subunit ion channels (=Ligand-gated ion channels) Located: Cell surface transmembrane Examples of ligands: Acetylcholine (nicotinic), GABA, Glutamate, Glycine GABA A receptor GABA is the major inhibitory neurotransmitter in the central nervous system. Benzodiazepines enhance the response to GABA. They act allosterically on the receptor. * G-protein– coupled receptors Located: Cell surface transmembrane Examples of ligands: Acetylcholine (muscarinic), a- and ßAdrenergic, Eicosanoids 6 * Protein kinases Located: Cell surface transmembrane Examples of ligands; Growth factors, Insulin, Peptide hormones * Transcription factors Located: Cytoplasm Examples of ligands: Steroid hormones, Thyroid hormone, Vitamin D G-protein coupled receptors (GPCRs) One of most important targets for today’s drugs Very large family (~950 genes in human genome) of regulatory proteins (including olfactory, taste, light, endogenous compounds etc.) 7TM receptor structure GTP-GDP reaction Three key (others exist) targets for G-proteins translate the signal: Adenylate cyclase/ cAMP Phospholipase C/IP3/DAG Ion Channels (many) GPCR’s G-proteins are heterotrimers, with 3 subunits: α, β, γ A G-protein that activates cyclic-AMP formation within a cell is called a stimulatory G-protein, designated Gs with alpha subunit Gsa. Gs is for example activated by receptors for the hormones epinephrine (adrenalin) and glucagon. How is the signal turned off? > Ga hydrolyses GTP to GDP + Pi. (GTPase). The presence of GDP on Ga causes it to rebind to the inhibitory βγ complex. Adenylate Cyclase is no longer activated. > Phosphodiesterase catalyses hydrolysis of cAMP AMP. > Receptor desensitization occurs (varying with the ligand) 7 • Some receptors are phosphorylated via specific receptor kinases. • The phosphorylated receptor may then bind to a protein b-arrestin, that promotes removal of the receptor from the membrane by clathrin-mediated endocytosis. Example: β2-adrenergic receptor Pharmacology of Asthma: recurrent and reversible airway obstruction • Inflammatory changes in the airways • Bronchial hyper-responsiveness • Attack in two phases Pharmacological targets: • Reduction of inflammatory response • Bronchodilatation - β2 – adrenergic agonists relax smooth muscle - Short acting (salbutamol, terbutaline) or long acting (salmeterol, formoterol etc.) - Usually given as local formulation - Use depends on type of asthma, often combined with glucocorticoids - Sometimes: Muscarinic receptor antagonist (ipratropium) - Not common anymore: PDE inhibitor (theophylline) There are also inhibitory G-proteins . The stimulatory Gsα, when it binds GTP, activates Adenylate cyclase. . An inhibitory Giα, when it binds GTP, inhibits Adenylate cyclase. Different effectors & their receptors induce Giα to exchange GDP for GTP than those that activate Gsα. In some cells, the complex of Gβγ that is released when Ga binds GTP is itself an effector that binds to and activates other proteins. Example: Cannaboid receptor • Important endogenous regulation system • two G-protein coupled receptors described so far (CB1 and CB2) •Many endogenous and exogenous cannabinoids •Specific transporters Appetite stimulation, hallucinogenic & euphoric, antiinflammatory, psychosis risk? anti-tumour? 8 We have our own endocannabinoid system (ECS): The ECS is a highly important regulation system in our body (metabolism, immune defence, pain) Endocannabinoids are formed from fatty acids (lipid-like molecules) controls dietary fat intake The ECS offers many opportunities for disease management and prevention (Endo)cannabinoids: plant-derived (THC) or synthesized from fatty acids. CB1 in brain: regulates food intake, rewards high-caloric foods (makes you eat a lot of these) and stores it as fat Weight loss by CB1 blockade solution that’s too simple (side effects) Summary overview: Gi and Gs G-protein coupled receptors Bidirectional control of a target enzyme, such as adenylated cyclase by Gs and Gi. Heterogeneity of G-proteins allows different receptors to exert opposite effects on a target enzyme. 2-nd important effector pathway for GPCRs: The phospholipase C/inositol triphosphate (IP3)/diacylglycerol (DAG) pathway - When a particular GPCR is activated, GTP exchanges for GDP. Gqα-GTP activates Phospholipase C - Phospholipase C catalyses cleavage of PIP2 and this yields 2 second messengers: • inositol-1,4,5-trisphosphate (IP3) and • diacylglycerol (DAG). - Diacylglycerol, with Ca++, activates Protein Kinase C, which catalyses phosphorylation of several cellular proteins, altering their activity. Example: acetylcholine muscarinic M1 receptor (in brain) 9 Quantitation of dose-response relations A. is most potent Antagonist gives no signal and also inhibits the action of an inverse agonist. Three types of ligands: 1. agonists are ligands which shift the equilibrium in favor of the active state. 2. inverse agonists are ligands which shift the equilibrium in favor of inactive states. 3. neutral antagonists are ligands which do not affect the equilibrium. Inverse agonism: benzodiazepines and GABA 10 ADME/Pharmacokinetics ADME=Absorption, Distribution, Metabolism, Excretion Medicines are administered via different routes > Active substances meet different barriers > Consequences for effect (onset, duration etc.) > Rate-limiting steps are determining ultimate effect (-rate) How do compounds cross the intestinal epithelium? Active transporter proteins in intestinal epithelial cells 11 Drugs and other compounds are often metabolised in gut, liver (and elsewhere) Biotransformation processes Biotransformation in liver CYTOCHROME P450 (CYP450) Expression/activity dependent on: genetics, gender, age, diet, smoking, environment, diseases, medicines etc. 12 Lecture 3 pH dependent drug dissolution, absorption and distribution Many drugs are acids, bases or salts Basic compound: when you put it in water, pH will be >7 Hydrophilicity/lipophilicity (and water solubility) are pH dependent Examples: - Naproxen-Na - Amoxicillin-Na - Morphine-HCl - Salbutamol-sulphate - Tetracycline-HCl - Atropine-sulphate Penetration through membranes is dependent on pH. 13 4.16/2.26=2.. 2x more morphine in plasma This accumulation is sometimes called ion-trapping Ion trapping can be used to distribute drugs into the urinary compartment to increase /decrease the urinary excretion of poisons/drugs etc. - Alkalinisation of the urine (by administration of sodium bicarbonate) to increase urinary excretion of acetyl salicylic acid - Idem to reduce urine levels of illicit drugs with basic properties (cocaine, amphetamine, morphine..) Pharmacokinetics * To understand quantitative dose-effect relations * To estimate and individualize dosage regimens * To predict effect of co-medication, disease etc. Compound A which is given IV at dose of 50 mg This simple straight line can be expressed as: Per unit of time a constant amount of compound is eliminated from the plasma This is called “zero-order” kinetics (saturation kinetics) Observed when rate limiting processes are operating under “Vmax conditions” Examples: phenytoin, salicylate, ethanol and other compounds at high (toxic) compounds 14