Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Rheumatic fever wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Rheumatoid arthritis wikipedia , lookup
Immunocontraception wikipedia , lookup
Immune system wikipedia , lookup
Innate immune system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Systemic lupus erythematosus wikipedia , lookup
Autoimmunity wikipedia , lookup
Complement system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Monoclonal antibody wikipedia , lookup
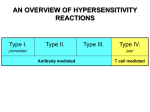
HYPERSENSITIVITY REACTIONS HYPERSENSITIVITY REACTIONS Innocous materials can cause hypersensitivity in certain individuals leading to unwanted inflammation damaged cells and tissues Non-proper reaction of the immune system to foreign substances Mainly harmless substances – after second or multiple exposure AN OVERVIEW OF HYPERSENSITIVITY REACTIONS Type I. Type II. „immediate” Type III. Type IV. „late” Antibody mediated T cell mediated TYPES OF ANTIBODY MEDIATED HYPERSENSITIVITY REACTIONS FcRIα) TYPE I HYPERSENSITIVITY REACTION ALLERGY SENSITISATION PROCESS MAST CELL RESPONSE TO SURFACE FcRεI CROSSLINKING IgE a g b I I TT AA MM PLA2 foszfa tidil-kolin LYSO-PC arachidonsav Fc eRI I T A M MAPkináz I T A M Lyn II TT AA MM Syk endoplazmás retikulum 2 Ca + 5-lipoxigenáz PIP2 PI-PLCg DAG IP3 foszfolipid ciklooxigenáz Ca 2+ PGD2 citokin gének transzkripciója LTC4 NFAT AP-1 NF-k B PAF szekretoros granulum 2+ PKC Ca Ca 2+ proteinek (miozinkönnyűlánc) foszforilációja Ca 2+ szekréció PGD2 LTC4 LTD4 LTE4 LATE MEDIATORS mediátorok EARLY MEDIATORS citokinek IL-3, IL-4, IL-5, IL-6 TNFa Biogenic amins – histamin Enzymes – triptase, chymase, carboxypeptidase THE EFFECT OF MAST CELL DEGRANULATION VARIES WITH THE TISSUE EXPOSED TO ALLERGEN SYSTEMIC ANAPHYLAXIS IS CAUSED BY ALLERGENS THAT REACH THE BLOOD STREAM TYPES OF IgE-DERIVED ALLERGIC RESPONSES SYNDROME ALLERGENS ROUTE OF ENTRY RESPONSE systemic anaphylaxis drugs anti-serum intravenous acute urticaria bug bite allergy test subcutan local increase in blood flow and vascular permeability allergic rhinitis pollen dust mite drops inhaled irritation and edema of nasal mucosa airway inflammation asthma animal fur pollen dust mite drops inhaled bronchial constriction, increased mucus production food allergy nut, peanuts, fish, shellfish milk, eggs oral vomiting, diarrhea pruritis (itching) urticaria (hives) anaphylaxia (rare) edema, increased vascular permeability tracheal occlusion circulatory collapse, death Short/Common ragweed (Ambrosia artemisiifolia) Short/Common ragweed (Ambrosia artemisiifolia) Green leaf back Mugwort (Artemisia vulgaris) White leaf back Mugwort (Artemisia vulgaris) – ? Wormwood (Artemisia absinthium) – Absinthe (thujone: max 35 mg/l) MAST CELL DEGRANULATION, ALLERGIC REACTION IN THE SKIN OF A SENSIBILIZED INDIVIDUAL PRICK TEST Prick test ImmunoCAP Specific IgE Blood Test Anti-IgE Serum IgE Allergen Solid phase COMPARISON OF SKIN TEST TO SPECIFIC IgE TESTING allergens speed (result) medication disease cost sensitivity Skin Prick test Specific IgE many 20 min almost all 1-2 days no antihistamines severe eczema: difficult € 20 (total) high no problem no problem € 20 per specific IgE slightly lower TYPE II HYPERSENSITIVITY IgG type antibodies bound to cell surface or tissue antigens • cells expressing the antigen become sensitive to complement mediated lysis or to opsonized phagocytosis • frustrated phagocytosis tissue damage • the antibody inhibits or stimulates target cell function no tissue damage (e.g. M. gravis – receptor-blocking antibodies) MECHANISMS OF TYPE II HYPERSENSITIVITY REACTIONS NK Mf Killing of target cell by effectormacrophage or NK-cell IgG ADCC IgG C' complement activation Killing of target cell by complementmediated lysis Receptor-specific autoantibody interferes with signal transduction FRUSTRATED PHAGOCYTOSIS MEDIATED BY IgG TYPE ANTIBODIES Binding Opsonization Internalization C3b C3b C3b C3b Enzyme release C3b C3R FcR The tissue, which can not be phagocytosed, is damaged C3b Absorbed antigen Opsonized surface Binding Frustrated (drug) phagocytosis Enzyme release EXAMPLES - TYPE II HYPERSENSITIVITY Newborn haemolytic anaemia Transfusion reaction Hyperacut allograft rejection Drug-derived • Haemolitic anaemia • Thrombocytopenia • Agranulocytosis • • Penicillin-based antibiotics Anti-arithmic quinidine Goodpasture syndrome (kidney, basal membrane - collagen type IV) Pemphigus vulgaris (mucosal bubbles) against desmosomal antigens, interruption of epidermal and mucosal connections, acantolysis (desintegration into single cells) Myasthaenia gravis (anti-acetyl-choline receptor antibodies) Graves-Basedow-Flajani disease (anti-TSH-receptor antibodies) DEVELOPMENT OF DRUG SENSITIVITY I. DEVELOPMENT OF DRUG SENSITIVITY II. TYPE III HYPERSENSITIVITY Antibodies binding to soluble antigens forming small circulating immune complexes which are deposited in various tissues Depends on: Size of immune complexes Antigen-antibody ratio Affinity of antibody Isotype of antibody THE PROCESS OF TISSUE DAMAGE CAUSED BY IMMUNE COMPLEXES Antigen C' Immune complex Antibody Complementa ctivation (C3a , C5a ) PMN Chemotaxis C' Endothelium Ba sophil Ba sa l membra ne gra nulocyte Vessel wa ll Thrombocytes Deposition Blood vessel wall permeability Frustrated phagocytosis Vasoactive a mines Immune complexes activate the complement system, neutrophils, basophils and thrombocytes SYPMPTPOMES CAUSED BY TYPE III HYPERSENSITIVITY REACTIONS DEPEND ON THE SITE OF IMMUNECOMPLEX DEPOSITION ARTHUS-REACTION • Localized Type III hypersensitivity • Local vasculitis develops as a result of immune complex deposition • Inhaled antigens (fungi, animal feces) may induce similar reaction in the lung • IgG type antibody • ‘Farmers lung’ and ‘piegeon-breeder’s lung’ MANIFESTATION OF TYPE III HYPERSENSITIVITY IN LUPUS ERYTHEMATOSUS Facial, malar "butterfly" rash with characteristic shape across the cheeks. Discoid lupus erythematosus (DLE) involves mainly the skin, it is relatively benign compared to systemic lupus erythematosus (SLE). In either case, sunlight exposure accentuates this erythematous rash. A small number (5 to 10%) of DLE patients go on to develop SLE (usually the DLE patients with a positive ANA). Here is a more severe inflammatory skin infiltrate in the upper dermis of a patient with SLE in which the basal layer is undergoing vacuolization and dissolution, and there is purpura with RBC's in the upper dermis (which are the reason for the rash). DEPOSITION OF IMMUNE COMPLEXES IN THE SKIN OF SLE PATIENTS When immunofluorescence staining with an antibody to complement or immunoglobulin is performed, a brightly fluorescent signal staining the dermal epidermal junction is visible indicating immune complex deposition. Immunofluorescence staining pattern with antibody to IgG staining immune complexes at the dermal-epidermal junction. If such a pattern is seen only in skin involved by a rash, then the diagnosis is probably DLE, but if this pattern appears even in skin uninvolved by a rash, then the diagnosis is SLE. RENAL FAILURE IN IMMUNECOMPLEX DISEASES Glomerulus of a healthy individual. Relatively wide spaces between capillary loops. One of the feared complications of the systemic autoimmune diseases is renal failure. This is most likely to occur in SLE. Here is a glomerulus in which the capillary loops are markedly pink and thickened such that capillary lumens are hard to see. This is lupus nephritis. ANA Anti-nuclear antibody This is the so-called "nucleolar pattern" of staining in which the bright fluorescence is seen within the nucleoli of the Hep2 cells. This pattern is more suggestive of progressive systemic sclerosis. This is the so-called "rim" pattern that is more characteristic of SLE. This is the so-called "speckled" pattern of staining which is more characteristic of the presence of autoantibodies to extractable nuclear antigens, particularly ribonucleoprotein. This pattern is not very specific, but may be seen with an entity called "mixed connective tissue disease" which is a mix between SLE, scleroderma, and polymyositis, but without serious renal or pulmonary disease. The autoimmune diseases are very hard to classify, even for the experts. TYPE IV HYPERSENSITIVITY REACTION T CELL MEDIATED PROCESS TYPE IV HYPERSENSITIVITY REACTION Chemokines, cytokines, cytotoxins DELAYED-TYPE (TYPE IV) HYPERSENSITIVITY DELAYED-TYPE (TYPE IV) HYPERSENSITIVITY DELAYED-TYPE HYPERSENSITIVITY (DTH) (e.g. tuberculin skin test) TH1 from a previous immunization (memory) Tuberculin skin test Introduction of Ag Ag = antigen Purified protein derivate (PPD) CHEMICAL MEDIATORS OF DTH DTH as a result of a contact-sensitizing agent* CONTACT DERMATITIS *a contact-sensitizing agent is usually a small molecule that penetrates the skin then binds to self-proteins, making them “look” foreign Poison ivy Anacardiaceae (family), Toxicodendron (genus) Toxicodendron radicans or Rhus toxicodendron Delayed-type hypersensitivity is mediated by T cells CELIAC DISEASE