Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Innate immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Molecular mimicry wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Complement system wikipedia , lookup
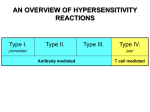
Chapter 17 Hypersensitivity 1 Types of hypersensitivity • Type I – immediate Due to IgE binding to Fc receptors on mast cells and basophils. • Type II - Antibody-Mediated Cytotoxic Due to antibody (IgG and IgM) mediated activation of complement or antibody dependent cell mediated cytotoxicity (ADCC). • Type III - Immune Complex–Mediated Due to accumulation of immune complexes and the resulting inflammatory response. • Type IV -Delayed-Type(DTH)Due to activation of TDTH cell mediated effectors. 2 Section II Type II hypersensitivity IgG or IgM bind to the Ag on the surface of target cells to activate complement, phagocytes, NK cells. As soon as Ag are cleared, the target cells and tissue are damaged by abnormal response. 3 I. Mechanism 1.Ag : on the surface of target cells 2.Ab : IgG and IgM 3.Cell damaged by complement, macrophage, NK cell et al. 4 Ag on the surface of the cell or hapten adsorbed on the surface of the cell + Specific Ab (IgG, IgM) Complement activation Lysis of target cell Opsonization Phagocytose of target cell NK cell phagocyte ADCC Stimulate or block receptor function Target cell dysfunction Target cell damage The mechanism of type II hypersensitivity 5 Mechanisms of Type II hypersensitivity B cell TH2 6 Host target cell Complement activation C1 C2 C4 C3 C3b & C5b C3a & C5a C5-C9 Host target cell 7 Opsonization Target cell C3b Antibody Lysosomal enzymes Phagocyte 8 ADCC NK Antibody Fc receptor Perforin and enzymes Host Target cell 9 Mechanisms of Type II hypersensitivity C activation Opsonization ADCC 10 II. Disease 1. Blood transfusion reactions Transfused cells are killed by complement-mediated lysis Symptoms: Fever, chills, nausea, clotting within vessels and lower back pain. Increased hemoglobin can lead to a buildup of bilirubin which can be toxic at high concentrations. Treatment: Stop the transfusion! Provide diuretic to increase urine output and reduce buildup of hemoglobin. 11 2. Hemolytic disease of the newborn 12 • Prevention :Hemolytic anemia of the newborn can be prevented by treating the mother with an anti-Rh antibody (Rhogam) within 72 hours after the first Rh+ child was born. • Rhogam binds to Rh on the fetal cells to eliminate Rh+ fetal RBC before B cell activation occurs. 13 3. Drug induced hemolytic anemia Drug (half Ag, penicillin) + membrane of RBC produce self Ab damage RBC 14 4. Drug allergy blood cells reduce disease 5. Goodpasture’s syndrome 6. Graves ′ disease (Thyroid Stimulating Hormone, TSH), high level thyroxine Normal: TSH+TSH-R induce T3, T4 production _ Abnormal: Anti-TSH-R+TSH-R induce T3,T4 production 15 16 17 18 Section III Type III hypersensitivity Immune complexes mediated reaction. In some case, such as high level antigen or phagocytosis deficiency, body can not clear these ICs in time. Through activating complement, neutrophil, platelet, basophil, the ICs induce erythema, edema, local tissue necrosis, and neutrophil homing. 19 I. Mechanism 1. Ag: soluble Ag. 2. Ab: IgG , IgM. 3.Immune complex. Big size IC: phagocytosis Medium size: deposit Small size: clear with urine 4. Tissue damage Complement, neutrophil, platelet, et al. 20 Ag + Ab Large IC Small IC Medium IC Immune complex , IC Phagocytosis by phagocytes Discharged from circulation Exist in circulation, and deposit 21 Immune complex deposit Activating complement Mediated mast-cell and basophil C3a, C5a, C567 Activating platelet, star blood coagulation Chemotaxis Neutrophil infiltrating Releasing vasoactive mediators Microthrombosis Releasing lysosomal Capillary permeability Tissue ischemia, necrosis edema Vasculitis 22 Type III Hypersensitivity Neutrophil C3a & C5a C3 C3b & C5b C4 C2 C1 C5-C9 23 24 25 26 II. Disease 1. Local IC disease ① Arthus reaction Arthus-like reaction 27 ② Human local IC disease 接种乙肝后第8天发生的Arthus反应 28 2. General immune complex disease ① serum disease Serum sickness can occur at 7-10 days after anti-serum injection. Antibodies were produced before antiserum was eliminated. The binding of antibodies to antiserum forms immune complexes The deposition of IC causes serum sick: fever, chills, rash, arthritis and sometimes glomerulonephritis. 29 ② Systemic lupus erythematosus (SLE) • Degraded DNA or RNA stimulate B cell to produce antibody ( anti-nuclear Ab ) • Formation and deposition of Ag-Ab complex 30 ③ Rheumatoid arthritis Degraded IgG stimulate B cell to produce IgM antibody ( Rhemotiod factor ) Formation and deposition of Ag-Ab complex 31 ④ Post-streptococcal glomerulonephritis •Streptococcal M protein stimulate B cell production •Formation of Ag-Ab complex and deposition in kedney Fluorescence Ab 32 Section IV Type IV hypersensitivity 33 • Type IV hypersensitive reaction develop when antigen activates sensitized TDTH cells (delayed type hypersensitivity, DTH); • Th1 • Tc • The hallmark of a type IV reaction are the delay in time required for the reaction to develop and the recruitment of macrophages. The symptoms usually reach maximum after 24h-72h after touching the antigens. 34 I. Mechanism Antigen: intracellular microbes Antibody: no Complements: no Cells: T cells, macrophages 35 Inducing Antigen T cell (CD4+,CD8+) Cytokine Il-2 CD4+ T cell IFN-γ TF T cell proliferation Tissue lesion TNF-β Monocyte infiltration Exudation MCF Re-exposure MIF Cytotoxicity Sensitized T cell (CD4+,CD8+) CD8+ T cell Killing target cell 1. Sensitization phase 2. Effector phase 36 37 38 Mechanisms of type IV hypersensitivity Mθ APC TH1 IL2 TNFα IFNγ NO Mθ IL2, TNFα IFNγ preTc Tc 39 Type IV Hypersensitivity perforin Td Cell lymphokines Host Target Cell altered self -antigens MΦ lysosomal enzymes & O2 radicals 40 II. Disease 1. Infectious disease 41 2. Contact dermatitis Contact dermatitis reaction to leather Contact dermatitis reaction to mango sap 42 Tuberculin test Tuberculin test is a screening tool for tuberculosis(TB) . 43 44 1. Ⅰ、Ⅱ、Ⅲ are mediated by antibody. 2.Complement participate Ⅱ、Ⅲ(must depend on complent to cause disease). 3.The same allergen in different individual or in the same individual can cause different type reaction. 4.There may exist two types or more reaction in an individual. 5.One disease can be elicited by different types reactions. Penicillin can induce all four types of hypersensitivity with various clinical manifestations. EXERISE 1.Hypersensitivity. 2.Types of hypersensitivity. 3.The mechanisms of type I,II,III,IV reaction. 4. The treatment of type I hypersensitivity reaction 5. The typical disease of type I,II,III,IV reaction. 47