Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
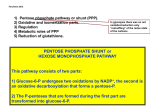
GLUCOSE-6-PHOSPHATE DEHYDROGENASE DEFECEINCY (G6PD) Introduction This anemia is classified as a hereditary hemolytic anemia due to an intrinsic defect (i.e., in the same major group of the spherocytosis). It is similar to HS because: 1- it is hereditary, 2- the defect is intrinsic, and 3- of a hemolytic nature. It differs from HS in the pattern of inheritance where G6PD deficiency is X-linked (HS is autosomal dominant), and, that the cell membrane is compromised by other mechanism (discussed in detail, below). G6PD deficiency along with other anemias such as Pyruvate Kinase deficiency, and Glutathione Reductase deficiency are classified in a group of anemia referred to as “hereditary erythrocyte enzymopathies” (only G6PD is discussed in detail in this course). G6PD deficiency is the most common erythrocyte enzymopathy leading to hemolytic anemia. Anemia results from the inheritance of one of many variant forms of the defective enzyme. The disease is X-linked and therefore all men affected with the disease show its symptoms, where as women can be either affected (homozygotes) or carriers (heterozygotes). G6PD deficiency is very common in West Africa, the Mediterranean, the Middle East, and South East Asia Pathophysiology Glucose-6-phosphate dehydrogenase is one of the most important enzymes in the Pentose Phosphate Pathway (PPP), where it is required for the conversion of Glucose-6-Phosphate (G6P) to 6PhosphoGluconate (6-PG), and for the subsequent production of NADPH and reduced Glutathione (GSH). GSH protects proteins and Hgb from oxidative radicals such as Hydrogen Peroxide, by detoxification and neutralization. RBC’s deficient in G6PD enzyme cannot detoxify hydrogen peroxide (due to low GSH), and subsequently the Hgb gets oxidized to methemoglobin (Hgb with iron in the Fe3+ form). This leads to the release of haem from hemoglobin molecule and the denaturation of the globin molecule forming little inclusions known as the “Heinz bodies”. Heinz bodies attach to the membrane increasing its rigidity, and therefore the cells get trapped and phagocytozed in the splenic microcirculation. Clinical presentation Haemolysis occure in 1-2 days, and it is self limiting. Anaemia takes 7-10 days. Jaundice. The symptoms of G6PD deficiency vary from a patient to another according to the race of the patient, the variation in the enzyme deficiency, and the degree of the oxidative stress. However, most patients experience hemolytic episodes after an exposure to a strong oxidative event, e.g., after taking oxidative drugs, severe infections, diabetic acidosis, etc. For instance, under normal situations patients with the G6PD- variant are not anemic and do not show hemolysis until there is a major stress of oxidative nature, which affects the older RBC’s, mostly. Lab findings 1. CBC (Complete Blood Count) Usually, Hgb is within normal range but falls by 3-5 g/dL suddenly after an oxidative stress. The anemia that develops is usually normocytic normochromic, which gets followed by an increased reticulocytes count 3-5 days after the onset of the hemolytic episode. During the hemolytic episode, peripheral blood smears show non-specific changes including polychromatophilia , increased retic count, poikilocytosis, some spherocytes, and some fragmentation effect (known as the “Bite” cells). Bite cells are the result of the splenic removal of Heinz bodies, and therefore, they are not considered as specific to G6PD deficiency as they can occur in hemoglobinopathies, GSH deficiency, and normal individuals after massive oxidative event. Acute hemolysis in glucose-6-phosphate dehydrogenase (G6PD) deficiency (arrow indicates a “bite” cell, or keratocyte). Chemical assays A number of tests can be useful in aiding the diagnosis of G6PD deficiency. All of which aid to diagnose Qualitative and Quantitative G6PD defects. Acute hemolysis in G6PD deficiency (arrows indicate “blister or bite cells,” and arrowheads irregularly contracted cells). Heinz bodies by supravital stain SICKLE CELL ANAEMIA Sickle cell disease is a group of haemoglobin disorders, in which the there is inherence globin abnormality, caused by substitution of valine for glutamic acid in position 6 in the B chain, that affect the shape and function of the red blood cell Pathology: Hb S is insoluble and forms crystals when exposed to low oxygen tension. Deoxygenated Hb polymerizes into long fibers and the Red Blood Cells (RBCs) form crescent or sickle shape and slow or may block different areas of the microcirculation or large vessels causing infarcts of various organs. Types of sickle cell disease: AS, SS, SC, S/ Thalassemia. When it of the SS type, it called sickle cell anaemia (homozygous condition). Sickle cell anaemia (homozygous condition). Clinical features: Chronic haemolysis, leads to jaundice and anaemia. Vaso-occlusion of blood vessels leads to pain. Infarction and infections. Complications: Begin at 6 months of age Pain in fingers and toes Folate deficiency. Chronic hemolytic anemia jaundiceInfective crises, Bacterial infections (children) Aplastic crises. bone marrow stops making RBCs A vascular necrosis of the head of the femur. Kidney damage, Stone in the gall bladder. Ulcer in the median side of the leg. Laboratory findings: Low Hb. Stained peripheral blood film shows, sickle cells and target cells. Normocytic Normo anemia, Sickle cells, Target Cells, Nucleated RBC/ Polychromasia Features of splenic atrophy (Howell-Jolly body and Pappenheimer), also appears. Reticulocytosis Screening tests for sickiling are positive. Haemoglobin electrophoresis detected the presence of Hb S while no Hb A is detected Hgb F = 1-20%, Hgb A2 = 2-5%. Increased bilirubin Sickle cell trait: This is a benign condition, where there is no anaemia and normal appearance of RBC on the PBF. Haematouria is the most common symptom. Care must be taken with anesthesia, pregnancy and at high altitude. The diagnosis of sickle cell trait is established by an electrophoresis that shows about 55% hemoglobin A and 45% hemoglobin S. Hemoglobin, reticulocyte count and all laboratory tests are normal with sickle cell trait. THALASSAEMIAS Thalassaemias are a heterogeneous group of genetic disorders, which results from a reduced rate of œ (alpha) and ß (beta) chain syntheses, this can result in moderate to severe anemia Basic defect is reduced production of selected globin chains: In alpha thalassaemia, there is no or little alphachain syntheses. In beta thalassaemia, there is no or little beta-chain syntheses. Demographics: Found most frequently in the Mediterranean, Africa, Western and Southeast Asia, India and Burma 1- (alpha)- Thalassaemia syndromes: Greek letter used to designate globin chain: / : Indicates division between genes inherited from both parents: / - Indicates a gene deletion: -/ Classification & Terminology Alpha Thalassemia Normal Silent carrier Minor Hb H disease Barts hydrops fetalis / - / -/- or --/ --/- --/-- 1- Major alpha- thalassaemia or Hydrops fetalis: four genes deletion, leads to complete suppression in the syntheses of alphachain. Alpha chain is important in formation of hemoglobin F in neonate, so in this case the formation of this haemoglobin which is important for fetal life will fail, leading to death in uterus. 2- Three genes deletion: leads to moderate to sever microcytic hypochromic anaemia, with splenomegaly. This is known as Hb H disease. 3- One or two genes deletion: alpha-thalassaemia trait, usually not associated with anaemia. ß- Thalassaemia syndromes: Greek letter used to designate globin chain: + : Indicates diminished, but some production of globin chain by gene: + 0 : Indicates no production of globin chain by gene: 0 ß- Thalassaemia syndromes: Classification & Terminology of Beta Thalassemia Normal / Minor /0 or /+ Intermedia 0/+ Major, very sever. 0/0 or +/+ 1- ß- Thalassaemia major: Sever anaemia (Hb 3-6 g/dl). Enlargement of liver ad spleen. Expansion of bones, leads to Bone deformities. Laboratory findings: Sever microcytic hypochromic anaemia (anisocytosis) Poikilocytosis, normoblast, target and Howell-Jolly bodies. Reticulocytosis. Haemoglobin electrophoresis shows absence of Hb A, Hb A2 is normal. 2- ß- Thalassaemia intermedia: Of moderate severity (Hb 7-10 g/dl). The patient may show bone deformity, enlarged liver and spleen. 3- ß- Thalassaemia trait (minor): This is usually symptom less, and mild anaemia.