Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
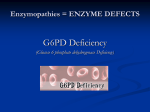
Pharmacogenetics Dr, P Derakhshandeh, PhD Pharmacogenetics genetic variations in drug response • Among normal subject : maximum rate of reaction of drug-metabolizing enzymes often differ widely • drug elimination rates measured in vivo vary by fourfold to more than fortyfold • depending on the drug and population studied • Numerous twin and family studies have shown that genetic factors are mainly responsible for these large interindividual variations. Pharmacogenetics has clinical consequences and biologic significance ? • the inherent capacity to clear a drug may differ among patients • A patient with rapid metabolism may require larger, more frequent doses to achieve therapeutic concentrations • a patient with slow metabolism may need lower, less frequent doses • to avoid toxicity, particularly for drugs with a narrow margin of safety. Many environmental and developmental factors can interact with each other and with genetic factors to affect drug response Genetic, environmental, and developmental factors that can interact, causing variations in drug response among patients. PHARMACOKINETIC VARIATION Acetylation • In about 50% of the U.S. population,drug inactivation • by hepatic N-acetyltransferase • Such persons (slow acetylators) require a longer time to metabolize drugs that are acetylated • therefore they are more susceptible to adverse effects of such drugs (eg, peripheral isoniazid,…) • In the rest of the population, acetylation is rapid • Compared with slow acetylators, such persons require larger or more frequent doses of drugs that are acetylated (eg, isoniazid) • to obtain the desired therapeutic response Oxidation • In about 5 to 10% of whites in North America and Europe • oxidative biotransformation of debrisoquin is decreased • if such persons take debrisoquin for hypertension they are at increased risk of toxicity Aldehyde dehydrogenase-2 • About 50% of Japanese, Chinese, and other Asian populations • lack aldehyde dehydrogenase-2 • an enzyme involved in ethanol metabolism • In such persons, alcohol ingestion results in marked elevations of blood acetaldehyde • in adverse effects (eg, facial flushing, increased heart rate, muscle weakness) Glucose-6-phosphate dehydrogenase (G6PD) deficiency • G6PD is essential for RBC reduction reactions • maintain cytoskeletal integrity. • 10% of black males, are at increased risk of developing hemolytic anemia when given oxidant drugs, such as antimalarials (eg, chloroquine, pamaquine,primaquine), aspirin, and vitamin K. G6PD • it is located at the q28 locus (Pai et al., 1980). • All X-linked genetic conditions, such as G6PD deficiency, are more likely to affect males than females • to have over 400 variant alleles • Different populations have different types of mutations, but within a specific population, common mutations are usually shared. • For example, in Egypt there exists only one type of allele, called the "Mediterranean" variant, demographics of G6PD deficiency • most of the affected individuals reside in Africa, the Middle East, and Southeast Asia. African Americans and some isolated tribes in Africa and Southeast Asia exhibit the highest frequency of incidence for any given population • a defective enzyme can be found in as many as one in four people among these populations (Scriver et al., 1995). CLINICAL ASPECTS OF G6PD DEFICIENCY • red blood cell can no longer transport oxygen effectively throughout the body • hemolytic anemia arises • neonatal jaundice, abdominal and/or back pain, dizziness, headache, dyspnea (irregular breathing), and palpitations (Cecil, 1992) NEONATAL JAUNDICE • Neonatal jaundice is a yellowish discoloration of the whites of the eyes and skin • a direct result of insufficient activity of the G6PD enzyme in the liver • In some cases, the neonatal jaundice is severe enough to cause death or permanent neurologic damage (Beutler, 1994). HEMOLYTIC ANEMIA • An anemic response can be induced in affected individuals by certain oxidative drugs, fava beans, or infections (Beutler, 1994). • Death : if the hemolytic episode is not properly treated Glutathione synthetase deficiency • In patients with RBC glutathione synthetase deficiency (much rarer than G6PD deficiency) • oxidant drugs cause hemolytic anemia • in hepatocytes are at increased risk of liver damage if given such drugs as acetaminophen. Cytochrome P450s • a multigene family of enzymes • in the liver • for the metabolic elimination of most of the drugs currently used in medicine • Individuals that are “poor metabolisers” of the genes encoding specific cytochrome P450s often have mutations which have inactivated the enzyme and severely compromised the ability to metabolize the drug of interest CYP2D6 • One example: the cytochrome P450: CYP2D6 • a highly polymorphic gene that is inactive in about 6% of Caucasians • Many drugs which are used for the treatment of psychiatric, neurological, and cardiovascular disease are metabolized by the product of this gene CYP2D6 • In one variant of the gene • tandem repeat causing individuals to metabolize the substrate so quickly that a therapeutic effect cannot be achieved by conventional doses. CYP2D6 • Also, individuals that are poor metabolisers of CYP2D6 cannot convert codeine to the analgesic morphine and do not achieve the desired effect.