Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
NK1 receptor antagonist wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
NMDA receptor wikipedia , lookup
Drug interaction wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
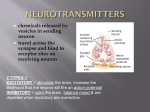
Pre-synaptic receptors Neurotransmitters Post-synaptic receptors -- precursors NT ‘x’ 1. produce 2. pack AP Ca++ inflow 3. release 4. Bind ++ 5. Post-synaptic changes (e.g., epsp) 6.A Recycle 6.B Destroy Pre-synaptic Neuron (axon) synaptic cleft Post-synaptic neuron (dendrite) Pharmacology • A drug can do only two things, either: – Increase the effect of neurotransmitter X (agonist) – Decrease the effect of neurotransmitter X (antagonist) Thus, in order to understand the action of a ‘drug Y’, we need to understand the neurochemical system it interacts with. In other words, we need to understand how Neurotransmitter X - is produced & released from the pre-synaptic neuron - acts on the receptors of the post-synaptic neuron - is removed from the synaptic cleft Specific Neurotransmitter Systems (& drugs that affect them) • Acetylcholine • Monoamines – Dopamine – Noradrenaline & Adrenaline – Serotonin • Amino Acids – Glutamate – GABA • Opioids • • THC Adenosine (caffeine) Receptors for Acetylcholine Cholinergic neurons (release Acetylcholine) Nicotine: Stimulates Nicotinic receptors - Muscarinic - Nicotinic Curare: Blocks nicotinic receptors 1. produce 2. pack 3. release 4. Bind 5. Post-synaptic changes BOTOX Ach-E Atropine: Blocks muscarinic receptors 6.B Destroy Pre-synaptic Neuron (axon) Alzheimer’s treatment Inhibits Ach-E Post-synaptic neuron (dendrite) Belladonna (atropine) curare Acetylcholine (Ach) • Important for: – – – – – Muscle Botox prevents release by terminal buttons (Antagonist) Vigilance Nicotine mimics Ach effect in brain (Agonist) Memory Anti-cholinesterase drugs for Alzheimer’s disease (Agonist) Learning Anticholinergic drugs (to prevent vomit) (Antagonist) Autonomic Nervous System • Cholinergic neurons (release Ach) • Receptors: – Nicotinic (ionotropic): stimulated by nicotine, blocked by curare – Muscarinic (metabotropic): blocked by atropine (belladona) Dopaminergic neurons Receptors for dopamine - D1, D2, D4 (release dopamine) MAO inhibitor L-Dopa Inactive substance Mono-amino Oxidase (MAO) D2 Antipsychotic drugs for schizophrenia Blocks D2 receptors Precursor dopamine pack D2 release Bind Recycle Pre-synaptic Neuron (axon) Cocaine, amphetamine, Methylphenidate (ritalin) Makes dopamine transporter work in reverse Post-synaptic changes D1 Post-synaptic neuron (dendrite) Dopamine (DA) • Important in: – Movement control – Drug addiction – Schizophrenia (?) – ADHD death of dopaminergic cells in Parkinson’s disease amphetamine, cocaine (agonist) anti-psychotic drugs (antagonists) metylphenidate (ritalin) • dopaminergic neurons (release DA) – Substantia nigra: – Ventral Tegmental Area (VTA): – VTA to frontal cortex • • movement control drug addiction schizophrenia (?) Receptors: D1, D2, D4 Group Activity: – Would PD treatment with L-dopa increase or decrease hallucinations? (one of the symptoms of schizophrenia) – Would antipsychotic drugs produce PD like symptoms as a side effect (e.g., motor problems)? Why? Why not? – Schizophrenic patients often fail to take their medication, despite the benefitial effects. Can you provide a physiological explanation? (hint: which systems does the drug block?) Dopamine The Reward System: Dopamine Activities of survival (sex, feed) activate the reward system Drugs of abuse similarly activate the reward system Electrical stimulation of the reward system is also addictive Dopamine release in the nucleus accumbens during Intracranial self stimulation - during sexual behavior - in anticipation of sex -during ingestion of a preferred food - to a cue associated with food (CS) -during IV cocaine self-administration -to a cue associated with cocaine (CS) Cocaine and Amphetamine: administration & distribution Administration: intranasal intravenous smoke (‘crack’) Distribution: ‘Crack’: is more liposoluble, thus stronger effect! Cocaine has a very short half life (40 mins) Overview- neurotransmitters • Acetylcholine • Dopamine • • • • • • Adrenaline Serotonine Glutamate GABA Opioids THC (cannabis) Noradrenaline & Adrenaline • Aka: norepinephrine & epinephrine • Important for: – Vigilance (adrenaline response) • Noradrenaline acts as a neurotransmitter • Adrenaline acts also as a hormone • Receptors: – Alpha – Beta: beta-blockers are used for hypertension Oh no! my sympathetic nervous system is overactive again! Serotonin (5-HT) • Important in: – Depression • Receptors: – Way too many! • Drugs: – Fluoxetine (prozac): inhibitor of reuptake (recycle) (SSRI) – LSD: agonist of 5-HT2A – Ectasy: agonist for serotonin and agonist for noradrenaline Glutamate • Is the most pervasive excitatory NT in the brain • Receptors: – Four types (remember NMDA): • Important in: – Learning (NMDA receptor in the hippocampus) • Drugs: – Alcohol: NMDA antagonist • Sleepy, impaired cognitive performance • Alcohol withdrawal seizures GABA • Is the most pervasive inhibitory NT in the brain • Receptors: – GABAa: opens Cl- channel – GABAb: opens K+ – Question: does it puzzle you that, being GABA an inhibitory NT, GABAa and GABAb receptors open channels of different polarity? Justify • Drugs: – Benzodiazepines (valium): GABA Agonist • For reducing anxiety, promoting sleep, anti-convulsant, muscle relaxant – Alcohol: GABA agonist • Anxiolytic • Don’t drink while taking this medication • Alcohol withdrawal seizures Alcohol • Alcohol acts on many systems: – Blocks NMDA: that is why memory is impaired, and why alcohol withdrawal can trigger seizures – GABA: That is why at low levels alcohol has an anxiolytic effect, and at higher levels sedative effect – Dopamine (mesolimbic system): increases release of DA in nucleus accumbens, thus the euphoria, addictive power of alcohol Opiates: – Endogenous opiates: secreted in response to survival behaviors • analgesia • positive reinforcement (encourages the survival behavior) – Exogenous opiates; • Morphine (opium) • Codeine (opium) • Heroin (semisynthetic) •1897 – Mail order advertisement from Sears, Roebuck & Co. for opium-based drink •Early 20th century – mothers encouraged to use opium syrup to soothe teething pain • •Narcotic comes from the Greek word, “narke”, meaning stupor and referred to any drug that induced sleep Opiates: administration & distribution Administration: smoke (Opium, Heroin) intranasal (heroin) intravenous (Heroin) oral, not very good to get high (Codeine, morphine, methadone) Distribution: Heroin is 10 times more liposoluble than morphine, so it reaches brain faster and at larger concentrations, and get transformed into morphine Opioids morphine • Drug Effects: – Analgesia (morphine) – Activates Reward system (addictive power) – Inhibits defensive response (e.g., hiding) • Antagonist: – Naloxone: • Use in the acute treatment of heroin overdose • Blocks analgesic effect of placebo Naloxone Opiates: Side effects Most of the risks are secondary to the status as illegal. – Legal: Jail – Health: HIV, hepatitis C, overdose – Financial: loss of employment, cost of drugs – Few direct problems from chronic use (surprisingly) • (constipation, bladder cancer, pregnancy) Cannabis: • THC is the active ingredient in marijuana. • THC receptor: CB1 – large concentration in hippocampus (memory effect) • THC stimulates release of dopamine in the nucleus accumbens and the ventral tegmental area – Long-term damage: • Cognitive impairments from long-term use appear to be subtle. Cannabinoids (THC) • There are endogenous & exogenous cannabinoids (marijuana) • They are lipids: – They mix well in butter (cookies) & oil (pesto), but not in alcohol or water. – They depot in fat tissue: thus metabolites can be detected in urine long after the psychoactive effect • Drug Effects: – Analgesia – Sedation – Stimulates eating (munchies) – Reduces concentration & memory – Distorts time perception •