Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychophysics wikipedia , lookup
Development of the nervous system wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuroregeneration wikipedia , lookup
Synaptogenesis wikipedia , lookup
Neural engineering wikipedia , lookup
End-plate potential wikipedia , lookup
Electromyography wikipedia , lookup
Central pattern generator wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
Proprioception wikipedia , lookup
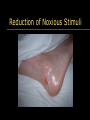
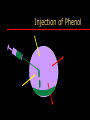
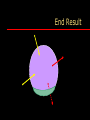
Improving life and end-of-life care in advanced neurological conditions: Spasticity Management Rory O’Connor MD Consultant Physician in Rehabilitation Medicine Airedale General Hospital Overview What is spasticity? Epidemiology Current spasticity treatment Pharmacotherapy What is Spasticity? Spasticity Diagnosis Central nervous system lesion – Motor and sensory loss Increased muscle tone – Especially rate dependent increase in tone Provoked or unprovoked spasms Consequences of Spasticity Contractures Skin breakdown Pain and discomfort Impairments Restricted participation Caregiver strain Spasticity What is Spasticity? Supraspinal Input Supraspinal or higher spinal lesion results in a net loss of inhibition below lesion – Dorsal Reticulospinal tract ( - ) – Medial Reticulospinal tract (+) – Corticospinal tract (+) – Vestibulospinal tract (+) – Coerulospinal tract (+) Spinal Input 1. Reflex disinhibition – Nociceptive reflex: flexor withdrawal – Propriospinal phasic reflex: tendon reflex 2. Primitive reflex release – Cutaneous: extensor plantar response – Proprioceptive: positive support reaction 3. Tonic stretch reflex Tonic Stretch Reflex No reflex activity in response to muscle stretch in a relaxed normal person Mediated via 1a afferents from muscle spindle Length dependent – Reflex inversely related to muscle length Loss of Supraspinal Input Uncontrolled efferent drive – Hemiplegic posture Associated reaction – Failure to inhibit spread of motor activity Disordered muscle control – Co-contraction Neurotransmitters Gamma amino butyric acid (GABA) – Inhibition of motor neurons Glutamate – Excitation of motor neurons Alpha-2 adrenergic – Spinal interneuron inhibition Soft Tissues in Spasticity Muscle biochemical changes: thixotropy – – – – Stiffness Contracture Fibrosis Atrophy Tendon changes Joint changes What is Spasticity? An increased tonic stretch reflex resulting in velocity- and length-dependent hypertonia due to abnormal spinal processing of proprioceptive input Epidemiology of Spasticity Epidemiology of Spasticity Spinal – Traumatic spinal cord injury – Non-traumatic spinal cord injury 60% Supraspinal – Stroke – Multiple Sclerosis – Cerebral Palsy – Traumatic Brain Injury 20% 30% 50% 19%* Current Spasticity Treatment Current Spasticity Treatment Reduction of noxious stimuli Multidisciplinary programme Pharmacotherapy – Generalised, regional, focal Surgery Spasticity Treatment Cost may inhibit decision to treat – Time-consuming and multidisciplinary – Expensive equipment and seating systems But untreated spasticity – May mask voluntary movement – Result in permanent contractures – Window of opportunity may be small Reduction of Noxious Stimuli Reduction of Noxious Stimuli Reduction of Noxious Stimuli Reduction of Noxious Stimuli Reduction of Noxious Stimuli Reduction of Noxious Stimuli Multidisciplinary Teamwork Careful positioning throughout 24-hours – Maintaining muscle length – Reducing deformity Regular stretching Splinting and orthoses All act to reduce the tonic stretch reflex Seating Pharmacotherapy Pharmacotherapy Follow-up No point in pharmacotherapy without – Avoidance of precipitating factors – Adequate therapy/splinting/orthosis – Appropriate seating review Pharmacotherapy Generalised – Oral baclofen, dantrolene, tizanidine Regional – Intrathecal baclofen or phenol Focal – Intramuscular botulinum, phenol neurolysis Generalised Generalised Reduce excitatory neurotransmitters – Tizanidine Facilitate inhibitory neurotransmitters – Baclofen Inhibit skeletal muscle contraction – Dantrolene Regional Intrathecal Baclofen Test dose to screen for effectiveness Non-destructive and reversible Dose titratable Reduction of side effects compared to oral baclofen – 1% of oral dose Intrathecal Pump Abdominal pocket for pump Intrathecal catheter tunnelled subcutaneously Intrathecal Phenol Severe lower limb spasticity affecting care, positioning or causing pain Generalised treatments ineffective or causing side effects Other regional and focal treatments inappropriate Bowel, bladder and sexual dysfunction Modified Right Lateral Position 30o Spinal fluid Modified Right Lateral Position Injection of Phenol Injection of Phenol Spinal fluid Injection of Phenol End Result Spinal fluid Unexpected Findings Final Outcome Focal Phenol Nerve Blocks Non-selective denervation – Protein denaturation – Destruction of nerve axons Effect apparent immediately and diminishes with time Injection of mixed nerves will cause anaesthesia as well as paralysis Commonly Blocked Nerves Musculocutaneous – Biceps brachii, brachialis Obturator – Hip adductors Sciatic – Hamstrings Posterior tibial – Gastrocnemius, soleus Botulinum Botulinum exotoxin – Types A and B available commercially Intramuscular injection – Endocytosed in pre-synaptic neuron – Cleaves acetylcholine – Neuromuscular junction function inhibited Axon sprouting terminates effect 2-6 months EMG Guidance Botulinum - FDS Botulinum - FDP Botulinum - Hypersalivation Botulinum - Hypersalivation Take Home Message I Spasticity limits activities in two ways – Inhibiting muscle power and coordination – “Masking” profound muscle weakness But anti-spasticity agents produce muscle weakness Take Home Message II Spasticity is the result of – Neural – Non-neural } abnormalities Take Home Message III Multidisciplinary treatment must comprise – Neural – Non-neural } modalities