Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Surround optical-fiber immunoassay wikipedia , lookup
Adaptive immune system wikipedia , lookup
DNA vaccination wikipedia , lookup
Molecular mimicry wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Duffy antigen system wikipedia , lookup
Autoimmune encephalitis wikipedia , lookup
Carbapenem-resistant enterobacteriaceae wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Immunocontraception wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Anti-nuclear antibody wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
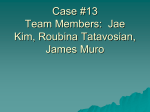
International Journal of Chemical Engineering and Applications, Vol. 2, No. 2, April 2011 Identification of Klebsiella Pneumoniae by Capsular Polysaccharide Polyclonal Antibodies A. S. Sikarwar and H. V. Batra Abstract— The aim of this study is to develop simple and rapid diagnostic method which can be utilized routinely for detection of Klebsiella pneumoniae. This study was done in India at DRDE, Gwalior. We have collected standard K.pneumoniae strain 3296 from Yamaguchi University, Japan and total fifty-nine clinical isolates of Klebsiella species from Armed Force Medical College, Pune, and Patel chest hospital, New Delhi. Bacteria were grown on trypticase soy broth and two Newzealand wistar white rabbit were immunized subcutaneously with purified capsular polysaccharide (CPS) of K.pneumoniae. Specificity of hyper immune sera raised against CPS was tested by counter current immunoelectrophoresis. We have generated four monoclonal antibodies, out of which two IgM producing clones (KP-1 & KP-2) and hyper immune sera against CPS antigen were used for agglutination test. KP-1, KP-2 and CPS hyperimmune sera showed different reactions. Out of the twenty biochemically confirmed K.pneumoniae clinical isolates, hyperimmune sera to CPS detected sixteen as positive whereas KP-1 reacted to eleven and KP-2 to thirteen of these isolates. One clinical Klebsiella species biochemically negative for K.pneumoniae and other Enterobacteriaceae organisms were negative by agglutination test to all the three antibody reagents. K.aerogenes, however, reacted to KP-2 and CPS hyperimmune sera. Standard K.pneumoniae was positive to all the three antibodies. The rapidity and ease of performance merited the hyper immune sera to CPS and IgM monoclonal antibody based agglutination test as the preliminary identification system for K.pneumoniae. Index Terms— Capsular Polysaccharide, diagnostic method, Klebsiella pneumoniae, polyclonal antibodies. I. INTRODUCTION Klebsiella is an important opportunistic pathogen, which was reported worldwide. It can causes infections of respiratory tract, nasal mucosa, pharynx and generally results in primary pneumonia. Pneumonia is the most frequent nosocomial infection (30 to 33% of cases) among combined medical-surgical intensive care units participating in the National Nosocomial Infections Surveillance System [1]. Klebsiella species were found to be the most frequently isolated gram negative bacteria in cases of primary bacteremia [2]. It is the second pathogen, next to E. coli that causes urinary tract infection. It normally affects persons Manuscript received Febraury,10, 2011. This work was supported by the Graduate Aptitude Test in Engineering scholarship, from behalf of Department of higher education, Ministry of Human Resources Development, Government of India. A.S. Sikarwar working with the International Medical University, No:126, Jalan Jalil Perkasa 19, Bukit Jalil, 57000, Kuala Lumpur, Malaysia (Phone: +60 3 2731 7274, Fax: +60 3 8656 7229, e-mail: [email protected]). Harsh Vardhan Batra working with Defence Research Development organisation, India . with low immune system such as hospital patients, diabetes patients and people with chronic lung disease. Many a times, alcoholics also suffer from K. pneumoniae infections. Thus, the infections are either hospital-acquired or community-acquired. Klebsiella pneumoniae is a facultative anaerobic, nonmotile, rod-shaped, gram-negative bacteria with a prominent polysaccharide capsule. This capsule encases the entire cell surface, accounts for the large appearance of the organism on gram stain, and provides resistance against many host defense mechanisms. Members of the Klebsiella genus typically express 2 types of antigens on their cell surface. The first is a lipopolysaccharide (O antigen); the other is a capsular polysaccharide (K antigen). Both of these antigens contribute to pathogenicity. About seventy-seven ‘K’ antigens and nine ‘O’ antigens exist. The structural variability of these antigens form the basis for classification into various serotypes. The virulence of all serotypes appears to be similar. Capsule plays a very important role in virulence so we have started our study with the aim to utilize capsular polysaccharide as an antigen to develop simple and rapid diagnostic method which can be utilized anywhere without the use of any sophisticated equipments specially for field use as a preliminary routine test for detection of Klebsiella pneumoniae. The diagnosis of Klebsiella infection is made on the basis of clinical examination, isolation and identification of the organism. Laboratory identification is usually carried out by cultures, gram staining and a battery of biochemical tests. Bacterial isolation takes 24 hours and biochemical tests have their own limitations in that the results may be available only after 48 hours. Even then accurate identification at species level of the genus may not be possible in all cases. In clinical situations, the severity of infections does not warrant such a long period of investigation for an appropriate treatment to be started. Speed of diagnosis, therefore, is essential in the management of serious patients. Hence, the need arises for reliable and quick serological methods for rapid diagnosis of Klebsiella infections. Several serological assays for detection of antibody and antigen have been developed and these include capsular swelling reaction, ELISA and so on. The problems with most of the reported antibody and antigen detection assays so far have been the low reproducibility, sensitivity and specificity with high cost. The reason being ,most of the antigenic moieties and polyclonal antibodies used are common to many related and unrelated bacterial species. As a result most of these assays have exhibited low potential in endemic areas due to ubiquitous nature of Klebsiella and 130 International Journal of Chemical Engineering and Applications, Vol. 2, No. 2, April 2011 shows extensive cross reactions among themselves. Since there is a need to develop more sensitive and specific assay with monoclonal antibodies and capsular polysaccharide antisera. With this aspect in view, the present study was initiated with the following aims and objectives: 1) To purify capsular polysaccharide antigen of K.pneumoniae and develop hyper immune sera against it. 2) To develop rapid and simple antigen detection immunoassay with capsular polysaccharide antisera for the diagnosis of K. pneumoniae. 3) To compare the effectiveness of monoclonal and capsular polysaccharide polyclonal antibodies against K.pneumoniae by using agglutination method for rapid detection of organism. II. MATERIAL AND MEHODS We have collected standard and clinical isolates of K.pneumoniae from different places and utilized them for the generation of monoclonal and polyclonal (CPS) antibodies. We utilized them for our study. A. Animals New Zealand male white rabbits weighing 1 to 1.2 kg, were obtained from animal house of Defence Research Development Establishment, (DRDE) Gwalior, India. B. Bacterial Strains 1) Standard cultures: K.pneumoniae strain 3296 was gifted by Dr Uchiyama, Yamaguchi University, Japan. Two K.pneumoniae serotypes, 01K1 & O1K2 were kindly provided by Dr Philip Domenico, Winthrop University Hospital, New York. Another standard strain of K.pneumoniae K-2 was obtained from Dr S.S. Thukral from Patel Chest Hospital, New Delhi, India. 2) Clinical isolates: Fifty - four clinical isolates of Klebsiella species recovered from pus, urine and sputum samples were collected from Armed Force Medical College, Pune, India. Four Klebsiella clinical isolates from pneumonic patients and one from urinary tract infection were obtained from Patel Chest Hospital, New Delhi, India. 3) Other bacteria: K. aerogenes, E. aerogenes, C. koseri, E. cloacae, Y. enterocolitica, Y. pseudotuberculosis were obtained from microbiology division of DRDE, Gwalior, India. C. Preparation of Whole Cell Lysate Young cultures of K.pneumoniae were harvestedand washed thrice, with sterile Phosphate Buffer Saline (0.01 M, pH 7.2).The pellet was suspended in sterile distilled water and centrifuged at 10,000 Xg for 15 minutes at 5oC in a Sorvall RC5C centrifuge. Bacterial suspensions were sonicated at 5 watts output for 15 cycles of one minute each with one minute rest in sonicator (Microson)using a titanium probe while the sonication vessel was kept covered in ice. The sonicated material was centrifuged at 10000 Xg for 30 minutes at 5oC.The supernatant was filter sterilized using 0.45 um pore size filter and antiproteolytic agents pepstatin (10-7 M), leupeptin (10-6 M), and phenyl methyl sulfonyl fluoride (2mM) were added. Thimersol at 0.01 percent was added as preservative. The protein contents of the antigens were estimated by Lowry’s method [3]. D. Purification of Capsular Polysaccharide Bacteria were grown on trypticase soy broth at 370C with shaking at 100 rpm in a shaker incubator for 16 hours. Organisms were harvested by centrifugation at 10,000 Xg for 30 minutes. Cetavlon, was added to a final concentration of 0.5 %. After stirring for 30 minutes at room temperature, the precipitate was collected by centrifugation. The material was dissolved in 1M CaCl2 solution and 25% ethanol was added to it in equal amount. After stirring for 60 minutes at room temperature, the precipitated nucleic acid were removed by centrifugation at 10,000 X g for 30 minutes. The CPS was precipitated from the resultant supernatant by addition of equal volume of 80% ethanol. The CPS was dissolved in distilled water and extracted three times with an equal volume of chloroform butanol solution (5:1). The pooled water phases were extensively dialyzed against distilled water at 40C and then vacuum concentrated. Finally the solution was centrifuged at 100,000 X g for 16 hours for the removal of lipopolyssacharide. The resulting pellet was discarded and supernatant containing CPS was collected. CPS was purified [4] followed with sugar estimation test [5]. E. Immunization with Capsular Polysaccharide Antigen Rabbits were immunized with 800 ug / dose of purified CPS of K.pneumoniae. Antigen was given subcutaneously with complete Frend’s adjuvant. Five doses of same amount of antigen were given at seven days interval each with incomplete Frend’s adjuvant. Antibody titer and specificity of hyperimmune sera against purified capsular polysaccharide antigen was checked by counter current immunoelectrophoresis . F. Generation of Monoclonal Antibodies Balb/c mice were immunized subcutaneously with 50 ug of sonicated antigen of K.pneumoniae with complete adjuvant followed by 3 booster injections containing similar antigen dose mixed in incomplete adjuvant given intraperitoneally at the interval of one week each. The mouse with high serum antibody titre was sacrificed by cervical dislocation. The spleen was removed aseptically and cell suspension was prepared after centrifugation at 1500 rpm at 4oC for 5 minutes with Dulbecco’s Minimal Essential Medium. Mouse myeloma cell line SP2/0 was used for fusion. Kohler and Milstein method was used for fusion with minor modification [6]. Clones were screened under inverted microscope for hybrids. Cloning was done by limiting dilution procedure followed by freezing and thawing of cells. G. Identification of Klebsiella Species 1) Morphological characterization: All the clinical isolates were examined morphologically for colony characterization on nutrient agar , Brain Heart Infusion as well as on MacConkey agar and incubated for 24 hours at 37oC followed by Gram’s staining. Bacterial suspension were made in normal saline for Gram’s 131 International Journal of Chemical Engineering and Applications, Vol. 2, No. 2, April 2011 staining. Smear was prepared on a glass slide followed by air dried and fixed by gentle heating. The slide was flooded with crystal violet for 1 minute. The stain was washed off with excess of tap water. Gram’s iodine was poured over the slide for 1 minute. The slide was washed and destained with ethyl alcohol. Finally, counter staining was done with safranin for 30 seconds. It was rewashed, dried and observed under the microscope. 2) Biochemical characterization: Clinical isolates those exhibiting mucoid colonies were processed for biochemical testing. Biochemical tests employed were urease production, citrate utilization and fermentation of sugars. Eight sugar fermentation tests were performed including sucrose, glucose, mannitol, lactose, adonitol, dulcitol, melibiose and esculin. Indole test and H2S production on TSI agar, oxidase, catalase and nitrate tests were also carried out. Beside these tests, motility and growth of organism in KCN were also checked. For biochemical tests standard procedures were used [7]. 3) Sodium Dodecyl Sulphate- PolyAcrylamide Gel Electrophoresis (SDS-PAGE) : Protein profile of biochemically confirmed positive clinical isolates of K.pneumoniae were observed by SDS-PAGE, which was carried out as per the procedure of Laemmli with minor modifications [8]. H. Agglutination Bacterial suspension of all clinical isolates of K.pneumoniae along with negative and positive control were made in glycine saline buffer and a homogeneous suspension was prepared. Equal volume of bacterial suspension and antibodies (monoclonal and CPS polyclonal) were added on glass slides separately. They were mixed properly with stick and observed for agglutination reaction within five minutes. III. RESULT AND DISCUSSION Capsular polysaccharide antigen was subjected to sugar and protein estimations. Purified CPS antigen preparation had sugar concentration of 0.27 mg/ml and protein concentration of 0.06mg/ml. Titre of rabbit hyperimmune sera to purified capsular polysaccharide antigen was checked by counter current immune electrophoresis. Purified capsular polysaccharide antigen was titrated against two fold dilution of CPS antisera against CPS antigen. Highest sera dilution at which single precipitin band could be observed was 1:4. There was no band seen with PBS blank. The specificity of CPS antisera was tested by counter current immunoelectrophoresis and Western blot. Result of CIE is shown in fig A. In Western blot CPS antisera showed specific reactions with K.peumoniae while there was no reaction seen with E.coli, S.typhi, Y.pseudotuberculosis, Y.enterocolitica and P.vulgaris. The standards and clinical isolates of Klebsiella species showed morphological characteristic bacterial colonies on BHI and nutrient agar exhibiting mucoid colonies of viscid consistency on these agars. Capsule production was seen by cultivating the organism on bromo thymol blue lactose agar. All the four standard K.pneumoniae (3296, 01K1, 01K2 and K2) strains produced navy blue colored colonies indicating capsule production. Fig 1: Specificity of hyperimmune sera to capsular polysaccharide by counter current immunoelectrophoresis. B= Blank, 1=K.pneumoniae, 2= E.coli, 3= S.typhi, 4= Y.pestis, 5= Y.enterocolitica The biochemical characterization of standards and clinical isolates of Klebsiella were examined by battery of biochemical tests. Standard K.pneumoniae cultures showed positive reaction for urease production, citrate utilization, catalase reaction and fermentation of sugar like glucose, lactose sucrose, mannitol, adonitol, melibiose and esculin. Organism showed negative test for indole production.There was no H2S production on Triple Sugar Iron agar but growth of organism was seen in KCN. All fifty-nine clinical isolates exhibiting colonies similar to Klebsiella species were tested biochemically. Thirty – six clinical isolates showed typical common biochemical reaction pattern similar to the one seen with Klebsiella species, being positive to glucose, lactose, sucrose, mannitol and negative to oxidase and indole. When tested by second battery of biochemical reactions that included some rare sugars (adonitol, melibiose, esculin and dulcitol), twenty of them exhibited reactions attributable to majority of K.pneumoniae sub species pneumoniae strains, being positive to adonitol, melibiose, esculin, urease, and citrate. They also showed growth in KCN.The rest of the isolates had variable reactions with these tests. The biochemical reactions of all fifty-nine samples are presented in Table I-a,b,c and d respectively. 132 TABLE I-A: BIOCHEMICAL CHARACTERIZATION OF CLINICAL ISOLATES OF KLEBSIELLA SPECIES. International Journal of Chemical Engineering and Applications, Vol. 2, No. 2, April 2011 on Sodium Dodecyl Sulphate – Polyacrylamide Gel Electrophoresis (SDS-PAGE).On SDS-PAGE approximately 25 to 30 bands could be obsereved with Klebsiella and other Enterobacteriaceae organism tested. The protein banding pattern of different organisms were studied. The unique pattern of Klebsiella could be easily identified from the others. The protein bands at 82 kDa area were prominently displayed in Klebsiella. Result of SDS-PAGE of selected biochemically positive clinical isolates is shown in fig B. TABLE I-B: CONTINUE TABLE I-C: CONTINUE Fig B: Protein profile of selected biochemically confirmed Klebsiella species from different clinical samples by SDS-PAGE. TABLE I-D: CONTINUE Lane 1= 17, Lane 2=18, Lane 3=21, Lane 4= 24, Lane 5=25, Lane 6= 26, Lane 7= 27, Lane 8= 28, Lane 9= 29, and Lane 10= 30. Besides biochemical testing of clinical isolates, we have also generated and collected monoclonal and polyclonal (CPS) antibodies which were used for rapid detection of K.pneumoniae by agglutination test. Following fusion of sensitized spleen cells with myloma cell line, a total of 137 wells contained hybrid clones. When tested by Enzyme Linked Immuno Sorbent Assay (ELISA) for anti – K.pneumoniae antibodies, out of 137 wells culture supernatant from 50 wells showed reactivity. After subsequent limiting dilutions, we were finally able to stabilized and preserved only 4 clones. Using rabbit anti-mouse immunoglobulin heavy chain antisera in plate ELISA, the 4 clones were tested for their isotypes. Two clones (KP-1 and KP-2) were with u chain type and 2 (KP-3 and KP-4) were of gamma chain type. Besides CPS antisera, we were also utilized KP-1 and KP-2 monoclonal antibodies to compare the effectiveness of type of antibodies for detection of K.pneumoniae by agglutination method. KP-1, KP-2 and CPS antibodies showed different reactions against K. pneumoniae. Out of fifty - nine clinical isolates morphologically resembling Klebsiella, twenty clinical isolates were found positive for K. pneumoniae at biochemical and SDS-PAGE characterization. Out of these clinical isolates, hyper immune sera to CPS detected 76% samples as positive and unable to react 24% samples of K. pneumoniae whereas KP1 reacted to 52% clinical isolates and showed no reaction to 48% samples. KP2 detected 62% of these isolates as positive and 38% were detected as negative samples. We have utilized K. aerogenes , E. aerogenes , C. koseri , E. cloacae ,Y. enterocolitica, Y. pseudotuberculosis as negative control and found that KP1 is highly specific with low sensitivity as it does not showed any cross-reactivity for negative controls but Biochemically identified K.pneumoniae organisms showed identical banding pattern to standard K.pneumoniae 133 International Journal of Chemical Engineering and Applications, Vol. 2, No. 2, April 2011 sensitivity of this clone is only 52% however, KP2 and CPS antisera showed cross - reactivity against K.aerogenes but not against any other negative control. CPS antisera showed the highest sensitivity out of these three antibodies as it has detected sixteen as positive and five as negative. Standard K.pneumoniae was positive to all the three antibodies. The details of data is shown in fig C. can possibly replace the time and resources consuming conventional biochemical identification in routine bacteriological laboratories. The test can also be utilized in peripheral disease surveillance / clinical laboratories for rapid identification of K. pneumoniae. Direct detection of antigens from clinical samples needs to be explored with the specific antibodies as reported here. For future research, we can generate monoclonal antibodies against purified CPS antibodies and utilized that for simple and more reliable preliminary testing purposes, especially in fields for soldiers and villagers where they don’t have advanced equipment for testing. KP1 ACKNOWLEDGEMENT KP2 CPS A.S. Sikarwar would like to thank to Ministry of Human Resources for providing GATE fellowship to complete this research . Author would also like to thank, Director of Defence Research Development Establishment Gwalior, India for his kind support during research. A.S. Sikarwar would also be thankful to Dr J.Uchiyama (Yamaguchi University, Japan), Dr Philip Domenico (Winthrop University Hospital, NewYork), Dr S. S. Thukral ( Patel Chest Hospital, India ) and Armed Force Medical College, Pune, India for providing us standard and clinical samples of K.pneumoniae for our studies. Fig. 2: Comparative analysis of newly developed detection system for specificity and sensitivity of monoclonal KP1, KP2 and CPS polyclonal antibodies against K.pneumoniae 16 14 REFERENCES 12 10 [1] 8 6 Series1 4 [2] 2 0 KP1(-) KP1(+) KP2 (-) KP2 (+) S1 CPS (-) CPS (+) [3] Fig 3 : Detection of K.pneumoniae clinical isolates by agglutination test. [4] IV. CONCLUSION [5] IgM producing clones KP1, KP2 and CPS antibodies were utilized for the agglutination test system. Out of these three antibodies, we found that CPS antibodies showed the highest sensitivity 76% for clinical isolates as shown in fig D. The rapidity and ease of performance merited the HIS to CPS polyclonal antibody based agglutination tests as the preliminary identification systems for K.pneumoniae.This newly developed CPS polyclonal antibody based agglutination test is simple and quick, which [6] [7] [8] 134 M.J., Richards, J. R. Edwards, D. H. Culver, R. P. Gaynes and the National Nosocomial Infections Surveillance System. “Nosocomial infections in combined medical-surgical intensive care units in the United States” Infect. Control Hosp. Epidemiol. 21: 2000, pp. 510-515 A. Cross, J.R. Allen, J. Burke, G. Ducel, A. Harries, J. John, D. Johnson, M.Lew, B.McMillan, P.Meers, R.Skalova, R. Wenzel and J. Tenney. “Nosocomial infections due to Pseudomonas aeroginosa”. Review of recent trends. Rev. Infect. Dis. 5 (Suppl.) 1983,pp. 837 – 845. O.H. Lowry, N.J. Rose brough, A.L. Fan and R.J. Randall. “Proein measurement with the folin-phenol reagent”.J. Biol. Chem., 193. 1951, pp.265-275. S.J.Cryz Jr, E. Furrer and R. Germanier. “Purification and vaccine potential of Klebsiella capsular polysaccharides. Infect.Immun. 50 (1), 1985a , pp. 225-230. M. Dubois, K. A. Giles, J. K. Hamilton, P. A. and F. Smith “Colorimetric method for determination of sugars and related substances”, Anal. Chem. 28 (3) , 1956 ,pp. 350 - 356. G. Kohler and C. Milstein. “ Continuous cultures of fused cells secreting antibody of predefined specificity. Nature. 256, 1975, pp.495-497. R. Cruickshankk, “Medical Microbiology” 12th eds. (revised reprint) Edinburg : Churchill Livingstone. 1980, 170 – 189. U.K. Laemmli,U.K. “ Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature (London), 227, 1970, pp.680-685.