Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Stimulus (physiology) wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Feature detection (nervous system) wikipedia , lookup
Proprioception wikipedia , lookup
Central pattern generator wikipedia , lookup
Development of the nervous system wikipedia , lookup
Sensory substitution wikipedia , lookup
Neural engineering wikipedia , lookup
Embodied language processing wikipedia , lookup
Premovement neuronal activity wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Evoked potential wikipedia , lookup
Neuroregeneration wikipedia , lookup
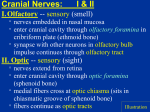
The Crash Course in Head, Neck, and Arm By Mike Sughrue This is not intended to be a primary text (if it was it would not have as many spelling and grammar errors as it does) nor does it cover every single topic that is on the test. Instead it focuses on the areas of confusion that lend themselves to simple ways to reorganize the information so that it is easy to retain and understand. Head and Neck Every branch of every Cranial nerve Learning the organization of the cranial nerves (including nuclei, ganglia, functions, lesions etc) can be a daunting task, however this can be greatly simplified with the use of the following tools (assuming that one has at least a minor degree of familiarity with the nerves) 1) Knowledge of the motor/sensory status of the nerves 2) My concept of “Modality” 3) The concept of Pre/post trematic branches (with my modifications) 4) The embryology of the Pharyngeal arch cartilages 5) Very minor knowledge regarding patterns of evolution in the CNS 6) Knowledge of the branching pattern of the Maxillary artery 7) One mnemonic 8) A brief understanding of the ways in which the III violates my rules #1-The 12 Nerves and their Motor/Sensory status First a listing of the nerves along classical lines, that will then be followed by a reclassification 1) Olfactory=Sensory 7) Facial=Mixed 2) Optic=Sensory 8) Vestibulocochlear=Sensory 3) Oculomotor=Motor 9) Glossopharyngeal=Mixed 4) Trochlear=Motor 10) Vagus=Mixed 5) Trigeminal=Mixed 11) Accessory=Motor 6) Abducens=Motor 12) Hypoglossal=Motor To reclassify along more functional lines Sensory- Olfactory (1), Optic (2), Vestibulocochlear (8) Motor- Oculomotor (3), Trochlear (4), Abducens (6), Accessory (11), Hypoglossal (12) Mixed- Trigeminal (5), Facial (7), Glossopharyngeal (9), Vagus (10) If we know just this, we can predict alot of things about these nerves. The nerves in the sensory group typically run directly to their target organ, and their complexity primarily becomes manifest in the CNS. Thus they are not the targets for this discussion. The motor and mixed group classification allows us to further elaborate on the key to understanding the cranial organization, the embryology of the area (I hear the groans). Nerves that are purely motor innervate structures from the somites and tend to be rather simple in their patterns. They have one nucleus in the medial column of the brain stem (the 3 as we will see is the exception), and that somatic motor nucleus is always named after the nerve. The Mixed nerves (5,7,9,10) are the pharyngeal arch nerves, their somatic motor nuclei are found in the lateral brainstem column, and because they tend to have multiple modalities, they have numerous associated ganglia, tracts, and nuclei. These nerves also follow the pre/post trematic rules. #2- My concept of Modality A peripheral nerve by definition can only carry 4 types of neurons: Somatic motor, Somatic sensation (touch, pain, and proprioception), Autonomic (for these nerves primarily parasympathetic) motor, and Visceral sensation (gut afferents and taste). Most motor only cranial nerves in this discussion (i.e. 4,6,11,12) have one modality (Somatic sensation). The III defies this by containing 2 modalities (Somatic and Parasymp. Motor). The mixed nerves are typically the source of worry with regards to serving multiple functions. Thus a listing of these is in order. Trigeminal-2 (Somatic sensory and Somatic motor) Facial-3 (4 depending on source, Netter has facial w/o somatic sensation, April has it included in the VII) Glossopharyngeal-4 Vagus-4 (the number of modalities increases with increasing CN number until it maxes out at 4) The reason for discussing this is because it allows us to understand the brainstem organization, the ganglia that lie near the nerve origin (Geniculate, Nodose etc), as well as helping keep track of what these nerves do. For each motor modality that a nerve contains, it will have a nucleus in the brainstem that corresponds to that. Somatic Motor nuclei are named for the nerve they contribute to (i.e. the III has an Oculomotor nucleus, the VII a facial nucleus etc). The only exception is the Nucleus Ambiguus, which is the somatic motor nucleus for IX and X. There are 4 peripheral Ganglia in the head (Ciliary, Pterygopalatine, Submandibular, and Otic). There are as many parasympathetic motor nuclei in the head (Edinger-Westphal, Superior salivatory, inferior salivatory, and Dorsal Motor Nucleus of the Vagus). This is often a point of confusion. First, remember that each nucleus will only exit via one nerve. Second, remember that the Trigeminal nerve lacks the modality of Parasympathetic motor and thus does not associate with these nuclei, where the Oculomotor carries the Edinger-Westphal (two modalities that exist in a purely motor nerve: this is the only property not predicted by the classification scheme in #1) to the Ciliary ganglion. Third, The Dorsal Motor nucleus supplies parasympathetic motor to the entire rest of the body, and thus does not have any function in the head. Thus, two nuclei are left to synapse on three peripheral ganglia. Hence, the Sup. Salivatory associates with two ganglia (the Pterygopalatine and Submandibular) and the Inf. Salivatory synapses on the Otic. (A figure is used to clarify) If a nerve contains somatic sensation, as do V, IX, and X (and maybe VII) it will associate with the Trigeminal nucleus/tract (this is where the 2nd order neurons lie). If the nerve contains visceral sensation (everyone but V meets this criteria due to taste), it will have some 2nd order neurons located in the solitary tract. The reasons for the origin of these tracts is explained in the section on evolutionary roots of structures. #3- Post and pre trematic distinction This concept is the key to remembering the primary branches of the 4 pharyngeal arch nerves. Personally, I detest remembering random details about what goes where, so taking a recognized term from embryology and running with it I devised a scheme to remember how the 4 toughest nerves divide their various branches up. It may appear confusing at first, however once understood it eventually gives order to a once chaotic system. Here are the rules: All 5 pharyngeal arch nerves (V, VII, IX, and X (it gives to two arches), are conceptually (despite the fact that they may not be physically) tri-pronged as in the way of the Trigeminal (though the prongs are seldom as distinct as the ones seen in the V). These three prongs are Post-trematic, Pre-trematic, and Pre-Pre-trematic. There is a diagram to explain all of this When I first heard the term pre-trematic, I initially inferred that the term “trematic” referred to the Helicotrema, the point in the cochlea where the scala vestibuli meets the scala tympani. I later read that this was false, however over time I have found that my error was actually rather helpful in describing the course of many nerves. Hence in this system, the term pre-trematic refers to a branch of each nerve that leaves the skull rostral to a plane through the helicotrema (try to correlate Netter plate 92 with plates 116 and 117 if this is completely confusing) The Pre-trematic branch of each nerve will always carry some type of sensation (somatic or visceral), will typically carry some type of Unconscious motor (not necessarily autonomic) at some point (this will be given off as its Pre-pre-trematic branch, but will never have any type of conscious motor, and will leave anterior to the plane of the helicotrema even if it has to do some serious backtracking (as with the chorda tympani). The pre-pre-trematic branch is one given off of the pre-trematic, and always will carry unconscious motor (I have to make this distinction in order to fit the Vagus into this scheme) for at least some part of its length, and will never have conscious motor. It often can have sensory branches. The post-trematic branches will always carry all the conscious motor of the nerve (sometimes this is one muscle), as well as at least some sensory component. It will NEVER have unconscious motor efferents running in it as a primary nerve (though it sometimes gets some of these from its pre-trematic partner). The final rule is that the Pre-trematic branch of one nerve will combine with the post-trematic branch of the previous arch’s nerve. Here is a listing of the nerves 1st Arch- Trigeminal- Pre-pre-V1 (unconscious motor to lacrimal gland for short time) PreV2- Sensory, no conscious motor, some unconscious motor (Via Pterygopalatine ganglion) which is given to Pre-pre Post- V3 Sensory, motor to muscles of mastication, etc 2nd Arch- FacialPre-pre- Greater Petrosal- Unconscious motor to Pterygop. gang. PreChorda Tympani- joins with V3 (lingual),sensory to ant 1/3 of tongue, unconscious motor so Sublingual and Submandibular PostFacial proper- Facial muscles, and Touch to auricle 3rd Arch-Glosso(IX)- Pre-pre- Lesser Petrosal- Unconscious motor to Otic PreTympanic Nerve of Jacobsen-sensation to tympanic membrane (cockroach in ear travels down this nerve to cause gag reflex) no conscious motor, gives off lesser Pet. Glossopharyngeal proper: Sensory-Posterior 1/3 of Posttongue, sensation to pharynx; Motor- Stylopharyngeus (it had to do something, OK 4th Arch-Upper (X)- Pre-pre- Part of Pharyngeal branch of X that controls Constrictors (i.e. unconscious motor) PrePharyngeal branch of Joins with Glossopharyngeal proper, sensory to lower pharynx (is physically same branch as Pre-pre) PostSuperior Laryngeal: Internal branch (epiglottic taste and touch above vestibular folds (i.e. false cord); External branch- motor to Cricothyroid (taking one for the team) 6th Arch-Lower (X)- Pre-pre- Vagal Nerves to the Cardiac plexus (unconscious motor) Vagal Nerves to the Cardiac plexus (visceral sensation) PrePost- Recurrent laryngeal sensation below vestibular folds, intrinsic laryngeal musculature A diagram is included to explain further. Correlating this with Netter plates 116-120 will make these branches stand out. #4- The Cartilages explain the weird musculature choices For those of you who do not remember the stuff from HD head and neck, I have enclosed a picture from Larsen on the topic. Each one of the above listed nerves has an associated cartilage, the understanding of which can allow one to remember the muscles that a nerve post-trematic (in the case of X the pre-pre-trematic (unconscious) also) branch innervates. This list focuses on the seemingly more random ones. 1st arch- Core of Mandible- all muscles that act on mandible (except Geniohyoid) this includes masseter, 2 pterygoids, temporalis, anterior belly of digastric, and myelohyoid (latter two depress mandible) Alisphenoid- (this includes the hamulus of Medial pterygoid)-tensor veli palatini Incus and malleus- Tensor tympani 2nd arch-Stapes- Stapedius Styloid, Stylohyoid ligament, Upper part of hyoid- two muscles run in this direction: stylohyoid and posterior belly of digastric 3rd arch- No cartilage will help with this one. IX in desperation to help my scheme out picked stylopharyngeus for its post-trematic branch 4th arch- Thyroid Cartilage- Cricothyroid Everything in the pharynx not already spoken for by V, VII or IX, No glossus-(XII) muscles (except palatoglossus) 6th arch- Cricoid and arytenoid cartilages- all intrinsic laryngeal muscles that touch these 2 cartilages without contacting thyroid cart (which excludes cricothyroid only) are innervated by recurrent laryngeal #5 Evolution and CNS The overall pattern of CNS organization, is that structures that are more rostral tend to have appeared later in evolution and thus tend to be involved in more complex activities than more caudal portions. While I have never read anything that explicitly stating that what I am going to say is accepted scientific dogma, the following inferences that I have made are greatly helpful for understanding the organization of cranial sensory tract, the 1st order ganglia, and the division of sensory pathways (plus I think I may be right on this one). The Trigeminal nucleus have 3 parts Mesencephalic (in the midbrain), Pontine, and the spinal nucleus of V (in the medulla). These nuclei contain the neurons for proprioception, touch, and pain (respectively). To remember this I view the fact that phylogenically older organisms (I usually envision worms)likely had little need for the control of complex limb movements (have you ever seen a worm try to hit a fastball...its ridiculous), as well as little use for discriminative touch. However, they do need to know that the fire on the left is not a good place to crawl into. As organisms evolved they slowly obtained more complex sensory apparati (i.e. pacinian corpuscles and muscle spindles) and thus had a need to attach 2nd order neurons for these modalities. In typical neuroevolutionary fashion, these neurons were attached to some rostral portion of the CNS. This is the reason why the pain/temp afferents synapse at the spinal level that they enter at, while the touch=proprio afferents run up to the medulla before meeting their 2nd order neurons: it is a newer system. To extend this further, this explains the Trigeminal nuclei: the proprioception 2nd orders are most rostral (mesencephalic) where as the pain, the older system is most caudal (spinal tract) and in fact is continuous with the spinal pain 2nd order neurons. Of note is the fact that the mesencephalic nucleus actually contains proprioceptive 1st order neurons (i.e. they don’t synapse there, nor are their cell bodies found in the dorsal root ganglion like are, but rather the 1st orders are in the nucleus itself and head down to the pontine nucleus of V to synapse on their 2nd orders) Netter plate 110-111 is good to study for this. The solitary tract has visceral sensations of two types: from the vital organs and taste. The taste is more rostral for the same reason as above, it is newer phylogenically and unlike its caudal brother, heads to the thalamus, cortex and hence consciousness. Every neuron in the PNS that contains sensation, must contain a ganglion that houses its first order neurons (think dorsal root ganglion). Nerves V, VII, IX, and X are no different. Here again, remembering the number of modalities (discussed in part 2) contained in a nerve (2,3,4,4 respectively) as well as the type contained, will allow us to understand the dorsal root ganglion like bumps near the nerve roots. The key to understanding this relationship is knowing that Visceral sensation and somatic sensation will have 1st order neurons in separate ganglia, and that if both types are present (i.e. in IX and X) the more complex modality evolutionarily (i.e. somatic-touch, pain) will be found as the higher of the two ganglia. If there are two ganglia, the superior one will be called jugular, the inferior one will have a unique name (i.e. petrosal or Nodose) V- This nerve only has one sensory modality (somatic) and thus has only one ganglion (Trigeminal) where all 1st orders (except proprio’s which are in mesencephalic nucleus) lie and eventually synapse on the trigem. nuclei in the brainstem. VII- Only one sensory modality (visceral- taste), thus has one ganglion (Geniculate) which has 1st orders that synapse on the solitary tract (made up entirely of 2nd orders) IX- Has two sensory modalities, and thus two ganglia. The upper is made up of somatic sensation 1st orders (touch and pain no proprio) and is called superior or jugular. Lower is called petrosal and has visceral (taste and carotid body) 1st orders which synapse in solitary tract X- Has two sensory modalities. The upper is somatic 1st orders and is known as jugular. The lower is Nodose and has visceral (taste and many visceral sensations) 1st orders (solitary tract). These type of questions are all over the green and red books. Netter 119 and 120 are good to look at for this. #6-Maxillary artery Now all we have left to figure out are the various branches of the Trigeminal nerve (methods for remembering and understanding all other branches have been previously described). V1, V2 (listed earlier as pre-trematic) and V3 (listed earlier as post-trematic), unlike most other nerves we have discussed have numerous branches. It so happens that if one knows the parts of the maxillary artery, one can determine the branches of V2 and V3 with only two modifications. Netter plate 35 is crucial here. The Maxillary artery has three portions Part 1- The mnemonic is MIM Middle meningeal, Inferior Alveolar, Muscular branches (to muscles of mastication Part 2- Has one branch- The buccal Part 3- This area is in the Pterygopalatine fossa, and has been depicted with the first two fingers and the thumb. I instead propose using the entire hand, with the ring and pinky fingers together and pointing downward. A figure is shown. The index finger represents the infraorbital, the thumb sphenopalantine, the middle finger is the Posterior superior alveolar, and the last two fingers represent the descending palatine which eventually branches into greater and lesser. To simplify what supplies teeth and what supplies palate, use the mnemonic: From superior to inferior: Teeth, palate, teeth, palate. Teeth 1- Infraorbital-goes through inf. orbital fissure and out infraorbital canal. While in the canal it gives off branches to the anterior teeth (Anterior Superior alveolar- it has two names because there is an inferior alveolar) Palate 1- Sphenopalatine- like thumb shows us, it passes medially through the sphenopalatine foramen where it supplies the nasal mucosa as the nasopalatine. It then passes through the incisive foramen to supply part of the hard palate. Teeth 2- Posterior Superior Alveolar- Comes off as middle finger shows, enters the back of the maxillary bone to supply the posterior teeth Palate 2- Descending palatine- passes down like ring and pinky fingers, and splits into greater and lesser palatines: these pass through their respective foramina to supply hard palate (greater) and soft palate (lesser). If we take the 1st two parts of the maxillary art and add a lingual branch, this is the pattern of V3-mandibular. If we take the 3rd part, insert the Pterygopalatine ganglion between the infraorbital and the greater/lesser palatines (where the descending used to be). These are all the branches of V2-maxillary. Correlate plate 35 with plates 40-41. Understanding this set up is crucial to understanding the flow in the high traffic area that is the Pterygopalatine ganglion. The sensory portions of the area follow branches of the artery. It is important to separate these from the efferent flow of the Vidian nerve, that connects to the ganglion straight from the posterior aspect as opposed to being running lateral to it and exchanging fibers (important for telling the difference). The Vidian nerve fibers enter the ganglion, the parasympath’s synapse (the sympath’s don’t because they have already synapsed in the superior cervical ganglion), and the fibers go to three places: 1) They hitch a ride up on V2 then V1 to the lacrimal gland 2) They have their own fibers to the nasal mucosa (thus these are non sensory and the sensory nerves are the sphenopalatine and the ethemoidals) 3) They run in the Greater/lesser palatines to cause salivation of the palate. (flip back to figure 2 if this is confusing) #7- The V1 mnemonic Because V1 wouldn’t yield to any good explanation I just made up a mnemonic V1 has three branches Frontal (supraorbital and supratrochlear), Nasociliary and lacrimal The mnemonic for the branches of the Nasociliary is LAPIS (the word for pencil). Long Ciliary- sensory to eye Anterior ethemoidal- sensory to the anterosuperior nasal septum and the tip of the nose Posterior ethemoidal- sensory to nasal septum Infratrochlear- terminal branch that runs under trochlea (pulley) of the superior oblique Short Ciliary- off Ciliary ganglion- carry sensation from eye to Nasociliary as well as autonomics to eyes #8- Oculomotor: The Exception The III breaks the 2 above listed rules. First, it is a purely motor branch that carries something besides pure somatic motor. Second, it has (as a consequence of the first part) 2 nuclei: one of which is not named after the nerve. Lesions III, IV, and VI- To understand how these nerves fail, one must first have knowledge of how the muscles work. The only two muscles that are pure are the lateral and medial recti. The others are not pure because they insert on a part of the eye that causes the muscle to not line up with the anteroposterior axis of the pupil. This is why a typical eye exam has someone follow the light laterally, then raise and lower the gaze (this lines the obliques up with the anteroposterior axis of the orbit (look at and thus they are raising and lowering the eyes with no interference from the recti).....the same process is repeated for the recti by moving medially and raising and lowering the gaze. A good picture for visualizing this is Netter 79. Here is the best explanation of this I can give. Superior Rectus- Inserts on the anterior, lateral part of globe. Thus when it pulls, it moves the front part of the eye upward, because of its angle, it pulls the front part of the eye inward, and thus adducts the gaze. And because it pulls the top of the eye inward it intorts the gaze by definition. Superior oblique- Pulls on back, lateral, and top of eye. Thus contraction pulls back of eye upward, and thus depresses gaze. It pulls back of eye inward, and thus front of eye is abducted, and intorted. Inferior oblique- Pulls on Back, lateral, bottom of eye- pulls back of eye down and thus elevates gaze, pulls back of eye outward, and thus abducts gaze, pulls bottom of eye inward, thus top of eye outward (extorsion) Inferior rectus- Pulls on Front, lateral, bottom of eye. Thus adducts (with superior rectus), extorts (with inferior obliques), and depresses (with superior oblique) Understanding this will allow us to comprehend lesions of the nerves. VI lesion- loss of VI causes loss of lateral rectus. Thus when one looks laterally onto side of lesion, the affected eye will not move as much as the unaffected eye in that direction. This causes the fovea of the two eyes to focus at different points, and thus leads to diplopia on lateral gaze. The affected eye now also lacks a lateral rectus to oppose the action of the medial rectus, and even though there are other muscles (the obliques) that can abduct the gaze, the eye has the tendency to deviate medially (medial strabismus). IV lesion- Loss of Superior oblique, can be compensated for with regards to depression and abduction (thus there is no serious strabismus) . However because the superior and inferior obliques oppose each other with regards to intorsion and extorsion, a IV lesion leaves the eye extorted due to loss of superior oblique’s intortion. Patients often present with head tilted towards opposite side of lesion (this causes inhibition on extorsion muscles (inf rectus and inf oblique) and minimizes inversion axis III lesion- Knocking out III in its entirety, (very commonly due to stoke of the posterior cerebral) leaves only the lateral rectus (abduction) and superior oblique (abduction, intorsion and depression) causes unopposed lateral deviation, intorsion, and depression (down and outward). As well as this, one loses the nerve to the pupillary constrictors leading to dilated pupil, and ptosis (full eyelid drooping due to loss of levator palpebrae) V lesion- lesions of V are usually described in terms of loss of various reflexes, most commonly the corneal blink (V1) but occasionally sneeze (V2), or Jaw-jerk (V3). Loss of corneal blink via V1 loss manifests itself as being able to touch the affected cornea without a response, with a bilateral response to touching the contralateral cornea. If a patient with a V3 lesion protrudes their jaw, there will be greater forces protruding the jaw on the unaffected side then on the injured side, thus the jaw will deviate towards the lesion. VII Lesion- This is crucial for the test (well and other things) To understand VII lesions, it is helpful to start distally and move proximally. Lesion in the periphery and/or parotid gland- Leads to Bell’s Palsy (includes inability to blink via loss of zygomatic branch of VII). A VII lesion as opposed to a V1 lesion will cause a loss of blink on either side, despite a reaction in the other eye to touch of either cornea. The patient will lack the ability to make “Muh” sound which is made by the lips. Lesion just proximal to stylomastoid foramen- all symptoms listed above plus loss of chorda tympani (pre-trematic branch) which causes lost of taste to anterior 2/3 and loss of sublingual and submandibular (as a side note, tying this into SBPM, the reason these two glands are innervated separately from the parotid, is because the parotid gland is purely serous (i.e. protein and water only) where as the other two glands are mixed serous and mucous. Separate innervation allows the nervous system to vary the concentration of the saliva.) Lesion just distal to Geniculate ganglion (or at ganglion): All of the above plus the nerve to the stapedius (2nd arch cartilage) leads to hyperacusis spares Lesion proximal to Geniculate ganglion (including at internal auditory meatus): If its proximal enough will take out greater petrosal (dry eye and nose) Netter plate 118 is good for viewing facial nerve course IX lesion- loss of gag reflex (it is the afferent), parotid gland and taste to posterior 1/3 of tongue X Lesion- With out the X, there is no elevation of the ipsilateral soft palate and thus the contralateral palate will elevate away from side of lesion and will tilt the uvula (if present) away from lesion side, this also prevents patient from making the “Kuh” sound which require palatal elevation. Lesion of other vagal branches cause loss of cough reflexes, loss of epiglottic feeling, tachycardic tendencies (due to cardiac vagal nerve involvement) and paralysis of intrinsic muscles of the larynx (recurrent). Bilateral recurrent loss causes inability to abduct vocal cord (due to loss of posterior cricoarytenoid) XI lesion- loss of Trapezius causes problems shrugging shoulders. Loss of SCM muscle cause difficulty in turning head to opposite side. XII lesion- this muscle inneverates all muscles that have the word glossus in them (except palatoglossus-which functionally should be named glossopalatus). A patient with a XII lesion will have greater genioglossus (which protrudes the tongue outward) on the unaffected side, and thus will push the tongue to the affected side (do the force-body diagram on that)...the mnemonic: Lick your wounds. A XII lesion also prevents the sound “La-La” due to the sound’s need of the tongue. Thus a simple test such as “muh-muh, kuh-kuh, la-la” rapidly tests three cranial nerves (7-10-12 in that order). This probably won’t be on this test, but is helpful to know for the future. One final note on the 12, It exits the skull via the hypoglossal canal, in the occipital bone. This bone arises from condensation of the occipital somites, which is also the origin of the muscles of the tongue, which migrated to their later place subsequently. As a result of its association with somites, the hypoglossal has a nucleus in the medial part (like all other purely motor/somite innervating nerves do). Swallowing The primary reason I am putting this as the only other section in the head and neck part is because there are alot of random muscles in the neck that don’t stick well unless you understand what they do. Here are my stages of swallowing, probably not the ones in most textbooks but its how I understand it. Relevant Netter plates are 49,58,59 and 24. Understanding the movement of the hyoid bone is crucial (this is plate 24). The hyoid bone serves as sort of a piston type apparatus to force food into pharynx and guide tongue to do the same. Stage one- Overall movement- tongue is placed between food and pharynx -Mylohyoid (V3), Anterior belly of Digastric (V3), and geniohyoid (superior root of ansa) are required to lift the tongue and hyoid forward in preparation to force hyoid backward. -Genioglossus (XII) presses tongue to teeth in preparation for this piston action Stage Two- Overall movement- The palate is elevated, the food is forced back into the pharynx, and the mouth is separated from pharynx in order to prevent backflow of food -Stylohyoid (VII), posterior belly of DG (VII), styloglossus (XII) pull hyoid back and force food into pharynx is a sort of “Ram-rod” fashion (see plate 24) -Tensor Veli palatini (V3) tenses palate (using the hamulus as a pulley) levator (X) lifts it, this moves the palate out of the way as well as protecting the nasal cavity from food -Palatoglossus (X) and Palatopharyngeus (X) close in order to a) prevent backflow of food that may occur when the constrictors contract and b) pinch a suitable smaller bolus off a larger bolus Stage Three- Overall movement- The Hyoid and tongue are retracted to allow food to go down, the pharynx is elevated, and the constrictors contract in order to force food through the upper esophageal sphincter -The strap muscles Sternothyroid, thyrohyoid, sternohyoid, and omohyoid (all Inferior ansa branches) retract hyoid to allow food to descend. the Hyoglossus (XII) does the same for the tongue. The sternothyroid and thyrohyoid also force the larynx into more of a v shape (this can be inferred from plate 24), the v shape helps protect the larynx from food -The Constrictors (X-pre-pre trematic) constrict to push food down into esophagus -The Salpingopharyngeus (X) and the stylopharyngeus (IX) elevate the pharynx. If you are wondering what this has to do with swallowing, then envision taking a bag full of leaves, turning it upside down and squeezing. The leaves would come out, however if you picked up the bag and lifted forcefully, this would cause the leaves to come out quicker. This lifting action is the purpose of the salpingo- and stylopharyngeus. The salpingo also pulls downward on the Eustachian tube, and effectively closes it, guarding the middle airway(plate 58 is good for visualizing this). Arm Brachial plexus and injury 1) The first thing you need to know is the order of its parts: The mnemonic is Real Texans Drink Cold Beer R=Roots- Come off ventral Rami of C5-T1 found between Anterior and Middle scalenes T=Trunks- Superior middle and inferior: exposed in posterior triangle of neck, D=Divisions- 3 trunks rearrange to form 3 cords, 3 anterior and 3 posterior, under clavicle C=Cords- lateral, medial and posterior, surround axillary artery B= Branches- In axilla proper, 5 main nerves to arm and other scapular area nerves 2) To remember all the little branches off of the plexus, I came up with this idea of tracks. To envision, a “track” envision the arm abducted so that the brachial plexus is horizontal. Then draw lines that separate the 3 trunks from each other and continue these onward through the terminal branches of the plexus (this is easier to do with the Netter plate 401) The upper “track” thus includes the superior trunk and lateral cord. The middle “track” is the middle trunk and posterior cord. The inferior track is the inferior trunk and medial cord. The reason I introduced this term is because it then simplifies remembering all the nerves. Because exactly 5 nerves come off each “track.” Upper “Track”1) Dorsal Scapular- Nerve to rhomboids and Levator scapulae (not one to stress over) 2) Suprascapular- gets 2 Spinatus muscles (supra and infra)- Tagged 3 times 3) Lateral Pectoral- Tagged once 4) 1/2 of Median 5) Musculocutanous Middle “Track”- STARS 1) Upper Subscapular -Tagged once- Subscapularis 2) Thoracodorsal (aka Mid subscapular)- Like artery of same name, goes to Lat Dorsi 3) Axillary 4) Radial 5) Lower Subscapular- gets Teres major Lower “Track” 1) Medial Pectoral- Tagged Twice 2) Medial brachial cutaneous 3) Medial antebrachial cutaneous- #2 and 3 are why the C8 and T1 dermatome run on medial part of forearm, correlate plates 401 and 150 and this will make sense 4) 1/2 of median 5) ulnar Throw in the long thoracic nerve which comes from roots C5-T1 (and is not on this test) and those are all of the Brachial plexus nerves. To finish off all the nerves (and to understand lesions of the plexus nerves) of the Arm a further discussion of the 5 most important nerves is in order. Posterior division nerves: Off Posterior Cord (aka medial track) Axillary: Comes off: Posterior cord- because posterior cord receives divisions from all three trunks, you would (or atleast you should) expect that the axillary nerve would receive contributions from C5-T1....alas it does not. Instead it receives only from C5-C6. If you have been following the discussion above you know that this means that only the superior trunk gives to the axillary. If you have instead been zoning out trying to find the random bit of info to cram, well here is the gist of this. The axillary nerve is the only major nerve (along with the lateral pec, and the suprascapular) that receives its only source of nerves from the superior trunk. Thus when the trunk is torn, (typically by landing on one’s shoulder), one loses only the axillary nerve in its entirety Branches are: One to deltoid and one to Teres Minor- Hence a axillary nerve loss would lead to weak Abduction of the shoulder (loss of deltoid) and External rotation (Teres minor loss).....this weakness becomes total loss when one tears the superior trunk and loses the suprascapular...in the process losing the supraspinatus (abductor) and infraspinatus (external rotator). Injury: Thus a tear of the superior trunk causes the arm to fall to the side and internally rotate (due to abduction and external rotation loss). Also resulting from this, is the loss of the subscapular nerves. Meaning loss of subscapularis (internal rotation) and teres major( loss of adduction) Imitating this you will see where the name of this syndrome, the waiter’s tip (aka Erb-Duchenne palsy) arises. Also because both of the axillary nerve muscles have backup muscles, you can see why a superior trunk injury is more severe than an axillary lesion. Radial: Comes off: The radial nerve comes off all the posterior cord, and thus receives contributions from all 5 roots Branches: Superficial and deep (in a trend that continues for many of the others the superficial gets cutaneous innervation, the deep focuses on muscle). The superficial radial involves cutaneous innervation to the area around the dorsal part of web space between the thumb and index, On the way it innervates the entire back of the arm and forearm The deep radial is nicknamed the “great extensor nerve” because it literally innervates every extensor muscle in the arm and forearm. as well as the supinator, the brachioradialis(its more of an elbow flexor but arises from the extensor tendon on lateral epicondyle) and the abductor pollicis longus (to keep track of this I think of hitchhiking the thumb action of which involves the extensors of the arm, abductor pollicis longus, and some brachioradialis, and some supinator) Because there are no intrinsic extensor flexor muscles in the hand, the radial nerve innervates no muscles in this area. Injury: Because the radial nerve receives from all 3 trunks, it is impossible for a proximal tear to completely wipe out the radial, thus the only tear that can cause radial nerve problems is to directly tear the nerve itself. Radial loss involves loss of supination extension, however it is of clinical (and thus examination interest) to note that 2 common lesions of the radial occur. The proximal lesion(aka saturday night palsy) causes complete loss of extensors. The distal (below the point where the nerve wraps around to the front of the arm) spares the triceps and the nerve to the anconeus and thus leads to wrist drop, loss of thumb extension and weakness of digit extension (though not total loss due to intrinsic muscles such as the lumbricals) Of note is the fact that a posterior cord lesion, as expected would lead to weak abduction, and ext. rotation, as well as saturday night palsy (wrist drop). This can be corrected by a splint that puts the wrist in extension and in doing so stretches the flexor digitorum superficialis and profundus. Anterior Division nerves: Off medial and lateral cords Musculocutaneous: Comes off: It is the Terminal branch of the Lateral Cord which in turn comes off the superior and middle trunks. Thus it receives innervation from C5-C7 and is not lost entirely in a superior trunk tear. Branches: It innervates the 3 muscles all of which contain the root brachi-, Biceps Brachii, Brachialis, coracobrachialis. It then continues on as the lateral antebrachial cutaneous (this is the C7 dermatome in the arm) Injury: Loss either via direct damage, or via laceration of the lateral cord (though not due to a single trunk injury) causes difficulty of flexion of the elbow, but not total loss because numerous wrist flexors (innvervated by the median and one by the ulnar) as well as the brachioradialis (innervated by the radial) remain intact to allow for some elbow flexion. Loss also leads to sensation loss in lateral forearm. Ulnar: Terminal Branch of medial cord. Because medial cord receives only from inferior trunk (C8-T1), a lesion of any of these components will cause ulnar loss. Branches (tagged a total of 5 times): Has a superficial branch that moves laterally and superficially to mediate cutaneous sensation around 4th and 5th digits (palmar and dorsal side) along with corresponding palm. Its deep branch gets the 2 medial lumbricals, all interosseus muscles, adductor pollicis, the deep head of flexor pollcis brevis (it is important to note that the FPB has a dual innervation, the superficial by the median, therefore median nerve lesion will not totally abolish thumb flexion). As well as this, during its course in the forearm, it gets the medial 1/2 of Flexor digitorum profundus and flexor carpi ulnaris. Injury: The common component of all injuries involving the ulnar nerve, is claw hand, and loss of sensation over 1.5 fingers. Claw hand results because due to loss of lumbricals, and interossei, the 4th and 5th fingers cannot be completely extended (ext digitorum doesn’t fully extend them), because of loss of 1/2 of flexor digitorum profundus this distal most phalanx of these two digits cannot be flexed. . As well as this there is no thumb adduction. Discussion of trunk and cord injuries simply involves adding additional symptoms to ulnar nerve injuries. Injury to the inferior trunk (due to violent upward pulling on arm.....a common cause, I’ve heard, is breach birth) leads to loss of arm adduction (medial pectoral) loss of feeling in entire medial arm (medial brachial and antebrachial cutaneous), as well as claw hand symptoms (ulnar). Medial cord trauma (because it only comes from the inferior trunk) will exhibit similar symptoms. Median: Comes off: The only nerve that involves more than one cord, it also receives contribution from all 3 trunks. Thus it is impossible to completely knock out the median via a proximal lesion Branches: In the forearm it gets all the flexor muscles except the ulnar most 1 1/2 (Flex. Carpi ulnaris, and 1/2 flex. digit. profundus), it then passes into hand where it gives off its recurrent branch (tagged 7 times) to the thenar muscles: abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis......as well as getting cutaneous innervation to the palmar side up to the lateral 1/2 of the ring finger and innervating the 1st two lumbricals. Injury: As stated above the Median nerve cannot be knocked out by the loss of any single trunk or cord (as is the only nerve that this applies to). A distal median nerve injury causes loss of much of wrist flexion (Flexor carpi radialis and palmaris longus) loss of some thumb flexion (flexor pollicis longus and superficial head of brevis) but not total loss (due to deep head innveration by ulnar). loss of some abduction (but not total because though the abductor Poll. Brevis is median the abductor poll longus is radial). The only total signs of a median nerve lesion is the inability to oppose the thumb (opponens pollicis) and a mild clawing of the 1st two fingers (the extension loss is due to lumbrical loss, the flexion loss is due to loss of flexor digitorum superficialis and profundus to those two fingers. Arteries Probably the most problematic of the arm are the ones that pass through the shoulder and neck (ie the subclavian and axillary). Both have an odd number of branches (subc= 3 and axillary=5) and the 2nd branch of both is an odd, 4 pronged trunk. For the subclavian, the first branch is the vertebral, the 3rd branch is the internal thoracic (from the 1st test) and the odd trunk in the 2nd slot is the thyrocervical trunk. The TC trunk has 4 branches: inferior thyroid, ascending cervical (run up somatic neck anterior to the transverse foramina), suprascapular (tagged once) and transverse cervical (typically the medial of the posterior bound branches). Note that though it is simpler conceptually to think of the suprascapular and transverse cerv. as branches off the TC trunk (and they typically do), they sometimes come off directly off the subclavian. As for the axillary, the trunk in the 2nd spot is the thoracoacromial trunk (not on this test). The other 5 branches come off via the mnemonic “slush“-SLSH: Superior thoracic (tagged once), Lateral thoracic (tagged on the 1st test), Subscapular (which terminates in circumflex scap. and thoracodorsal (goes to lat dorsi and has been tagged twice) and finally the Humeral circumflex (anterior and posterior: tagged once) Muscles To familiarize myself with all the muscles of the arm I grouped them into Threes. Based on names and functional characteristics The groups spell out the words TOPPED BEEF 3- Thenar “OAF” muscles3 hypothenar muscles 3- Other intrinsic muscles of hand (lumbrical, palmar and dorsal interossei) 3- Pronator/supinators 3- Pollicis longus muscles (abductor, extensor, flexor) 3- Exacerbate median nerve pain(ie run in carpal tunnel-flexor digitorum superficialis, profundus and flexor pollicis longus)- this is redundant with other groups but is important to know 3- Digitorum muscles (1 extensor, 2 flexor (superficialis and profundus) 3- Brachi muscles that flex elbow (brachialis, brachioradialis, biceps) 3- Extra extensors (Pollicis brevis, indicis, and digiti minimi) 3- Extensor Carpi muscles (1 ulnar, 2 radial (longus and brevis)) 3- Flexor Carpi muscles (1 ulnar, 2 radial (this includes palmaris longus- has this function) The goal is not to necessarily memorize the names of all the muscles but rather to familiarize yourself with them so that the nerve injuries make sense.