Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Psychoneuroimmunology wikipedia , lookup
Complement system wikipedia , lookup
DNA vaccination wikipedia , lookup
Adaptive immune system wikipedia , lookup
Duffy antigen system wikipedia , lookup
Molecular mimicry wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Biochemical cascade wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
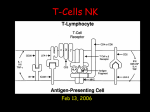
History of immunosuppressants Dr. 1st successful kidney transplant Dec 23, 1954 – Peter Bent Brigham Hospital, Boston MA – Dr. Joseph Murray 23 yr old identical twin brothers – No immunosuppression used – d. 1962 due to disease recurrence (glomerulonephritis) N Engl J Med 2004;351:2761-6 History of immunosuppression in transplantation Goals of immunosuppression (IMS) To prevent allograft rejection To prolong allograft functional life To optimise allograft function Prolong patient survival Improve patient quality of life To minimize toxicity of IMS agents – immunodeficiency complications – non-immune toxicities Transplantation and the immune system Recognition of allograft as non-self Donor and recipient antigen presenting cells (APC’s = dendritic cells, macrophages) – Present donor antigen to host T-lymphocyte Key event:= T-lymphocyte activation Immunosuppression: 3 ways to achieve Depletion of lymphocytes – Polyclonal antibodies (horse, rabbit anti-thymocyte globulin) – Mouse monoclonal anti-CD3 antibody (OKT3) – Humanized monoclonal anti-CD52 (alemtuzumab) – B-lymphocyte monoclonal anti-CD20 (rituximab) Diversion of lymphocyte traffic Blocking of lymphocyte response NEJM 2004;351:2715-29. Calcineurin inhibitors Anti-IL2 receptor Antibodies Corticosteroids Antigen presenting cell Basiliximab Daclizumab Ciclosporin Tacrolimus Helper T Lymphocyte A C T I V A T I O N Activated T Lymphocyte IL-2 IL-2 ILIL-2 R (High affinity) Antigen /T-cell receptor/ MHC II Everolimus Sirolimus P R O L I F E R A T I O N T Lymphocyte DNA synthesis T Lymphocyte Mycophenolic acid Azathioprine Immune system: 3 signal model of T-cell activation Signal 1: Antigen-specific signal Donor antigen is presented on APC (antigen presenting cell) T-cell recognized antigen as “non-self” Complex formed between MHC-AntigenTcell receptor (TCR) Immune signal is transduced through CD3 complex N Engl J Med 2004;351:2715-29. Signal 2: Non-antigen-specific co-stimulatory signal Binding of co-receptors between APC and T-cell – CD80/86 (aka B7) on APC with CD28 on Tcell “reinforces” and strengthens immune signal transduced through CD3 complex Combined action of signals 1 & 2 activate important intracellular pathways N Engl J Med 2004;351:2715-29. Combined action of signals 1 & 2 activate important intracellular pathways – Calcium-calcineurin pathway – RAS-MAP kinase pathway – Nulcear factor-κB pathway Leads to – production of IL-2 and other growth promoting cytokines – Expression of IL-2 receptor (CD25) N Engl J Med 2004;351:2715-29. Signal 3: Mammalian target of rapamycin (mTOR) activation IL-2 produced binds to newly activated IL2 receptor (CD25) Binding activates mTOR mTOR activation triggers cell cycle – Lymphocyte proliferation – Results in large numbers of effector T-cells N Engl J Med 2004;351:2715-29. Result of effector T-cells Effector T-cells targeted at donor antigen infiltrate graft – Interstitial and/or perivascular infiltration – Cascade of activation of macrophages, Bcells, plasma cells – Resultant cell lysis – Severe – edema, hemorrhage, vasculitis Three Signal Model of T cell Activation [adapted from Sing-Leung 2001] Antigen Presenting Cell Signal 1 Signal 2 MHC II B7 Antigen CD45 CD4 CD3 Signal 3 Interleukin-2 CD28 Interleukin-2 receptor TCR Calcineurin Pathway TOR Pathway Cytokine gene nucleus T Lymphocyte Purine Cell Cycle Synthesis Target lymphocyte Sites of Action of Immunosuppressive Medications [adapted from Sing-Leung 2001] Antigen Presenting Cell Steroids Signal 1 MHC II OKT3 ATG CD45 Signal 2 CD4 Calcineurin Pathway Steroids B7 Belatacept CD3 TCR Signal 3 CD28 Cyclosporine & Tacrolimus Anti-IL-2R Interleukin-2 Interleukin-2 receptor TOR Pathway Cytokine gene Cell Cycle nucleus T Lymphocyte Sirolimus MMF Purine Synthesis Target lymphocyte Individual Immunosuppressive Drugs and Sites of Action in the Three-Signal Model N Engl J Med 2004;351:2715-2729 Target Antigens Immunosuppressant drugs Anti-metabolites Calcineurin inhibitors – Ciclosporin A – Tacrolimus – Azathioprine – Mycophenolates – Leflunomide? m-TOR inhibitors – Sirolimus – Everolimus Newer antibody drugs Alemtuzumab Rituximab IL-2 receptor ‘mabs’ – Basiliximab – Daclizumab CNI’s: Tacrolimus and Cyclosporine Major breakthrough in modern transplantation Lead to significant improvements in outcome “Backbone” of most IMS protocols Similar mechanisms of action – Differ in structure and receptor interactions Transplant Proc 2004;36:25S-32S. Am J Kidney Dis 2006;47:S3-21. Calcineurin inhibitors (CNIs) : Mechanism of action Forms complex with cytosolic proteins (aka immunophilins) – CSA = cyclophilin – Tacrolimus = FKBP-12 (FK-binding protein) ↑ affinity and binding of immunophilin-drug complex to calcineurin Inhibits of transcription of IL-2, other cytokines ↓ T-cell activation & proliferation Transplant Proc 2004;36:25S-32S. Circulation 2004;110:3858-65. Calcineurin inhibitors (CNIs) Ciclosporin A (CyA) binds to intracellular protein, cyclophilin only active once bound Tacrolimus (FK506) binds to intracellular protein, FKBP-12 only active once bound The fungus Tolypocladium inflatum Fungal source of CyA Hydrophobic cyclic endecapeptide Scanning electron micrograph of Streptomyces tsukubaensis Bacterial source of tacrolimus Sirolimus from Streptomyces hygroscopicus & very similar structure Basic mode of action (Drug + immunophilin) inhibits calcineurin – Prevents dephosphorylation (activation) of NF-Act Tcell – factors which stimulate cytokine (i.e. IL-2/IFN-) gene transcription – Net result: impaired IL-2 production ‘reversible inhibition of T-cell activation, proliferation & clonal expansion’ – Stops cell cycle at G0-G1 stage Ciclosporin A & tacrolimus share a mechanism of action and metabolic route Never given together (additive nephrotoxicity) Tac interacting with CyA? 12-24hr gap only if converting Differences include ADR’s & efficacy Ciclosporin Oral absorption – Large inter & intra-patient variability – Food & juices – IV dose & administration Distribution – extensive (not dialysed) Metabolism – CYP450 3A4 with adult half-life 5-18 hours Shorter in children Steady state 2-3 days after change of dose Tacrolimus Absorption – Fatty food decreases rate & extent >80% distributes into erythrocytes – Whole blood trough levels – Remainder 99% protein bound CYP450 3A4 metabolism – Adult half-life approx 9-12 hours Clearance faster in <6yrs Metabolic interactions on CNI & m-TOR inhibitor levels Interacting drug Effect on blood level Erythromycin & clarithromycin Increased Diltiazem, nicardipine, verapamil Increased Fluconazole, itraconazole, ketoconazole, voriconazole Increased Rifampicin Decreased Carbamazepine Decreased Phenobarbital Decreased Phenytoin Decreased St John’s Wort Decreased Typical CNI doses target levels Calcineurin inhibitor Common initial oral doses Ciclosporin 5mg/Kg bd Tacrolimus 0.15mg/Kg bd Once daily? Typical target blood levels 0-6 months Greater 6 months 150 to 75 to 300ng/mL 150ng/mL 10 to 5 to 15ng/mL 10ng/mL Anti-metabolites Only purine anti-metabolites routinely used 1) Azathioprine 2) Two mycophenolate presentations – mofetil – sodium EC Azathioprine Guanine anti-metabolite – rapidly converted 6-mercaptopurine thioguanine nucleotides – Disrupts synthesis of developing cellular DNA & RNA strands & so prevent mitosis ‘Prevents early stages of activated T & Bcell proliferation’ One metabolic route involves thiopurine methyltransferase (TPMT). – Absent in 1 in 300 Toxicity Final metabolism to inactive 6-thiouric acid – Via xanthine oxidase Quarter dose in combination with allopurinol Usual starting dose 1-2mg/Kg – Can use 50% dose if giving iv Maintenance immunosuppression over first year after transplantation (1994-2003). (2005 OPTN/SRTR Annual report) Mycophenolic acid precursors Isolated in 1896 from Penicillium spp. mofetil ester rapidly cleaved active mycophenolic acid (MPA) 1 enzyme is rate limiting step in lymphocyte de novo purine biosynthesis – Inosine Mono-Phosphate DeHydrogenase Mycophenolic acid non-competitively inhibits IMPDH – Prevents production of Guanosine triphosphate (GTP) – Impairs production of DNA limiting lymphocyte proliferation T & B-lymphocytes preferentially use this pathway for purine production. – Other cell lines have salvage pathways. Molar equivalent doses: – 1gram MMF = 720mg MPS EC Paed MMF dose with ciclosporin 600mg/M2 bd MMF dose with tacrolimus = less (50-25%) – MPA glucuronide undergoes entero-hepatic recirculation – Second peak maintains levels – ciclosporin inhibits this recirculation MMF injection available if necessary – Same dose iv as oral – Requires aseptic manipulation Interactions Magnesium & aluminium (antacids) – Reduced absorption Cholestyramine – Reduced entero-hepatic recirculation (Val) aciclovir – Competes for tubular secretion with MPAG – Modest effect +12% MPAG AUC & +20% aciclovir AUC Pros & cons of mycophenolate Reduced incidence of ACR c.f. placebo or azathioprine with Sandimmune & steroid Lower incidence CAN c.f. azathioprine – Reduced interstitial fibrosis? Much more expensive than azathioprine Higher incidence of GI ADR - strategies diarrhoea 12.7 – 31.5% abdominal pain 11.5 – 26% nausea 4.2 – 14% and vomiting 2.4 – 12%. Higher incidence of anaemia (15%) Sirolimus Another macrocyclic antibiotic – Immunophilin binder (like CyA & FK506) also bind ubiquitous protein, FKBP-12 Does not inhibit cytokine (i.e. IL-2) gene transcription Complex inhibits m-TOR – Inhibits multiple biological steps e.g. activation of p70S6 kinase – Prevents IL-2-mediated signal transduction to cell nucleus Cell cycle arrest at G1-S phase Also inhibits tumour cell & smooth muscle cell proliferation (CAN) Absorption is poor – Food also affects rate & extent Consistency Widely distributed into tissues CYP450 3A4 & P-glycoprotein metabolism – Adult half-life long (57-63 hours) Clearance slightly higher in <11yrs cf 12-18yrs Levels 4-12ng/mL, no more frequently than every fortnight. Adverse effect profile dissimilar to CNIs – Not nephrotoxic – Wound healing delay & fascial dehiscence lymphocele formation – – – – – – – Mouth ulceration – transient? Topical steroid Acne and pilosebaceous rash - doxycycline Peripheral & angioedema >10% - withdrawal Dose related mixed hyperlipidaema - statins Anaemia & thrombocytopaenia Arthralgias – dose reduction or withdrawal Interstitial lung disease - withdrawal Adverse events leading to discontinuation Reason SRL (N=85) CNI (N=53) Chronic allograft nephropathy Raised creatinine Mouth ulcers Pneumonitis Rash Diarrhoea Other Adverse Event 0 1 1 6 2 10 3 10 1 0 0 0 0 0 Total 32 2 Transplantation 2003: 76; 364-370. Use of sirolimus Licensed for use with ciclosporin A for 1st 3 months only in adult renal transplant – Rarely used in this way Where to position sirolimus? – Replace CNI or replace anti-metabolite Appears to offer better GFR (graft survival?) than CNI maintenance. Skin cancers?? Alemtuzumab Licensed for chronic lypmphcytic leukaemia Recombinant humanised mab vs CD52 – CD52 cell surface antigen T&B lymphocytes, monocytes, macrophages Depleting mab – Binds and leads to immediate cell lysis Single 30mg dose leads to profound lymphocyte depletion – Persists 6-12 months before recovery – Optimal dose, frequency & timing unknown Mainly as induction immunosuppression Instead of rATG or IL-2R mabs – Also used to treat acute rejection Very limited RCT evidence Similar 1 year graft/patient survival & ACR incidence to basiliximab, dacilzumab & rATG Infusion-related ADRs very common – Fever, rigors, hypotension, urticaria, hypotension, bronchospasm, ARDS, arrest – Must be infused over 2 hours Preceded by iv MePred, Piriton & paracetamol Pancytopenia, leukopenia, thrombocytopenia Rituximab Chimeric mouse/human mab vs CD20 – CD20 cell surface antigen Pre-B & mature B lymphocytes – Not stem cells or other cell lines Depleting mab – Inhibits B cell proliferation Reduces PRA titre – New, healthy cells regenerate 9-12 months Effects still apparent at 15 months Role of rituximab in transplant unclear – Licensed for lymphoma/leukaemia & autoimmune disorders Humeral rejection episodes Some data but no local experience Pre-transplant, pre-conditioning regimes – High donor-relevant HLA antibody titre With DFPE, IVIG (?), mycophenolate Single doses 375mg/M2 – ABO incompatible transplant Early infusion-related ADRs in > 50% – Classic ‘cytokine –release’ syndrome – Fever, rigors, hypotension, urticaria, bronchospasm, angioedema, ARDS, death – Infusion started slowly and rate adjusted Preceded by iv steroid, Piriton & paracetamol Tumour-lysis syndrome association Leucopaenia/thrombocytopenia – Less common than with alemtuzumab Anti-CD 25 antibodies Two IL-2 receptor (IL-2R) ‘mabs’ – Daclizumab – Basiliximab Both ‘humanised’ monoclonal antibodies against the chain of IL-2R – aka anti-Tac/CD25 antibodies Bind to, saturate & block activated IL-2R – don’t affect resting T-cells Both manipulated to prevent patient antibody formation – unlike OKT3 or ???Thymoglobuline Used exclusively as induction agents – Duration Pooled analysis for anti-CD 25 antibodies Biopsy confirmed acute rejection absolute difference (95% CI) Biopsy confirmed acute rejection odds ratio (95% CI) Daclizumab versus placebo -16% 0.48 (-24% to –8%) (0.33 to 0.70) Basiliximab versus placebo -14% 0.51 (-20% to –9%) (0.40 to 0.65) New Engl J Med 1998: 338; 161-165 Transplantation 1999: 67; 110-115 Lancet 1997: 350; 1193-1198 Transplantation 1999: 67; 276-284 Transplantation 2001: 72; 1261-1267 IL-2R blocking ‘mabs’ Advantages – reduce renal rejection rates by approx 30% in classic triple therapy – short courses iv, in hospital only Compliance guaranteed – ‘Few’ adverse effects Severe re-exposure hypersensitivity seen with both Disadvantages – Cost But cost-effective to add basiliximab to ciclosporin regimens Same report states that should not be added to tacrolimus based regimens. – Daclizumab is a 5 dose, fortnightly regimen & requires infusion