Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Vaccination policy wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Social immunity wikipedia , lookup
Molecular mimicry wikipedia , lookup
Childhood immunizations in the United States wikipedia , lookup
Whooping cough wikipedia , lookup
Immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Herd immunity wikipedia , lookup
Anaphylaxis wikipedia , lookup
Adaptive immune system wikipedia , lookup
Innate immune system wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Food allergy wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
DNA vaccination wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
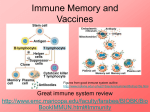
The immune system and anaphylaxis [email protected] About the immune system The immune system Protects the body from infectious organisms, foreign bodies and malignancies Surface barriers Innate immunity Acquired immunity 3 Key issues 4 • Discrimination between self and non-self • Sufficient but not excessive immunity • The right kind of response • A response in the right place at the right time • Sufficiently quick to prevent damage Antigens 5 • Immune system works by identifying antigens • Antigen is anything recognised by the immune system; immunogen provokes immune response • A bacterium will contain many antigens • Immune system does not have to recognise them all Antigens An antigen is a molecule that is recognised by the immune system; an immunogen provokes an immune response A single bacteria will contain many hundreds of individual antigens Vaccines contain differing numbers depending upon their formulation Sometimes referred to as the valency Diphtheria Tetanus Whole cell pertussis Acellular pertussis Offitt (2002) Pediatrics 109 124-129 1 1 3 000 5 Active antigens, may contain others such as antibiotics and preservatives Influenza Vaccine components 2014/5 A/California/7/2009 (H1N1)pdm09-like virus A/Texas/50/2012 (H3N2)-like virus B/Massachusetts/2/2012-like virus Quadrivalent vaccine B/Brisbane/60/2008-like virus Vaccines for use in the 2015/2016 influenza season (northern hemisphere winter) A/California/7/2009 (H1N1)pdm09-like virus A/Switzerland/9715293/2013 (H3N2)-like virus B/Phuket/3073/2013-like virus Quadrivalent vaccine B/Brisbane/60/2008-like virus WHO (2015) WER 90, 97–108 Overview Innate (non-specific) Acquired (specific) Neutrophils T lymphocytes Macrophages T helper cells (CD4) Natural killer cells T cyototoxic (CD8) Acute phase proteins B lymphocytes Complement Plasma cells Dendritic cells 10 Memory cells Lymphocytes Four main classes 1. B (plasma cell) 2. T cell Helper (CD4) Cytotoxic (CD8) 3. Natural regulatory (nTreg) 4. Natural killer cells (NK) - innate 11 Antibody classes IgA IgD IgE IgG IgM mucosal, no maternal transfer but found in breast milk bound to B cells general inflammation, macroparasites main serum antibody, maternally transferred produced by naive plasma cells Immunoglobulins and infants • IgG transferred maternally • The process is active, but immunity is passive • Provides immunity to everything the mother has immunity to • Declines over first 6 months of life, all gone by 18 months • No IgA which is important for mucosal immunity • IgA from breast milk Primary and secondary immune responses The ‘problem’ of immunity • Balancing the need to rid the body of a foreign body with the avoidance of damage • May result in hypersensitivity, damage caused by an immune respsonse • Gell and Coombs (1963) suggested 4 types 1. Allergic/anaphylactic 2. Antibody dependent cytotoxic 3. Immune complex 4. Delayed type About anaphylaxis Anaphylaxis Allergy - a hypersensitivity reaction initiated by specific immunologic mechanisms Atopy - a personal and/or familial tendency, usually in childhood or adolescence, to become sensitized and produce IgE antibodies in response to ordinary exposures to allergens, usually proteins Anaphylaxis - a severe, life-threatening generalized or systemic hypersensitivity reaction Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization J Allergy Clin Immunol 113-832-836 Pathology IgE-mediated Initial sensitization stage Subsequent anaphylactic response Sensitisation stage Exposure to antigen (allergen) Plasma cells (B cells) produce specific IgE in response to allergen Circulating IgE antibodies attach to mast cells and basophils Anaphylactic response Subsequent dose of same allergen invades body Allergen binds to IgE attached to mast cells and basophils This triggers degranulation and release of histamine/other chemical mediators Type 1 hypersensitivity - allergy Antigen acts as allergen B cell produces large amounts IgE IgE binds to mast cell Subsequent exposure allergen cross links bound IgE leading to degranulation Rochester Institute of Technology Substances released during degranulation Histamine Capillary dilation and permeability Oedema Chemoattraction Nerve irritation Proteoglycans, mainly heparin Serine proteases Prostaglandin D2 Leukotriene C4 Various cytokines Clinical signs Skin Flushing, pruritus, urticaria, angioedema Upper respiratory Congestion, rhinorrhea Lower respiratory Bronchospasm, throat or chest tightness, hoarseness, wheezing, shortness of breath, cough Gastrointestinal tract Oral pruritus Cramps, nausea, vomiting, diarrhea Cardiovascular system Tachycardia, bradycardia, hypotension/shock, arrhythmias, ischemia, chest pain 42 How it looks in the Green Book 1. Send for additional health professional assistance 2. Send a responsible adult to dial 999 and state that there is a case of suspected anaphylaxis 3. Stay with the patient at all times 4. Lie the patient down, ideally with the legs raised (unless the patient has breathing difficulties) 5. Administer oxygen if available 6. If breathing stops, mouth to mouth/mask resuscitation should be performed 7. If there is no pulse, start cardiopulmonary resuscitation All patients with clinical signs of shock, airway swelling or definite breathing difficulties should be given adrenaline 1:1000 IM The preferred site is the mid-point of the anterolateral aspect of the thigh Doses The intramuscular doses we recommend are for healthcare staff who rarely deal with paediatric emergencies The doses have been chosen because they are easy to draw up and administer and are within the safe acceptable dose ranges for the particular age groups Needles IM injection - blue needle (25 mm 23 G) Best site for IM adrenaline is the anterolateral aspect of the middle third of the thigh Needle needs to be long enough to ensure that the adrenaline is injected into muscle Current RC UK guidance states that a 25 mm length needle is best and suitable for all ages If obese a longer needle may be needed (38 mm) Standard orange needle is only 16 mm in length which can result in injecting the adrenaline SC Vaccine related anaphylaxis Between 1997 and 2003, there were 130 reports to the MHRA and no reported deaths 117 million doses of all vaccines were supplied to hospitals and GPs This equates to a rate of approximately 1:1 000 000 vaccine doses Usually occurs in people without history Risk of anaphylaxis after vaccination of children and adolescents 4 HMOs USA, looked for ICD-9 codes suggestive of anaphylaxis Vaccinations administered n = 7 644 049 Initially reviewed 657 diagnoses of interest 6 probable or possible anaphylaxis 1 not vaccine related = 5 cases = 0.65 per million doses (CI 0.21-1.53) 3 questionable regarding vaccine or outcome =2 cases = 0.26 per million doses (CI 0.03-0.95) Bohlke (2003) Pediatrics 112 815-820 Adrenaline shock packs Check Dosage/resuscitation card The expiry dates on adrenaline shock packs must be checked regularly Packs are sealed, if opened, do not use and do not add anything to the pack Protect from heat, light and moisture Packs do not need to be refrigerated Avoid prolonged exposure to heat Return expired packs to pharmacy Contents adrenaline shock packs 3 x 1 ml adrenaline injection 1:1000 3 x 1 ml syringes 3 x blue needles 23G 3 x green needles 21G Dosage/resuscitation card The ‘problem’ of immunity • Balancing the need to rid the body of a foreign body with the avoidance of damage • May result in hypersensitivity, damage caused by an immune respsonse • Gell and Coombs (1963) suggested 4 types 1. Allergic/anaphylactic 2. Antibody dependent cytotoxic 3. Immune complex 4. Delayed type The following conditions are contraindications to routine immunisation All vaccines are contraindicated in those who have had: • A confirmed anaphylactic reaction to a previous dose of a vaccine containing the same antigens, or • A confirmed anaphylactic reaction to another component contained in the relevant vaccine, e.g. neomycin, streptomycin or polymyxin B (which may be present in trace amounts in some vaccines) Egg allergy Individuals with a confirmed anaphylactic reaction to egg should not receive yellow fever vaccine Individuals who have egg allergy may be at increased risk of reaction to some influenza vaccines All children with egg allergy should receive the MMR vaccination as a routine procedure in primary care Latex allergy History of anaphylactic allergy to latex, vaccines supplied in vials or syringes that contain latex should not be administered, unless the benefit of vaccination outweighs the risk of an allergic reaction to the vaccine Immunesuppression Live vaccines can, in some situations, cause severe or fatal infections in immunosuppressed individuals due to extensive replication of the vaccine strain. For this reason, severely immunosuppressed individuals should not be given live vaccines, and vaccination in immunosuppressed individuals should only be conducted in consultation with an appropriate specialist Pregnancy There is a theoretical concern that vaccinating pregnant women with live vaccines may infect the foetus. There is no evidence that any live vaccine (including rubella and MMR) causes birth defects. However, since the theoretical possibility of foetal infection exists, live vaccines should generally be delayed until after delivery Note injected influenza and pertussis are not live vaccines Timing Observe patient for 10 minutes Most reactions occur within 2 minutes Another adult should be present What to do if worried Discuss with patient/parents Don’t vaccinate Refer to local vaccine co-ordinator Most hospitals run vaccination clinics