Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Extrachromosomal DNA wikipedia , lookup
No-SCAR (Scarless Cas9 Assisted Recombineering) Genome Editing wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Cell-free fetal DNA wikipedia , lookup
Bisulfite sequencing wikipedia , lookup
X-inactivation wikipedia , lookup
Designer baby wikipedia , lookup
Microevolution wikipedia , lookup
Genomic library wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Comparative genomic hybridization wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
History of genetic engineering wikipedia , lookup
Genome (book) wikipedia , lookup
Vectors in gene therapy wikipedia , lookup
Cancer epigenetics wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Polycomb Group Proteins and Cancer wikipedia , lookup
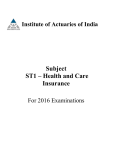
Oncogene (2001) 20, 6245 ± 6249 ã 2001 Nature Publishing Group All rights reserved 0950 ± 9232/01 $15.00 www.nature.com/onc Loss of heterozygosity analysis de®nes a 3-cM region of 15q commonly deleted in human malignant mesothelioma Assunta De Rienzo1, Binaifer R Balsara1, Sinoula Apostolou1, Suresh C Jhanwar2 and Joseph R Testa*,1 1 Human Genetics Program, Fox Chase Cancer Center, Philadelphia, Pennsylvania, PA 19111, USA; 2Department of Human Genetics, Memorial Sloan-Kettering Cancer Center, New York, NY 10021, USA Previous comparative genomic hybridization and allelic loss analyses demonstrated frequent deletions from 15q11.1 ± 15 in malignant mesothelioma. Recurrent losses of 15q11 ± 22 have also been reported in several other tumor types such as breast and colorectal cancers. To more precisely map the commonly deleted region, we have performed a high density loss of heterozygosity analysis of 46 malignant mesotheliomas, using 26 polymorphic microsatellite markers spanning the entire long arm of chromsome 15. Allelic loss from 15q was observed in 22 of 46 (48%) cases. These analyses have de®ned a minimally deleted region of *3-cM, which was con®rmed to reside at 15q15 by ¯uorescence in situ hybridization analysis with yeast arti®cial chromosome probes. No tumor suppressor genes have been reported to map to this site. The minimally deleted region identi®ed in this investigation overlaps those observed in other kinds of cancer, and is the smallest site of recurrent 15q loss identi®ed to date in human tumors. The identi®cation of this commonly deleted site implicates a putative tumor suppressor gene(s) at 15q15 involved in diverse forms of human neoplasia. Oncogene (2001) 20, 6245 ± 6249. Keywords: malignant mesothelioma; LOH; chromosome arm 15q; tumor suppressor gene Human malignant mesotheliomas (MMs) are highly aggressive tumors that arise from mesothelial cells lining the pleural, peritoneal, and pericardial cavities (Antman, 1981). More than 2000 cases of MM are diagnosed annually in the USA, and the incidence is expected to steadily increase worldwide until the year 2020 (Attanoos and Gibbs, 1997). Exposure to asbestos is known to be a major contributor to the development of this malignancy (Craighead and Mossman, 1982). It is unknown whether asbestos ®bers act directly on mesothelial cells, or indirectly, via formation of reactive oxygen species and/or increased growth factor *Correspondence: JR Testa; E-mail: [email protected] Received 13 April 2001; revised 29 June 2001; accepted 12 July 2001 receptors (Mossman et al., 1996; Pache et al., 1998). Recent investigations have also implicated simian virus 40 (SV40) in the etiology of some MMs (Testa et al., 1998). It has been postulated that SV40 and asbestos could act as co-carcinogens, and that individuals who are SV40-positive may be at a higher risk of developing mesothelioma when exposed to asbestos (Carbone et al., 1999; Testa et al., 1998). MM is characterized by a long latency from the time of asbestos exposure to clinical diagnosis (Lynch et al., 1985), suggesting that an accumulation of multiple somatic genetic alterations may be required before a mesothelial cell is converted into a neoplastic cell. The most common cytogenetic aberrations in MM are deletions involving discrete regions in chromosome arms 1p, 3p, 4q, 6q, 9p, 13q, 14q, 15q and 22q (Balsara et al., 1999; Bell et al., 1997; Bjorkqvist et al., 1997, 1999; De Rienzo et al., 2000; Popescu et al., 1988; Shivapurkar et al., 1999; Taguchi et al., 1993). The high frequency of speci®c chromosomal losses suggests a recessive tumorigenic mechanism in this cancer, and the inactivation of tumor suppressor genes (TSGs) residing in these deleted chromosomal regions may contribute to the development and/or progression of MM (Taguchi et al., 1993). Loss of heterozygosity (LOH) is the most frequent type of genetic alteration found in many kinds of malignancies. LOH occurs as a consequence of deletions, whole chromosome losses, or aberrant mitotic recombination events (Seemayer and Cavenee, 1989; Weinberg, 1993) and can reveal the presence of a recessive mutation in the remaining allele of a TSG localized within the aected region of the genome (Knudson, 1989). Previously, we used comparative genomic hybridization analysis to identify a new common region of deletion, 15q, in MM (Balsara et al., 1999). LOH analysis on eight MM cases with 16 microsatellite markers con®rmed a common region of deletion at 15q 11.1 ± 15 (Balsara et al., 1999). To more precisely localize the minimal region of 15q loss in MM, we here report allelic loss studies on a much larger series of MMs, using 26 polymorphic DNA markers spanning 15q. The location of each marker from the centromere to the telomere and the corresponding distances in cM are shown in Figure 1. 15q losses in mesothelioma A De Rienzo et al 6246 Figure 1 Pattern of LOH in MMs exhibiting deletions in 15q. Thick vertical bar, designated by SRO, indicates the minimal region of overlapping deletion. Markers, with corresponding cM distances, are shown in the predicted order from the centromere to the telomere. For each locus, the overall frequency of allelic loss is shown at the right. Primer pairs used for polymerase chain reaction (PCR) ampli®cation of tetra, tri-, and dinucleotide repeat markers were obtained from Research Genetics. The chromosomal location of the markers and their relative order were ascertained from either the Genetic Location Database, University of Southampton (Collins et al., 1996) and the Center of Medical Genetics Database, Marsh®eld Medical Research Foundation (Broman et al., 1998). PCR was performed in a ®nal volume of 5 ml with 20 ng of genomic DNA, 75 ng of each primer, 50 mM of each dNTP, 1 unit of AmpliTaq DNA polymerase (Perkin Elmer), and 0.2 mCi [a-32P]-dCTP (DuPont NEN), using a Hybaid OmnE Thermal Cycler. Ampli®cation conditions consisted of an initial denaturation of 5 min at 948C followed by 35 cycles of 1 min at 948C, 1 min at 55 ± 578C and 1 min at 728C, with a ®nal extension of 10 min at 728C. PCR products were diluted 1 : 1 with 95% formamide gel loading buer. Three ml of each PCR product were separated electrophoretically in a 6.5% denaturing (8 M urea) polyacrylamide gel. Gels were dried at 808C under vacuum and subjected to autoradiography at room temperature for 2 ± 6 h. LOH was scored when constitutional heterozygosity in control DNA and complete loss of one allelic band in the tumor cell line DNA was observed Tumor specimens were surgically resected primary pleural MMs from newly diagnosed patients. Criteria for the diagnosis of MM were in accordance with established guidelines (Antman et al., 1989). Forty-six tumor cell lines were established from primary MM cultures as described previously (Taguchi et al., 1993), and genomic DNA was isolated by standard methods. Allelic patterns of DNA from 19 tumor cell lines were compared with those from matched blood samples. Matched peripheral blood was not available for the remaining 27 cell lines. In these cases, the constitutional allelic pattern was determined from DNA obtained from tumor tissue containing a mixture of tumor and normal cells. Among the 46 MMs examined, 22 (47.8%) displayed allelic loss of at least one marker (Figure 1). Nine of these cases exhibited allelic loss of all informative markers, presumably because of whole chromosome loss. Case 17 displayed allelic loss of all markers except D15S1031. The remaining 12 cases showed interstitial Oncogene deletions, 11 of which were overlapping. The exception, case 7, displayed allelic loss only at GATA153F11, which may represent a nonspeci®c event because this locus showed a relatively low overall frequency of allelic loss. Analysis of the LOH patterns of the cases with overlapping interstitial deletions revealed a shortest region of overlap (SRO) of approximately 3 cM, located between markers D15S1007 and ACTC at 15q15.3. The proximal boundary was de®ned by case 13, which retained both alleles at D15S1007 (Figure 2A). Case 49 delineated the distal boundary, with retention of both alleles at marker ACTC (Figure 2B). The frequencies of LOH in the minimally deleted region were 42.9% (15 of 35) at D15S1040 and 40.7% (11 of 27) at GATA50C03. An even higher frequency of LOH was observed at D15S144, which resides slightly proximal to the SRO (Figure 1); however, the number of cases informative for D15S144 was considerably lower than that for any marker in 15q15. 15q losses in mesothelioma A De Rienzo et al 6247 Figure 2 Representative autoradiograms showing allelic band patterns at several loci within 15q. Case numbers are indicated below each panel. Alleles recognized by microsatellite markers are depicted by dots (.). Arrowheads: allelic loss. Letters above panels indicate DNA from tumor cell line (C), primary tumor (T), and normal peripheral blood (B) Matched tumor, blood, and cell line DNAs were available for four of 46 MMs with allelic loss in 15q15. DNA from the tumor specimens exhibited reduction in the intensity of the allelic band corresponding to the one unequivocally lost in the matched cell line (Figure 2B), suggesting that LOH seen in the MM cell lines is representative of that observed in the corresponding tumor specimens. The SRO was con®rmed by two-color ¯uorescence in situ hybridization (FISH) analysis using YACs containing loci immediately ¯anking or within the SRO. Three YACs (812-C-4, 908-C-5, and 822-G-2) contained marker D15S1040, from the SRO, as well as one or more ¯anking markers (Figure 3). However, each of these YACs was found to be chimeric and, thus, was excluded from further analysis. YACs 775-D-2 contained D15S1007 and other markers located proximal to the SRO, whereas 947-F-7 and 914-A-2 contained D15S971, which is distal to the SRO. YAC 947-F-7 was excluded because it was chimeric. FISH analysis was performed with YACs 775-D-2 and 914-A-2 on cases 13 and 49, which collectively delineated the SRO. Case 13 showed loss of 914-A-2, while YAC 775-D-2 was retained (Figure 4). FISH analysis for case 49 revealed multiple copies (3 ± 4 each) of two dierent marker chromosomes which hybridized to YACs 775D-2 and 914-A-2. One marker exhibited overlapping signals for each YAC. The other marker showed loss of 775-D-2, and retention of YAC 914-A-2 (data not Figure 3 Diagrammatic representation of YAC contig in 15q15. Markers are shown on the top in the predicted order from the centromere to the telomere. Horizontal bars represent YACS. We identi®ed YACs located in the vicinity of the 15q15 SRO using the Center for Genome Research Database, Whitehead Institute for Genome Research. Yeast strains carrying the YACs were obtained from Research Genetics. To verify the positions of these YACs relative to our SRO, we carried out PCR analysis to determine which YACs contained the following markers: D15S1007, D15S1040, ACTC, GAAA11C1, and D15S971. DNA was puri®ed from yeast strains by standard methods, and PCR analysis was performed to determine which YACs contained markers ¯anking or residing within the SRO. Each PCR reaction was performed in a ®nal volume of 20 ml with 20 ng of yeast DNA, 100 ng of each primer, 50 mM of each dNTP, and 1.2 units of AmpliTaq DNA polymerase, using the same ampli®cation conditions described in Figure 1 shown). Collectively, these results con®rm that the minimally deleted region resides at 15q15. MM is characterized by recurrent chromosomal deletions involving discrete regions in 1p, 3p, 4q, 6q, 9p, 13q, 14q, 15q and 22q (Balsara et al., 1999; Bell et al., 1997; Bjorkqvist et al., 1997, 1999; De Rienzo et al., 2000; Seemayer and Cavenee, 1989; Shivapurkar et al., 1999; Taguchi et al., 1993), suggesting that each of these regions harbors a putative TSG whose loss/ inactivation may contribute to the pathogenesis of this malignancy. Thus, far, TSGs within two of these chromosomal regions, CDKN2A/ARF (encoding the alternative products p16INK4a and p14ARF) at 9p21 and NF2 at 22q12, have been implicated in MM. Homozygous deletions appear to be the major mechanism aecting CDKN2A in MM (Cheng et al., 1994). Inactivating mutations coupled with allelic loss occur at the NF2 locus (Bianchi et al., 1995; Cheng et al., 1999; Sekido et al., 1995). Recently, we identi®ed a minimal region of chromosomal loss in 15q11.1 ± 15 in MM (Balsara et al., 1999). In this study, we have re®ned the region of chromosomal loss, de®ning a 3-cM region between D15S1007 and ACTC, and the location of the SRO was con®rmed to be at 15q15 by FISH mapping. Several studies have reported recurrent deletions of 15q in various types of cancer. In ovarian carcinoma, 15q losses have been proposed as a late event observed in most high-grade and in a subset of low-grade tumors (Dodson et al., 1993). Wick et al. (1996) reported LOH Oncogene 15q losses in mesothelioma A De Rienzo et al 6248 Figure 4 Two-color FISH analysis showing heterozygous loss of YAC 914-A-2 and retention of both copies of YAC 775-D-2 in MM case 13. Rhodamine (red) signal: YAC 775-D-2; FITC (green) signal: YAC 914-A-2. Partial metaphase spread shows single copy of normal chromosome 15 with signals for both YACs (arrow) and a deleted chromosome 15 with loss of signal for YAC 914-A-2 (arrowhead). Note that overlapping portions of the adjacent green and red signals in the normal chromosome 15 appear yellow. FISH was performed using biotin-16-dCTP and digoxigenin-11-dUTP. Probes were labeled by random ocatamer priming at 378C for 1 h, followed by ethanol co-precipitation with Cot1 DNA. Hybridization was carried out on metaphase spreads from phytohemagglutinin-stimulated normal lymphocytes and MM cells from case 13, as described previously (Altomare et al., 1996). Hybridization of biotinylated probes was detected with FITC-avidin (Oncor), and hybridization of digoxigenin-labeled probes was detected with anti-digoxigenin rhodamine (Boehringer Mannheim). Chromosomes were counterstained with 4', 6'diamidino-2-phenylindole. Images of chromosomes and hybridization signals were captured separately using a cooled CCD camera (Photometrics), pseudo-colored, then merged using computer imaging software from Oncor from 15q in 42 of 99 (42%) primary and metastatic breast carcinomas, with the SRO residing between D15S231 and D15S641, another 15q15 marker, which resides between D15S971 and D15S118. The frequency of 15q loss was signi®cantly higher in metastatic cases. Deletions of 15q have also been reported in 35% of parathyroid adenomas, with two common regions being observed, one at 15q11 ± 21 and another at 15q26-qter (Tahara et al., 1996). Kersemaekers et al. (1998) described a novel site with frequent LOH on 15q in carcinoma of the uterine cervix. They analysed only three markers from 15q and concluded that a novel TSG may be present at 15q21. Allelotype analysis has also demonstrated recurrent losses of 15q in small cell lung carcinomas, although only a few markers on this chromosome were evaluated (Stanton et al., 2000). To evaluate the possible existence of colorectal cancer susceptibility genes, a large family with multiple colorectal adenomas and carcinomas was investigated by linkage analysis (Tomlinson et al., 1999). All aected individuals shared a haplotype of marker alleles in a 40-cM interval de®ned by D15S1031 and Oncogene D15S153 at 15q14 ± q22. LOH analysis of sporadic colorectal tumors identi®ed an SRO at 15q21.1 (Park et al., 2000). However, the region between D15S1040 and D15S971, where our SRO resides, was not analysed. Taken collectively, these investigations suggest the frequent involvement of one or more TSGs located between 15q14 and 15q22. Our data show that the SRO in MM is located at 15q15 between the markers D15S1007 and ACTC. This region overlaps with sites frequently deleted in other human malignancies and represents the smallest SRO in 15q reported to date. One candidate TSG located at 15q14 ± 15 is the hRAD51 gene, which encodes a member of the RecA/ Rad51 family of proteins. However, this gene resides 4 cM proximal to our SRO. Moreover, in other cancers with 15q14 ± 15 LOH, neither hRAD51 mutations nor hypermethylation of the hRAD51 promoter were observed (Schmutte et al., 1999). To date, no bona ®de TSG has been mapped to our SRO. Mutations in the actin alpha cardiac muscle (ACTC) gene, which ¯anks the SRO identi®ed in MM, are responsible for dilated cardiomyopathy (Olson et al., 1998). To investigate whether this gene might be involved in MM, we performed RT ± PCR on normal mesothelial cells and on several MM cases displaying LOH in 15q. No dierences in expression were detected (data not shown). A recent report suggested an association between a rare connective tissue disorder, Marfan's syndrome, and MM in two aected brothers not exposed to asbestos (Bisconti et al., 2000). The ®brillin gene (FBN1), which is responsible for Marfan's syndrome, maps approximately 5-cM distal from the 15q15 SRO. However, RT ± PCR analysis revealed similar levels of expression of this gene in normal mesothelial cells and MM cases with LOH in 15q (data not shown). In conclusion, we have demonstrated that genomic losses from 15q are a common occurrence in MM and have de®ned a discrete region of deletion involving markers within 15q15. This region overlaps with sites frequently deleted in several other types of cancer and is the smallest site of recurrent 15q loss identi®ed to date in human tumors. Thus, the identi®cation of a tumor suppressor locus in 15q may be important in understanding how 15q contributes to the pathogenesis of MM and other malignancies, as well. Acknowledgments This investigation was supported by National Cancer Institute Grants CA-45745 and CA-06927, by a gift from the Local #14 Mesothelioma Fund of the International Association of Heat and Frost Insulators & Asbestos Workers in memory of Hank Vaughan and Alice Haas, and by an appropriation from the Commonwealth of Pennsylvania. 15q losses in mesothelioma A De Rienzo et al 6249 References Altomare DA, Kozak CA, Sonoda G and Testa JR. (1996). Cytogenet. Cell Genet., 74, 248 ± 251. Antman KH. (1981). Semin. Oncol., 8, 313 ± 320. Antman KH, Li FP, Osteen R and Sugarbaker DJ. (1989). Mesothelioma. J.P. Lippincott Co, Philadelphia. Attanoos RL and Gibbs AR. (1997). Histopathology, 30, 403 ± 418. Balsara BR, Bell DW, Sonoda G, De Rienzo A, du Manoir S, Jhanwar SC and Testa JR. (1999). Cancer Res., 59, 450 ± 454. Bell DW, Jhanwar SC and Testa JR. (1997). Cancer Res., 57, 4057 ± 4062. Bianchi AB, Mitsunaga SI, Cheng JQ, Klein WM, Jhanwar SC, Seizinger B, Kley N, Klein-Szanto AJ and Testa JR. (1995). Proc. Natl. Acad. Sci. USA, 92, 10854 ± 10858. Bisconti M, Bisetti A and Bidoli P. (2000). Respiration, 67, 223 ± 228. Bjorkqvist AM, Tammilehto L, Anttila S, Mattson K and Knuutila S. (1997). Br. J. Cancer, 75, 523 ± 527. Bjorkqvist AM, Wolf M, Nordling S, Tammilehto L, Knuuttila A, Kere J, Mattson K and Knuutila S. (1999). Br. J. Cancer, 81, 1111 ± 1115. Broman KW, Murray JC, Sheeld VC, White RL and Weber JL. (1998). Am. J. Hum. Genet., 63, 861 ± 869. Carbone M, Fisher S, Powers A, Pass HI and Rizzo P. (1999). J. Cell. Physiol., 180, 167 ± 172. Cheng JQ, Jhanwar SC, Klein WM, Bell DW, Lee WC, Altomare DA, Nobori T, Olopade OI, Buckler AJ and Testa JR. (1994). Cancer Res., 54, 5547 ± 5551. Cheng JQ, Lee WC, Klein MA, Cheng GZ, Jhanwar SC and Testa JR. (1999). Genes Chromosomes Cancer, 24, 238 ± 242. Collins A, Teague J, Keats BJ and Morton NE. (1996). Genomics, 36, 157 ± 162. Craighead JE and Mossman BT. (1982). N. Engl. J. Med., 306, 1446 ± 1455. De Rienzo A, Jhanwar SC and Testa JR. (2000). Genes Chromosomes Cancer, 28, 337 ± 341. Dodson MK, Hartmann LC, Cliby WA, DeLacey KA, Keeney GL, Ritland SR, Su JQ, Podratz KC and Jenkins RB. (1993). Cancer Res., 53, 4456 ± 4460. Kersemaekers AM, Kenter GG, Hermans J, Fleuren GJ and van de Vijver MJ. (1998). Int. J. Cancer, 79, 411 ± 417. Knudson AG. (1989). Cancer, 63, 1888 ± 1891. Lynch HT, Katz D and Markvicka SE. (1985). Cancer Genet. Cytogenet., 15, 25 ± 35. Mossman BT, Kamp DW and Weitzman SA. (1996). Cancer Invest., 14, 466 ± 480. Olson TM, Michels VV, Thibodeau SN, Tai YS and Keating MT. (1998). Science, 280, 750 ± 752. Pache JC, Janssen YM, Walsh ES, Quinlan TR, Zanella CL, Low RB, Taatjes DJ and Mossman BT. (1998). Am. J. Pathol., 152, 333 ± 340. Park WS, Park JY, Oh RR, Yoo NJ, Lee SH, Shin MS, Lee HK, Han S, Yoon SK, Kim SY, Choi C, Kim PJ, Oh ST and Lee JY. (2000). Cancer Res., 60, 70 ± 73. Popescu NC, Chahinian AP and DiPaolo JA. (1988). Cancer Res., 48, 142 ± 147. Schmutte C, Tombline G, Rhiem K, Sado MM, Schmutzler R, von Deimling A and Fischel R. (1999). Cancer Res., 59, 4564 ± 4569. Seemayer TA and Cavenee WK. (1989). Lab. Invest., 60, 585 ± 599. Sekido Y, Pass HI, Bader S, Mew DJ, Christman MF, Gazdar AF and Minna JD. (1995). Cancer Res., 55, 1227 ± 1231. Shivapurkar N, Virmani AK, Wistuba II, Milchgrub S, Mackay B, Minna JD and Gazdar AF. (1999). Clin. Cancer Res., 5, 17 ± 23. Stanton SE, Shin SW, Johnson BE and Meyerson M. (2000). Genes Chromosomes Cancer, 27, 323 ± 331. Taguchi T, Jhanwar SC, Siegfried JM, Keller SM and Testa JR. (1993). Cancer Res., 53, 4349 ± 4355. Tahara H, Smith AP, Gas RD, Cryns VL and Arnold A. (1996). Cancer Res., 56, 599 ± 605. Testa JR, Carbone M, Hirvonen A, Khalili K, Krynska B, Linnainmaa K, Pooley FD, Rizzo P, Rusch V and Xiao GH. (1998). Cancer Res., 58, 4505 ± 4509. Tomlinson I, Rahman N, Frayling I, Mangion J, Barfoot R, Hamoudi R, Seal S, Northover J, Thomas HJ, Neale K, Hodgson S, Talbot I, Houlston R and Stratton MR. (1999). Gastroenterology, 116, 789 ± 795. Weinberg R. (1993). Neuron, 11, 191 ± 196. Wick W, Petersen I, Schmutzler RK, Wolfarth B, Lenartz D, Bierho E, Hummerich J, Muller DJ, Stangl AP, Schramm J, Wiestler OD and von Deimling A. (1996). Oncogene, 12, 973 ± 978. Oncogene