Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Saethre–Chotzen syndrome wikipedia , lookup
Heritability of IQ wikipedia , lookup
Ridge (biology) wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
X-inactivation wikipedia , lookup
Epigenetics of diabetes Type 2 wikipedia , lookup
Gene nomenclature wikipedia , lookup
Gene desert wikipedia , lookup
Genomic imprinting wikipedia , lookup
Genetic engineering wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Genome evolution wikipedia , lookup
Gene therapy wikipedia , lookup
Medical genetics wikipedia , lookup
Biology and consumer behaviour wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Epigenetics of human development wikipedia , lookup
History of genetic engineering wikipedia , lookup
Gene expression programming wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Site-specific recombinase technology wikipedia , lookup
Gene expression profiling wikipedia , lookup
Public health genomics wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Designer baby wikipedia , lookup
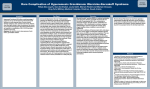
Alcohol & Alcoholism Vol. 44, No. 2, pp. 166–170, 2009 Advance Access publication 18 December 2008 doi: 10.1093/alcalc/agn101 Molecular Genetics of Alcohol-Related Brain Damage ∗ Irene Guerrini1,2, , Allan D. Thomson2 and Hugh M. Gurling2 1 Bexley Substance Misuse Service, South London and Mausdley NHS Trust, London, UK and 2 Molecular Psychiatry Laboratory, Research Department of Mental Health Sciences, Windeyer Institute of Medical Sciences, London Medical School, University College London, 46 Cleveland Street, London W1T 4JF, UK ∗ Corresponding author: Molecular Psychiatry Laboratory, Department of Mental Health Sciences, Windeyer Institute of Medical Sciences, University College London, 46 Cleveland Street, London W1T 4JF, UK. Tel: +44-1322-357940; Fax: +44-1322-357960; E-mail: [email protected] Abstract — Aims: In the scientific literature it has been repeatedly hypothesized that there is a heritable susceptibility to thiamine deficiency comparable to other hereditary metabolic disorders. The aim of this paper is to review the most recent knowledge on the genetic susceptibility to the development of alcohol-related Wernicke–Korsakoff syndrome (WKS). Methods: A literature review was carried out looking at the molecular genetics studies performed in alcohol-dependent patients affected by WKS. Results: A genetic component in the pathogenesis of WKS has been postulated since the late seventies. Since then, very few genetic studies have been carried out on candidate genes such as thiamine-dependent enzymes, alcohol-metabolizing enzymes and GABA receptors. The findings are controversial and not conclusive. Several authors reported the important role of the thiamine transporters in the pathogenesis of the thiamine deficiency disorders. Our findings on SLC19A2 and SLC19A3 suggest a potential role of these two genes in the pathophysiology of alcohol-related thiamine deficiency but further studies need to be carried out. Conclusions: The WKS may be a very complex, multifactorial disorder where the interaction of multiple genes and environment plays an important role in the pathogenesis. However, it is still plausible that megaphenic gene effects are responsible for WKS susceptibility and the thiamine transport genes are good candidates for having such a role. Further genetic studies are definitely needed to investigate the association with candidate genes or linkage with hot spot areas. INTRODUCTION Prolonged and heavy alcohol intake has been linked to cognitive deficits that vary from very mild to moderate cognitive impairment to severe amnesia. The most common neurological disorder associated with chronic alcohol abuse is Wernicke–Korsakoff syndrome (WKS). The acute phase of this syndrome called Wernicke’s encephalopathy (WE) is characterized by the classical triad of symptoms, oculo-motor abnormalities such as nystagmus and opthalmoplegia, cerebellar dysfunction or ataxia and confusion. However only 16% of patients develop the full triad of symptoms, frequently they present as simply confused or comatose (Thomson et al., 2008a, 2008b). Left untreated, the thiamine deficit can cause severe brain damage resulting in death or progression to the chronic stages of the disorder known as Korsakoff’s psychosis (KP), characterized by pronounced short-term memory impairment resulting in neuronal damage in specific brain sites (Thomson et al., 2008a, 2008b). Thiamine deficiency was first implicated as the major aetiological factor in WKS by Bowman and Alexander independently in 1939. Later, De Wardner and Lennox (1947) observed 52 malnourished prisoners of war and further established a link between thiamine deficiency and WKS in humans (Thomson et al., 2008b). Anatomical studies of the brains of WKS patients and experimental rat or mouse models of thiamine deficiency have demonstrated similar acute and chronic neuronal damage with evidence of haemorrhages, demyelinization, gliosis and neuronal loss localized to the mammillary bodies, thalamic nuclei and cerebellum with relative sparing of cerebral cortical structures (Harper et al., 2003). Postmortem (PM) studies have shown that 1.5% of all patients specifically examined for damage in the WKS areas at PM in general hospitals have the neuropathological lesions characteristic of the syndrome and that 12.5% of alcoholics were found to have the brain lesions specific to WKS (Harper et al., 1986, 2003). C SUSCEPTIBILITY TO THIAMINE DEFICIENCY IN ALCOHOLISM The importance of thiamine to the central nervous system is shown by its key role in glucose metabolism. Eighty percent of brain thiamine is in the form of thiamine diphosphate, a cofactor for three thiamine-dependent enzymes important in brain cell metabolism—α-ketoglutarate dehydrogenase complex (KGDHC), transketolase (Tk) and pyruvate dehydrogenase (PDH) enzymes. Thiamine deficiency diminishes thiamine-dependent enzyme activity, alters mitochondrial function, impairs oxidative metabolism and causes selective neuronal death (Hazell et al., 1998; Gibson and Zhang, 2002; Ke et al., 2003). In alcoholics, thiamine deficiency may result from an inadequate dietary intake, an impaired thiamine absorption in the gastrointestinal tract, a reduced liver storage and a decrease in the transformation of thiamine into its active form (Thomson, 1978; Butterworth, 1995). Experimental animal studies of the role of alcohol misuse and thiamine deficiency in the development of cognitive and neurological deficits indicate a synergy between alcohol and thiamine deficiency in the pathophysiology of the cognitive impairment (Ambrose et al., 2001; Sechi and Serra, 2007). Investigations in humans and studies in animal models have implicated a reduction in the activities of thiamine-utilizing enzymes as a marker of the metabolic basis of tissue injury due to thiamine deficiency (Butterworth et al., 1993; Heap et al., 2002). Butterworth and colleagues demonstrated significant reductions of the thiamine-dependent enzymes, pyruvate dehydrogenase complex (PDHC), α-KGDH and Tk, in autopsied cerebellar vermis samples from alcoholic patients with the clinically and neuropathologically confirmed diagnosis of WKS (Butterworth et al., 1993). In the scientific literature, it has been repeatedly hypothesized that there is a heritable susceptibility to thiamine deficiency comparable to other hereditary metabolic disorders. The The Author 2008. Published by Oxford University Press on behalf of the Medical Council on Alcohol. All rights reserved Molecular Genetics of Alcohol-Related Brain Damage CANDIDATE GENES Literature Transketolase McCool et al., 1983; Martin et al., 1995; Guerrini and Thomson, 2008 Apoe epsilon4 Muramatsu et al., 1997 GABAAbeta2 & GABAAalpha6 receptors Loh et al., 1999 ADH2*1/2*1 genotype Matsushita et al., 2000 DLST gene Matsushita et al., 2001 SLC19A2 Guerrini et al., 2005 SLC19A3 Guerrini and Thomson, 2008 OGDH (E1K ) Guerrini and Thomson, 2008 Fig. 1. Summary of candidate genes implicated in the genetic susceptibility to develop WKS. aim of this paper is to review the most recent knowledge on the genetic susceptibility to the development of alcohol-related WKS (see Fig. 1 for reference). CANDIDATE GENES Tk genes Blass and Gibson postulated that in susceptible patients the enzyme would have an abnormally low affinity for cofactor thiamine pyrophosphate (TPP) (Blass and Gibson, 1977). Changes in this enzyme function were initially identified in subjects with WKS as well as in a small minority of alcohol misusers and chronically malnourished individuals. The Tk extracted from cultured fibroblasts of WKP patients show decreased affinity for TPP (Blass and Gibson, 1977). A study of cultured fibroblasts from various groups of patients that included cases of WKS, familial chronic alcoholic males, their sons and controls also showed decreased affinity of Tk for TPP (Mukherjee et al., 1987). Martin and co-workers investigated the interactions of Tk, derived from human fibroblasts, lymphoblasts and various brain regions, with its cofactor, TPP. They found that the rate of TPP-dependent formation of active Tk holoenzyme varied 6- and 4-fold, respectively, in the different brain regions examined (Martin et al., 1994). Heap and co-workers investigated the affinity of erythrocyte Tk for its cofactor in alcohol abusers with cognitive impairment and have shown that a subgroup of these patients has altered Tk-binding parameters despite adequate nutrition and supplementation with vitamin preparations (Heap et al., 2002). Previous studies of red cell Tk in a study by Kaczmarek and Nixon (1983) using isoelectric focusing identified variations of the Tk isoenzyme pattern. These authors and later Kaufmann and colleagues were able to distinguish five different isoenzyme patterns, one variant of which was preferentially found in patients with WKP (Kaczmarek and Nixon, 1983; Nixon et al., 1984; Kaufmann et al., 1987). Nucleotide sequence of the Tk-coding sequence from two WKP and two non-alcoholic controls was compared by reverse transcription of total cellular fibroblast RNA followed by PCR 167 amplification and direct sequencing with specific Tk primers (McCool et al., 1993). Although various nucleotide variations were observed, none of these changes corresponded to alterations in the amino acids thought to be important in the protein functions. The sequencing of Tk in just two cases of WKS by McCool and colleagues was not a sufficient test of the hypothesis (McCool et al., 1993). A novel transketolase-related gene (TKR), located between the green colour vision pigment and the ABP-280 filamin gene, has been isolated at Xq28 (Coy et al., 1996). Coy et al. found several differences in the protein sequence between human Tk and TKR, such as the acquisition of a tissue-specific spliced exon, and two deletions in the TKR gene. The deletion of 38amino acids leads to the lack of a region important for TPP binding and it is likely that this deletion results in a decrease in the affinity of TKR for TPP (Coy et al., 1996). The PDHC The PDHC consists of three enzymes: (a) pyruvate decarboxylase, E1 (b) dihydrolipoyl transacetylase, E2 and (c) dihyrolipoyl dehydrogenase, E3. The PDH and the α-ketoglutarate together with Tk were shown to have reduced activity in PM samples from frontal cortex and cerebellum of alcoholic patients with neuropathologically confirmed WKS (Butterworth et al., 1993). Both PDH and α-keto complexes are located within the mitochondria and catalyze the oxidative decarboxylation of α-keto acids in the citric acid cycle. All four genes are candidates for increasing genetic susceptibility to WKS. The α-KGDHC α-KGDHC is essential for the cellular production of reducing equivalents (NADH) and in maintaining the mitochondrial redox state of the brain (Gibson et al., 2000). The genes for the enzymes of three composite subunits have been cloned and sequenced: α-KGDH (E1K) also designated (OGDH) on chromosome 7p (Koike, 1995), dihydrolipoyl succinyltransferase (DLST/E2K) on chromosome 14 (Nakano et al., 2002) and dihydrolipoyl dehydrogenase (E3) on chromosome 7p. KGDHC genes are thought to be unique in comparison to other thiamine-dependent enzyme genes because they do not depend on TPP for their regulation. The KGDHC enzyme is constituted of multiple copies of each of its subunits E1K (12 dimers), E3 (6 dimers) that are packed around the edges and face the E2 octahedral core (24 subunits) (Perham, 1991; Berg and de Kok, 1997). The three subunits E1K and E2K are unique to KGDHC while E3 is also found in PDHC and the branched chain dehydrogenase complex (BCDHC). Research into the genetics of E2K has revealed no associations between the E2K gene and alcoholic WKS patients (Matsushita et al., 2001). The thiamine-binding capacity of E1K or 2-oxogluterate dehydrogenase (OGDH) that catalyzes the oxidative decarboxylation responsible for converting 2-oxogluterate to succinyl-CoA and CO2 makes E1K or OGDH a good target of investigation in the aetiology of WKS. Thiamine deficiency is responsible for a 40% reduction in α-KGDH activity as demonstrated in rats with pyrithiamine induced thiamine deficiency (Munujos et al., 1996). OGDH/E1K is responsible for the catalysis of the 168 Guerrini et al. conversion of α-ketogluterate to succinyl coenzyme A, a critical step in the Kreb’s tricarboxylic acid cycle, a large reduction in which leads to compromised cerebral energy metabolism and focal accumulation of potentially toxic lactate in the thalamus, midbrain, hypothalamus and colliculi. The thiamine transporters In humans, thiamine cannot be synthesized and must therefore be obtained from exogenous sources, through absorption in the intestine. Healthy adults require 1.4 mg of thiamine daily; requirements are higher in children, in pregnancy, in alcoholics and in critically ill patients. The cellular transport of thiamine is mediated by specific carriers, recently identified and characterized: the thiamine transporter-1 and transporter-2, respectively, the products of the SLC19A2 and SLC19A3 genes (Ganapathy et al., 2003). Gene expression studies have shown that the thiamine transporters are well expressed in several tissues such the intestine, placenta, kidneys and brain (Guerrini et al., 2005). The SLC19A2 gene encodes the human thiamine transporter protein that is made up of 497 amino acids and is predicted to have 12 transmembrane domains responsible for importing thiamine into the cell for utilization by thiamine-dependent enzymes such as the 2-OGDH complex. Recently, Diaz and colleagues (1999) mapped the high affinity thiamine transporter gene to chromosome 1q23.2–q23.3 (Diaz et al., 1999; Fleming et al., 1999, 2001). The SLC19A2 gene was first identified in a group of Iranian families affected by a thiamineresponsive megaloblastic anaemia syndrome (TRMA), an autosomal recessive disorder characterized by diabetes mellitus, megaloblastic anaemia and sensorineural deafness (Diaz et al., 1999). The SLC19A2 gene is expressed ubiquitously in human tissues and consists of six exons spanning ∼22.5 kb. The promoter region has been recently characterized (Reidling et al., 2002). Several functional mutations have been characterized in this gene including 10 prematurely truncated mutants resulting from point mutation, deletion or insertion of nucleotides (Fleming et al., 1999). The SLC19A3 is a second thiamine transporter that has been recently identified and mapped to chromosome 2q37. The murine SLC19A3 gene has also been mapped to chromosome 1 in a seizure susceptibility locus in the DBA/2J mouse strain (Eudy et al., 2000; Rajgopal et al., 2001). In 2005, Zeng and colleagues identified two missense mutations in the SLC19A3 in a group of highly inbred families affected by the biotinresponsive basal ganglia disease (Zeng et al., 2005). Our laboratory at University College London, UK, screened the high affinity thiamine transporter gene SLC19A2 on chromosome 1q23.2–q23.3 and the low affinity thiamine transporter gene SLC19A3 on chromosome 2q36.3 in a group of alcoholics affected by WKS and in super-normal controls. We identified several genetic variants in the SLC19A2 (exon 6, 3 UTR region) and in the SLC19A3 (promoter and intron 1) (Guerrini et al., 2005). These genetic variants are not described as common polymorphisms in published databases. We found two of the changes in the 3 untranslated region of the thiamine transporter gene that can potentially affect gene expression. Further case-control studies are necessary to confirm or disconfirm our findings. Other genes Several mechanisms have been implicated in the pathogenesis of thiamine deficiency such as oxidative stress, glutamatemediated excitotoxicity and focal lactic acidosis. Hazell and colleagues extensively studied the role of glutamate neurotoxicity triggered by thiamine deficiency. Their findings showed that the glutamate transporter (GLAST) gene is down regulated in astrocytes under conditions of thiamine deficiency by inducing increased phosphorylation of GLAST. These findings support the hypothesis that glutamate accumulation and toxicity are important factors in the degeneration of selective brain regions under conditions involving thiamine deficiency such as WKS (Hazell et al., 1998). The role of the GABAA receptor cluster on chromosome 5q33 was investigated by Loh and colleagues (1999) in a group of Scottish uncomplicated, alcoholics affected by KP and normal controls (Loh et al., 1999). The authors showed a significant association between the alcohol-dependent subjects with KP and the BanI RFLP (P = 0.039) at the GABAA beta2 (GABRB2) receptor subunit gene and the AlwNI RFLP (P = 0.003) at the GABAA alpha6 (GABRA6) receptor gene. Haplotype analysis also provided evidence of association when all alcohol-dependent subjects (P = 0.013) and the subjects with KP (P = 0.007) were compared with controls (Loh et al., 1999). Muramatsu and co-workers analysed the role of the ApoE epsilon 4 allelle in the pathogenesis of WKS in a group of Japanese alcoholics with WKS (Muramatsu et al., 1997). This study showed that the frequency of ApoE epsilon 4 allele was significantly higher in the patients with global deficits, suggesting the involvement of this allele in the intellectual decline of WKS. In contrast, distributions of other two markers, alpha 1-antichymotrypsin and presenilin-1, did not differ between the group of Korsakoff patients with preserved intellectual function other than amnesia and those with global intellectual deficits (Muramatsu et al., 1997). CONCLUSIONS A genetic component in the pathogenesis of WKS has been postulated since the late seventies (Blass and Gibson, 1977). Since then, very few genetic studies have been carried out on candidate genes such as thiamine-dependent enzymes (Matsushita et al., 2001), alcohol-metabolizing enzymes (Matsushita et al., 2000) and GABA receptors (Loh et al., 1999). The findings are controversial and not conclusive. Several authors reported the important role of the thiamine transporters in the pathogenesis of the thiamine deficiency disorders. Our findings on SLC19A2 and SLC19A3 suggest a potential role of these two genes in the pathophysiology of alcoholrelated thiamine deficiency but further studies need to be carried out. The WKS may be a very complex, multifactorial disorder where the interaction of multiple genes and environment play an important role in the pathogenesis (Fig. 2). However, it is still plausible that megaphenic gene effects are responsible for WKS susceptibility and the thiamine transport genes are good candidates for having such a role. Further genetic studies are definitely needed to investigate the association with candidate genes or linkage with hot spot areas. Molecular Genetics of Alcohol-Related Brain Damage 169 Fig. 2. Wernicke–Korsakoff syndrome—a pathogenetic model. Identifying genes that predispose development of alcoholrelated brain damage would ultimately allow clinicians to early detect individuals potentially at risk of thiamine deficiency and treat them properly before the development of the disease. REFERENCES Ambrose ML, Bowden SC, Whelan G. (2001) Thiamine treatment and working memory function of alcohol-dependent people: preliminary findings. Alcohol Clin Exp Res 25:112–6. Berg A, de Kok A. (1997) 2-Oxo acid dehydrogenase multienzyme complexes. The central role of the lipoyl domain. Biol Chem 378:617–34. Blass JP, Gibson GE. (1977) Abnormality of a thiamine-requiring enzyme in patients with Wernicke–Korsakoff syndrome. N Engl J Med 297:1367–70. Butterworth RF. (1995) Pathophysiology of alcoholic brain damage: synergistic effects of ethanol, thiamine deficiency and alcoholic liver disease. Metab Brain Dis 10:1–8. Butterworth RF, Kril JJ, Harper CG. (1993) Thiamine-dependent enzyme changes in the brains of alcoholics: relationship to the Wernicke–Korsakoff syndrome. Alcohol Clin Exp Res 17: 1084–8. Coy JF, Dubel S, Kioschis P et al. (1996) Molecular cloning of tissuespecific transcripts of a transketolase-related gene: implications for the evolution of new vertebrate genes. Genomics 32:309–16. De Wardener HE, Lennox B. (1947) Cerebral beriberi (Wernicke’s Encephalopathy): review of 52 cases in a Singapore prisoner-ofwar hospital. Lancet 1:11–17. Diaz GA, Banikazemi M, Oishi K et al. (1999) Mutations in a new gene encoding a thiamine transporter cause thiamine- responsive megaloblastic anaemia syndrome. Nat Genet 22:309–12. Eudy JD, Spiegelstein O, Barber RC et al. (2000) Identification and characterization of the human and mouse SLC19A3 gene: a novel member of the reduced folate family of micronutrient transporter genes. Mol Genet Metab 71:581–90. Fleming JC, Steinkamp MP, Kawatsuji R et al. (2001) Characterization of a murine high-affinity thiamine transporter, Slc19a2. Mol Genet Metab 74:273–80. Fleming JC, Tartaglini E, Steinkamp MP et al. (1999) The gene mutated in thiamine-responsive anaemia with diabetes and deafness (TRMA) encodes a functional thiamine transporter. Nat Genet 22:305–8. Ganapathy V, Smith SB, Prasad PD. (2003) SLC19: the folate/ thiamine transporter family. Pflugers Arch 6:6. Gibson GE, Park LC, Sheu KF et al. (2000) The alpha-ketoglutarate dehydrogenase complex in neurodegeneration. Neurochem Int 36:97–112. Gibson GE, Zhang H. (2002) Interactions of oxidative stress with thiamine homeostasis promote neurodegeneration. Neurochem Int 40:493–504. Guerrini I, Thomson A (2005) The genetics susceptibility to WernickeKorsakoff syndrome in alcoholism. Alcohol Alcohol 40(Suppl. 1):16–7. Guerrini I, Thomson A. (2008) The genetics of alcohol-related brain damage: from brain specimen to association studies. Alc Clin Exp Res 21:203A. Guerrini I, Thomson AD, Cook CC et al. (2005) Direct genomic PCR sequencing of the high affinity thiamine transporter (SLC19A2) gene identifies three genetic variants in Wernicke–Korsakoff syndrome (WKS). Am J Med Genet B (Neuropsychiatr Genet) 137:17– 9. Harper C, Dixon G, Sheedy D et al. (2003) Neuropathological alterations in alcoholic brains. Studies arising from the New South Wales Tissue Resource Centre. Prog Neuropsychopharmacol Biol Psychiatry 27:951–61. Harper CG, Giles M, Finlay-Jones R. (1986) Clinical signs in the Wernicke-Korsakoff complex: a retrospective analysis of 131 cases diagnosed at necropsy. J Neurol Neurosurg Psychiatry 49:341–5. Hazell AS, Todd KG, Butterworth RF. (1998) Mechanisms of neuronal cell death in Wernicke’s encephalopathy. Metab Brain Dis 13:97– 122. Heap LC, Pratt OE, Ward RJ et al. (2002) Individual susceptibility to Wernicke–Korsakoff syndrome and alcoholism-induced cognitive deficit: impaired thiamine utilization found in alcoholics and alcohol abusers. Psychiatr Genet 12:217–24. Kaczmarek MJ, Nixon PF. (1983) Variants of transketolase from human erythrocytes. Clin Chim Acta 130:349–56. Kaufmann A, Uhlhaas S, Friedl W et al. (1987) Human erythrocyte transketolase: no evidence for variants. Clin Chim Acta 162(2):215– 9. 170 Guerrini et al. Ke ZJ, DeGiorgio LA, Volpe BT et al. (2003) Reversal of thiamine deficiency-induced neurodegeneration. J Neuropathol Exp Neurol 62:195–207. Koike K. (1995) The gene encoding human 2-oxoglutarate dehydrogenase: structural organization and mapping to chromosome 7p13– p14. Gene 159:261–6. Loh EW, Smith I, Murray R et al. (1999) Association between variants at the GABAAbeta2, GABAAalpha6 and GABAAgamma2 gene cluster and alcohol dependence in a Scottish population. Mol Psychiatry 4:539–44. Martin PR, Pekovich SR, McCool BA et al. (1994) Thiamine utilization in the pathogenesis of alcohol-induced brain damage. Alcohol Alcohol Suppl 2:273–9. Matsushita S, Arai H, Yuzuriha T et al. (2001) No association between DLST gene and Alzheimer’s disease or Wernicke–Korsakoff syndrome. Neurobiol Aging 22:569–74. Matsushita S, Kato M, Muramatsu T et al. (2000) Alcohol and aldehyde dehydrogenase genotypes in Korsakoff syndrome. Alcohol Clin Exp Res 24:337–40. McCool BA, Plonk SG, Martin PR et al. (1993) Cloning of human transketolase cDNAs and comparison of the nucleotide sequence of the coding region in Wernicke–Korsakoff and non-Wernicke– Korsakoff individuals. J Biol Chem 268:1397–404. Mukherjee AB, Svoronos S, Ghazanfari A et al. (1987) Transketolase abnormality in cultured fibroblasts from familial chronic alcoholic men and their male offspring. J Clin Invest 79:1039–43. Munujos P, Coll-Canti J, Beleta J et al. (1996) Brain pyruvate oxidation in experimental thiamin-deficiency encephalopathy. Clin Chim Acta 255:13–25. Muramatsu T, Kato M, Matsui T et al. (1997) Apolipoprotein E epsilon 4 allele distribution in Wernicke–Korsakoff syndrome with or without global intellectual deficits. J Neural Transm 104:913–20. Nakano K, Tanabe M, Nakagawa S et al. (2002) Isolation and sequence analysis of the rat dihydrolipoamidesuccinyltransferase gene. DNA Seq 13:363–7. Nixon PF, Kaczmarek MJ, Tate J et al. (1984) An erythrocyte transketolase isoenzyme pattern associated with the Wernicke–Korsakoff syndrome. Eur J Clin Invest 14:278–81. Perham RN. (1991) Domains, motifs, and linkers in 2-oxo acid dehydrogenase multienzyme complexes: a paradigm in the design of a multifunctional protein. Biochemistry 30:8501– 12. Rajgopal A, Edmondnson A, Goldman ID et al. (2001) SLC19A3 encodes a second thiamine transporter ThTr2. Biochim Biophys Acta 1537:175–8. Reidling JC, Subramanian VS, Dudeja PK et al. (2002) Expression and promoter analysis of SLC19A2 in the human intestine. Biochim Biophys Acta 1561:180–7. Sechi G, Serra A. (2007) Wernicke’s encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol 6:442–55. Thomson AD. (1978) Alcohol and nutrition. Clin Endocrinol Metab 7:405–28. Thomson AD, Cook CC, Guerrini I et al. (2008a) Wernicke’s encephalopathy revisited. Translation of the case history section of the original manuscript by Carl Wernicke ‘Lehrbuch der Gehirnkrankheiten fur Aerzte and Studirende’ (1881) with a commentary. Alcohol Alcohol 43:174–9. Thomson AD, Cook CC, Guerrini I et al. (2008b) Wernicke’s encephalopathy: ‘plus ca change, plus c’est la meme chose’. Alcohol Alcohol 43:180–6. Zeng WQ, Al-Yamani E, Acierno JS Jr et al. (2005) Biotin-responsive basal ganglia disease maps to 2q36.3 and is due to mutations in SLC19A3. Am J Hum Genet 77:16–26.