Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Hedgehog signaling pathway wikipedia , lookup
Purinergic signalling wikipedia , lookup
Programmed cell death wikipedia , lookup
Lipid signaling wikipedia , lookup
Cannabinoid receptor type 1 wikipedia , lookup
Leukotriene B4 receptor 2 wikipedia , lookup
Biochemical cascade wikipedia , lookup
Signal transduction wikipedia , lookup
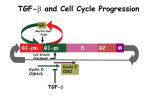
Transforming Growth Factor-s and Vascular Disorders Alex Bobik Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 Abstract—Transforming growth factor- (TGF-) superfamily members, TGF- and bone morphogenetic proteins (BMPs), are potent regulatory cytokines with diverse functions on vascular cells. They signal through heteromeric type I and II receptor complexes activating Smad-dependent and Smad-independent signals, which regulate proliferation, differentiation, and survival. They are potent regulators of vascular development and vessel remodeling and play key roles in atherosclerosis and restenosis, regulating endothelial, smooth muscle cell, macrophage, T cell, and probably vascular calcifying cell responses. In atherosclerosis, TGF- regulates lesion phenotype by controlling T-cell responses and stimulating smooth muscle cells to produce collagen. It contributes to restenosis by augmenting neointimal cell proliferation and collagen accumulation. Defective TGF- signaling in endothelial cells attributable to mutations in endoglin or the type I receptor ALK-1 leads to hereditary hemorrhagic telangiectasia, whereas defective BMP signaling attributable to mutations in the BMP receptor II has been associated with development of primary pulmonary hypertension. The development of mouse models with either cell type–specific or general inactivation of TGF-/BMP signaling has started to reveal the importance of the regulatory network of TGF-/BMP pathways in vivo and their significance for atherosclerosis, hereditary hemorrhagic telangiectasia, and primary pulmonary hypertension. This review highlights recent findings that have advanced our understanding of the roles of TGF- superfamily members in regulating vascular cell responses and provides likely avenues for future research that may lead to novel pharmacological therapies for the treatment or prevention of vascular disorders. (Arterioscler Thromb Vasc Biol. 2006;26:1712-1720.) Key Words: TGF- 䡲 BMP 䡲 signaling 䡲 vascular cells 䡲 atherosclerosis 䡲 restenosis 䡲 hereditary hemorrhagic telangiectasia 䡲 pulmonary hypertension he transforming growth factor- (TGF-) superfamily is composed of many multifunctional cytokines, including TGF-s, bone morphogenetic proteins (BMPs), activins, inhibins, and mycostatin. They participate in a wide range of processes, from tissue differentiation during development through to regulation of mesenchymal and immune cell functions. Two members of the TGF- superfamily, TGF- and BMPs, have been the most extensively studied members in the vasculature, affecting key cell functions and have been implicated in vascular disorders such as atherosclerosis, pulmonary hypertension, hereditary hemorrhagic telangiectasia (HHT), and restenosis. TGF- isoform TGF-, TGF-2, and TGF-3, as well as several BMPs, in particular BMP-2, BMP-4, BMP-6, and BMP-7, are expressed by cells in the vessel wall and are capable of modulating vascular development and remodeling by altering cell differentiation, proliferation, migration, extracellular matrix production, and the activities of immune cells. This review discusses the vascular effects of these TGF- superfamily members, their signaling systems, and how their actions in multiple cell types including those of the immune system regulate processes involved in the development of T atherosclerosis, restenosis, vascular development, and remodeling associated with diseases such as HHT and primary pulmonary hypertension (PPH). TGF- Superfamily Members and Effects on Vascular Cells TGF- isoforms and several BMPs, BMP-2, BMP-4, BMP-6, and BMP-7 are expressed by ⱖ1 vascular cells, endothelial cells, vascular smooth muscle cells (VSMCs), macrophages, and various types of lymphocytes. TGF- isoforms are produced as inactive dimeric latent precursors and are subsequently processed extracellularly to yield active receptor binding ligands. In the vessel wall, inactive TGF- can be activated via the cooperation between the mannose-6phosphate/insulin-like growth factor II receptor and the urokinase-type plasminogen activator receptor, plasmin, thrombospondin, and furin-like proprotein convertases; the latter are responsible for TGF- activation after arterial injury.1 In contrast, BMPs are secreted in an active form and regulated through reversible interactions with extracellular antagonists, including noggin, chordin, and DAN.2 These interactions determine the bioavailability of different TGF- Original received January 3, 2006; final version accepted April 24, 2006. From the Cell Biology Laboratory, Baker Heart Research Institute, Melbourne, Australia. Correspondence to Professor Alexander Bobik, Cell Biology Laboratory, Baker Heart Research Institute, PO Box 6492, St Kilda Rd Central, Melbourne, Victoria 8008, Australia. E-mail [email protected] © 2006 American Heart Association, Inc. Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org 1712 DOI: 10.1161/01.ATV.0000225287.20034.2c Bobik Transforming Growth Factor-s and Vascular Disorders 1713 Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 Figure 1. TGF- and BMP transduce signals through Smad-dependent and Smad-independent pathways in vascular cells. Dimeric TGF- becomes active after dissociation from its complex of the latency-associated protein (LAP) and latent TGF- binding protein-1 (LTBP), whereas BMP free of antagonists activate their respective tetrameric receptor complexes with or without endoglin. Subsequently, the type I receptors (ALK-5 or ALK-1 for TGF- and ALK-1, ALK-2, ALK-3, and ALK-6 for BMP) phosphorylate respective receptor-activated Smads (R-Smads; -1,-2,-3,-5, and -8), which translocate to the nucleus as a trimeric complex with Smad4. The complex interacts with other transcription factors (TF), coactivators, or corepressors and the Smad binding element (SBE). When complexed with transcriptional coactivators (eg, CBP/p300) target genes are activated), and when complexed with corepressors (eg, Sno), transcription is repressed. Smad-independent signals generated by TGF-/BMPs are boxed and include ERK1/2, p38MAPK, JNK, and phosphatidylinositol 3-kinase (PI3K). s/BMPs for binding to their receptors. Endothelial cells, smooth muscle cells, mesenchymal cells, macrophages, and lymphocytes respond to these TGF- family members by their interaction with a heteromeric complex of type I and type II transmembrane serine/threonine kinase receptors. Multiple type I and II receptors have been identified that exhibit specificities in signaling mediated by TGF- isoforms or BMPs (Figure 1). TGF- isoforms, BMP-6, and BMP-7 have a high affinity for the type II receptors, and on binding, a type I receptor is recruited, forming a heteromeric complex resulting in phosphorylation of the type I receptor in a conserved region, the GS domain, changing its conformation; BMP-2 and BMP-4 exhibit a higher affinity for the type I receptor but also signal through the heteromeric type I/type II complex.3 Signal propagation to the nucleus then occurs by the type I receptor phosphorylating Smad proteins, the major nuclear effectors for TGF- receptors.4 There are 3 distinct types of Smads: receptor regulated, common mediator Smads, and inhibitory Smads. Smad1, Smad2, Smad3, Smad5, and Smad8 are receptor regulated and phosphorylated at their extreme C-terminal serines followed by interaction with the common mediator Smad, Smad4, and translocation to the nucleus. Inhibitory Smads, Smad6, and Smad7 compete with receptor-activated Smads for receptor interaction and recruit ubiquitin ligases or phosphatases to activated receptors, promoting their degradation or dephosphorylation.5 TGF- and BMPs exert multiple effects on endothelial cells. TGF- exerts bifunctional effects on cell proliferation, stimulating proliferation and migration at low concentrations, whereas at higher concentrations, it inhibits these processes. It regulates the activation state of endothelial cells via 2 type I receptors, ALK-5, and ALK-1.6 The TGF-/ALK-1 pathway stimulates endothelial cell proliferation and migration, whereas the TGF-/ALK-5 pathway inhibits these processes. Constitutively active forms of ALK-1 and ALK-5 initiate differential patterns of gene expression.7 ALK-1 stimulates the expression of Id-1, an inhibitor of basic helix-loop-helix proteins that promotes endothelial cell proliferation, migration, and tube formation,8 whereas ALK-5 induces expression of plasminogen activator inhibitor-1, a negative regulator of endothelial cell migration and angiogenesis. When ALK-5 kinase is inhibited by SB-431542, TGF-1 only stimulates endothelial cell proliferation.9 Studies on signaling mechanisms initiated by ALK-1 and ALK-5 indicate a complex interaction between the receptors. ALK-5 deficiency not only impairs TGF-/ALK-5 signaling but also reduces TGF-/ 1714 Arterioscler Thromb Vasc Biol. August 2006 Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 ALK-1 responses, suggesting that ALK-5 is essential for efficient ALK-1 activation and recruitment into a TGF- receptor complex.10 ALK-1 not only induces responses opposite to ALK-5 but also antagonizes ALK-5/Smad3 signaling. This dual receptor system in endothelial cells provides an intricate mechanism for switching between different TGF-– induced responses. When ALK-5 is inhibited by SB-431542, TGF-1 also affects vascular permeability by upregulating the expression of Claudin-5, an endothelial cell–specific component of tight junctions,9 and inhibits the expression of adhesion molecules. The TGF- type III receptor endoglin is also important for TGF- responses by endothelial cells. Both the extracellular and intracellular domains of endoglin interact with TR-II and ALK-5 and its cytoplasmic domain, which is phosphorylated by ALK-5 and TR-II.11 Deletion of endoglin from endothelial cells potentiates the inhibitory effects of TGF- on endothelial cell migration and growth, suggesting that it is a negative regulator of TGF-/ALK-5 signaling. Endoglin stimulates TGF-/ALK-1 signaling and indirectly inhibits TGF-/ALK-5 signaling. It also stimulates the expression of endothelial NO. In addition to activating genes in endothelial cells, TGF- also represses gene expression, particularly genes that promote inflammation, interleukin-6 (IL-6), monocyte chemoattractant protein-1, and granulocyte– colony-stimulating factor.12 Such effects may be tissue specific (see below). Although VSMCs express multiple type I receptors as well as the type II TGF- receptor,13 most of the effects of TGF- on VSMC function appear to be mediated via the ALK-5/TR-II complex. Subsequent downstream signaling is complex, not only involving Smad2/3 but also kinases such as p38 mitogenactivated protein kinase (MAPK), p42/p44, and JNK as well as transcription factors, which are all dependent on ALK-5 (Figure 1).14 TGF- is a potent vascular smooth muscle differentiating factor, increasing the expression of ␣-smooth muscle actin, smooth muscle myosin, and calponin. At low concentrations, it stimulates proliferation by inducing platelet-derived growth factor (PDGF)–AA. TGF-1 can also attenuate VSMC activation by opposing the effects of mitogenic growth factors, proinflammatory cytokines, and genes that affect vascular remodeling. Both Smad-dependent and Smad-independent mechanisms contribute to its ability to inhibit proliferation,15 whereas its ability to activate genes such as ␣2 type I collagen and inhibitor of metalloproteinase-1 is Smad3 dependent. TGF-/ Smad3-dependent signaling also prevents cytokine-mediated activation of smooth muscle cells by Smad3 binding directly to the CCAT/enhancer-binding protein- and also reducing the expression of CCAT/enhancer-binding protein-␦.16 Other signaling cascades are also important, for example, increases in plasminogen activator inhibitor type I gene expression by TGF-1 is dependent on transactivation of the epidermal growth factor receptor and c-Src activation.17 Increases in fibronectin expression and the synthesis of vascular endothelial growth factor are also Smad independent and regulated via disabled-2 association with TAK1, leading to JNK activation and p38MAPK activation, respectively.18 Mechanistically, other effects of TGF-1 on VSMCs, such as stimulating proteoglycan synthesis, are yet to be defined. TGF-1 also exerts important effects on immune cells. Macrophages produce and are highly responsive to TGF-1. TGF- can activate and also deactivate these cells depending on the local cytokine environment.19 Signaling cascades appear similar to those in VSMCs. TGF-1 promotes monocyte adhesion to type IV collagen, laminin, and fibronectin20 and stimulates monocyte chemotaxis via Smad3,21 increasing expression of receptors for multiple chemokines.22 TGF- may also potentiate inflammation by inducing the secretion of IL-1 and IL6.19,23 It protects macrophages from apoptosis by stimulating extracellular-signal regulated kinase (ERK) and attenuates macrophage foam cell formation by downregulating the expression of CD36; it also increases cholesterol efflux, the expression of the ATP-binding cassette transporter-1,24 and inhibits lipoprotein lipase expression via mechanisms involving Sp1-binding sites.25 TGF- exerts anti-inflammatory effects by attenuating macrophage activation. It reduces cytokine-stimulated inducible NO synthase expression in a Smad3-dependent manner by recruiting the limited amounts of p300/CREB-binding protein from nuclear factor B and AP-1 to Smad3.26 It also promotes inducible NO synthase protein degradation27 and inhibits cytokinemediated increases in metalloelastase and the expression of chemokines KC and MIP-2 by destabilizing their mRNAs via p38MAPK-dependent mechanism.28 TGF- affects T-cell proliferation, differentiation, and survival. This important function of TGF- is exemplified in vivo, in which animals expressing the dominant-negative TGF- type II receptor specifically in T cells develop severe autoimmunity characterized by uncontrolled T-cell activation.29 Similarly, blockade of TGF-/Smad signaling in T cells by overexpression of Smad7 also enhances inflammation.30 Like the other vascular cell types, in lymphocytes, TGF- signals by recruiting type II and type I (ALK-5) receptors followed by phosphorylation of receptor-regulated Smads. Endoglin is also expressed on T-cells and acts to counteract TGF-–mediated suppression. TGF- inhibits proliferation by inhibiting IL-2 expression, c-myc, and cyclins D2 and E. Inhibition is influenced by differentiation state and is most apparent in naive cells; it has minimal effects on activated T cells, which express low amounts of the type II receptor. Upregulation of the type II receptor by IL-10 treatment restores TGF- responsiveness on activated T cells.31 Other effects include inhibition of Th1 and Th2 differentiation,32 the latter via GATA3, inhibition of interferon-␥ (IFN-␥) production, upregulation of tristetraprolin, a protein involved in tumor necrosis factor-␣ degradation, inhibition of IL-2 production, and T-cell proliferation.33 TGF- inhibits Th1 development in part via suppression of T-bet, an IFN-␥–induced transcription factor that promotes Th1 differentiation (Figure 2).34 TGF- also inhibits Fas ligand expression and subsequent activation-induced cell death by downregulating c-myc. Other effects of TGF- include inhibition of CD1d expression on dendritic cells;35 CD1d is essential for lipid antigen recognition by NKT cells. TGF- also influences CD4⫹CD25⫹ T-cell development by regulating the expression of Foxp3, a transcription factor essential for their generation and function.36 BMPs BMP-2, BMP-4, BMP-6, and BMP-7 also exert important effects on endothelial and smooth muscle cells. Bobik Transforming Growth Factor-s and Vascular Disorders Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 Figure 2. TGF- and T-cell responses. TGF- inhibits T-cell proliferation by inhibiting IL-2 production and suppressing c-myc, cyclins, and cyclin-dependent kinase 4 (CDK4). It inhibits differentiation of Th1 and Th2 cells by suppressing the expression or function of T-bet and GATA3 but stimulates expression of Foxp3, increasing the suppressive activities of regulatory CD4⫹CD25⫹ T cells. TGF- can also prevent T-cell activation–induced apoptosis by inhibiting c-myc. Dysregulation of TGF- signaling in T cells increases atherosclerosis severity. Adapted from Li et al.34 BMPs interact with 3 type 2 receptors, BMP receptor II (BMPR-II), ActR-II, and ActR-IIB, to activate ⱖ1 of 4 different type I receptors, ALK-1, ALK-2, ALK-3, and ALK-6, which then signal in a manner similar to TGF- using specific receptor-regulated Smads (Figure 1). BMP-2 stimulates endothelial cell migration and angiogenesis via Id1 and the p38MAPK pathway,37 whereas BMP-4 stimulates production of reactive oxygen species and monocyte adhesion.38 In some endothelial cell types, BMP-4 induces apoptosis.39 BMPs are expressed by endothelial cells and influence smooth muscle cell phenotype. BMP-2 expression by endothelial cells is regulated via a hydrogen peroxide/nuclear factor B pathway, activated by proinflammatory cytokines and high pressure; oscillatory shear stress regulates BMP-4 expression. The effects of BMPs on VSMCs include inhibition of proliferation and modulation of smooth muscle cell differentiation markers; BMP-2 decreases, whereas BMP-7 increases expression of smooth muscle cell markers.40 In pulmonary VSMCs, BMP-4 activates Smad1, p38MAPK, and ERK1/2 pathways.41 Inhibition of proliferation by BMP-4 is dependent on the Smad1 pathway and elevations in p21WAF1; activation of Smad1 also downregulates the antiapoptotic protein Bcl-2, making these cells more sensitive to apoptosis. In contrast, p38MAPK/ERK promotes proliferation and is antiapoptotic. BMP-2 also stimulates smooth muscle cell migration by undefined mechanisms. TGF- and Atherogenesis TGF- and receptors are abundantly expressed by smooth muscle cells, macrophages, and T cells in human atherosclerotic lesions during development of fatty streaks and subsequent atheroma.42 Because TGF- stimulates leukocyte chemotaxis21 and proteoglycan production by smooth muscle cells, it is possible that TGF- contributes to early macrophage migration and lipid accumulation. TGF- appears to determine the extent to which developing atherosclerotic 1715 lesions are stabilized by a collagen-rich fibrous cap. Smooth muscle cells in stable lesions express greater amounts of TGF- than unstable lesions.43 Smooth muscle cells from lesions dominantly express the type I receptor, whereas smooth muscle cells from normal vessels dominantly express the type II receptor.44 Cells dominantly expressing type I receptors respond to TGF- by producing copious amounts of extracellular matrix. Smooth muscle cells within the fibrous cap of atherosclerotic lesions and fibrofatty lesions also appear to differ in their responsiveness to TGF-. Smooth muscle cells within fibrous plaques express Smad proteins, which are essential for TGF-–mediated increases in collagen gene expression, but in macrophage-rich fibrofatty lesions, smooth muscle cells do not express Smad proteins, suggesting that their ability to produce collagen in response to TGF- is impaired.45 In fibrofatty lesions, IFN-␥ produced by T cells and macrophages can also contribute to reduced collagen levels by inhibiting collagen production.46 Treatment of apolipoprotein E– deficient (apoE⫺/⫺) mice with an anti–TGF- neutralizing antibody reduces collagen by 50%, also supporting an important role for TGF- in collagen production in lesions.47 This was associated with reduced Smad2 phosphorylation and an increase in lesion size but no change in the smooth muscle cell numbers. Inhibiting TGF- with a recombinant soluble TGF- receptor fusion protein was associated not only with increased inflammation but also intraplaque hemorrhage.48 At least a component of the inflammatory response to TGF- depletion appears because of T-lymphocyte deregulation; adventitial lymphocytes increase in number after treatment with the neutralizing antibody.47 Furthermore, disruption of TGF- signaling specifically in T cells also results in increased lesion size and development of an unstable phenotype.49 Lesions in the transgenic mice overexpressing dominant-negative type II receptors in T cells contain more macrophages and lymphocytes and less collagen, similar to mice treated with neutralizing antibodies; IFN-␥, which was also increased, could contribute to collagen reductions in the lesions. The recent identification of markers of CD4⫹CD25⫹ regulatory T cells in lesions raises the question as to whether the effect of impairing TGF- signaling in T lymphocytes is at least in part a consequence of reduced CD4⫹CD25⫹ regulatory T-cell activity.50 Depletion of CD4⫹CD25⫹ regulatory T cells increases lesion size in apoE⫺/⫺ mice.51 These cells, which constitute 5% to 10% of peripheral CD4⫹ lymphocytes, are capable of inhibiting CD4⫹ and CD8⫹ T-cell responses via TGF-– dependent mechanisms; T cells that do not respond to TGF- escape control by CD4⫹CD25⫹ regulatory T cells.52 TGF- supports Foxp3 expression in these cells, their regulatory function, and homeostasis. Foxp3 is a master control gene for the development and function of CD4⫹CD25⫹ regulatory T cells and is upregulated in atherosclerotic lesions of apoE⫺/⫺ mice, suggesting an important role for these cells in regulating atherosclerosis.50 Depletion of TGF- greatly reduces their numbers in the periphery.53 Furthermore, inhibition of TGF- signaling markedly reduces Foxp3 expression, impairing their suppressor activity. Together, these studies indicate that TGF- promotes a stable lesion phenotype by ⱖ2 mechanisms, stimulating collagen biosynthesis by 1716 Arterioscler Thromb Vasc Biol. August 2006 Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 VSMCs and inhibiting T-cell activation either directly or indirectly via CD4⫹CD25⫹ regulatory T cells. Evidence for a role for BMPs in atherogenesis is more indirect. BMP-2, BMP-4, and BMP-6 are expressed in advanced atherosclerotic lesions and associated with lesion calcification.54,55 BMP-2 not only induces VSMC cycle arrest but also stimulates the loss of smooth muscle cell markers56 and the gain of an osteoblastic gene expression profile related to Msx-2 and Runx, transcription factors that promote osteogenic gene expression.57 BMP-2 may also induce apoptosis; apoptosis appears to be critical to the initiation and propagation of calcification by calcifying vascular cells. Reductions in atherosclerotic lesions of matrix Gla protein would promote calcification by a BMP-2– dependent mechanism.58 It will be of interest to determine whether overexpression of BMP antagonists such as noggin reduces calcification of advanced atherosclerotic lesions in apoE⫺/⫺ mice.59 Recently, BMP-7 has been shown to reduce calcification of lesions.60 The mechanism by which BMP-7 reduces calcification may be related its ability to promote a contractile phenotype in smooth muscle cells and reduce serum phosphate levels. TGF- and Restenosis Restenosis attributable to excessive intimal fibrocellular proliferation and inward remodeling is the main limitation to therapeutic revascularization, angioplasty, stenting, or atherectomy used to treat obstructive atherosclerotic lesions. The TGF- system is rapidly upregulated after balloon catheter injury to vessels with increases in TGF- isoforms, together with the type II TGF- receptor and ALK-5.61 After endothelial denudation, platelets attached to the site of injury degranulate, releasing large amounts of TGF-;62 this can further enhance platelet aggregation63 and stimulate apoptosis of surviving endothelial cells64 and promote smooth muscle cell survival.65 The TGF- inhibitory binding protein vasorin is also downregulated, enabling TGF- to participate in the healing process.66 Two lines of evidence suggest that TGF- contributes to restenosis, (1) its overexpression stimulates neointimal hyperplasia and extracellular matrix accumulation,67 and (2) targeting TGF-1 mRNA degradation with chimeric DNA–RNA hammerhead ribozymes attenuates neointima growth.68 Pharmacological inhibition of TGF-1 signaling also attenuates neointima growth and remodeling after stenting.69 The mechanisms by which TGF- promotes proliferation under these circumstances most likely involve TGF-–stimulating release of mitogenic growth factors. Low concentrations of TGF- stimulate PDGF-AA expression, PDGF-B expression, and release of extracellular fibroblast growth factor-2.70,71 TGF-1 may also enhance proliferation by upregulating Nox4, a gp91phox homologue of the NADPH oxidase system, and increasing reactive oxygen species production with transient oxidative inactivation of phosphatases and augmentation of growth signaling cascades.72 Inhibition of TGF-1 in addition to reducing intimal proliferation also reduces collagen accumulation in the neointima. These combined results suggest that TGF-1 is a potential target to reduce restenosis. It will be of interest to determine whether the recently developed ALK-5 antago- nists,73 adsorbed onto stents, delivered by microparticles or administered systemically can prevent clinical restenosis. TGF- Signaling and HHT HHT is an autosomal dominant disorder affecting ⬇1 in 8000 individuals. Serious complications of HHT include pulmonary, cerebral, and hepatic arteriovenous malformations, which can lead to severe hemorrhage, stroke, and brain abscess. Mutations in 2 receptors of the TGF- family have been causally linked to HHT: endoglin for type I HHT and ALK-1 for type 2 HHT.74,75 Mutations of all types are distributed through both genes, and severity of diseases does not correlate with any aspecific mutations. Mutations in endoglin include deletions, insertions, and missense mutations and splice site changes, the majority representing null alleles, which lead to reduced levels of endoglin protein on the surface of endothelial cells. More than 150 mutations have been reported in endoglin, mostly within exons 1 to 12, which encode the extracellular domain, and none in exons 13 and 14, which encode the transmembrane and cytoplasmic domains, respectively. More than 120 mutations have been reported in ALK-1 with more than half being missense mutations and the remaining being small deletions, insertions, splice site mutations, and nonsense mutations frequently leading to truncated proteins.76 The most common mutations occur in both the extracellular region and kinase domain with frequencies highest in the kinase domain. Mutations in the kinase domain lead to alterations in polarity, charge, and hydrophobicity, as well as misfolding of the protein. HHT1 has a higher prevalence of pulmonary arteriovenous malformations, and HHT2 families generally exhibit a milder phenotype and later onset of disease.77 It still remains to be determined how reductions in endoglin or ALK-1 predispose to HHT and what causes vascular lesions to develop in selective vascular beds. Some insights into mechanisms responsible for the disease have been obtained from endoglin⫹/⫺ and ALK-1⫹/⫺ mice.78,79 Endoglin-deficient mice die at midgestation of angiogenic and cardiovascular defects. Vasculogenesis in these mice is normal, but angiogenesis is impaired along with remodeling of the primary vascular plexus. The mice exhibit poor VSMC development that results in dilatation and rupture of the vascular channels. In the heterozygous mice, disease severity increases with age and can include rupture of major vessels. During development, both endoglin- and ALK-1– deficient mice lose structural, molecular, and functional distinctions between arteries and veins, but only ALK-1– deficient mice exhibit profound vessel dilatation.79,80 Endoglin⫹/⫺ mice generally exhibit a greater number of dilated venules, a greater number of capillaries across the dermis, and large numbers of irregular or thinned vessels with reduced numbers of smooth muscle cells. The reduction in smooth muscle cell numbers appears at least in part attributable to defective vessel formation in early development, probably the consequence of reductions in the production of autoinducible TGF- by endothelial cells.81 Recruitment of mesenchymal cells into new vessels is achieved in part by TGF-. On contact of mesenchymal cells with the endothelium, latent TGF- is activated, inducing differentiation of mesenchymal Bobik Transforming Growth Factor-s and Vascular Disorders Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 cells into pericytes and smooth muscle cells.82 In endoglindeficient mice, differentiation of smooth muscle cells can be rescued with exogenous TGF-1.81 Endothelial cells from subjects with type I HHT also exhibit reduced production of TGF-1.83 These cells also exhibit disorganized cytoskeleton and fail to form endothelial cell tubes. A disorganized cytoskeleton is prone to cell breaking with changes in shear stress and blood pressure. The latter defect may be the consequence of reduced endothelial NO synthase/Hsp90 association and uncoupling endothelial NO synthase activity, resulting in increased endothelial NO synthase– derived superoxide anion production rather than NO production.84 Although endoglin and ALK-1 mutations are strongly associated with development of HHT, the clinical manifestations of HHT are highly heterogenous between families as well as within a given family with the same mutation; also in mice, the high prevalence of HHT in endoglin⫹/⫺ 129/Ola mice compared with endoglin⫹/⫺ C57BL6 mice suggests an involvement of modifier genes.85 Thus, although defective TGF- signaling in endothelial cells attributable to mutations in endoglin and ALK-1 are clearly important in HHT, other yet to be identified genetic and epigenetic factors also contribute. Identifying these genes, which could involve genes regulating downstream TGF- signaling and also understanding how mutations in ALK-1 and endoglin contribute to abnormalities in vessel development, should provide further insights into this vascular disorder. Recently, mutations in smad4 have been associated with the combined syndrome of juvenile polyposis and HHT, suggesting a role for downstream TGF- signaling components in HHT.86 Vessel Remodeling in PPH PPH is characterized by a marked and sustained elevation in pulmonary vascular resistance. Typical pathological features of this disorder include enhanced cell proliferation, muscularization, the obliteration of small pulmonary arteries, and formation of plexiform lesions. PPH has been strongly linked to mutations in the BMPR-II gene, suggesting that impaired BMP signaling greatly increases susceptibility to this disorder.87 Most of the mutations in the BMPR-II gene are predicted to lead to premature termination codons, but some missense mutations have also been identified, suggesting that the mutations can contribute to PPH via haploinsufficiency or dominant-negative mechanisms. Mutations include nonsense or frame shift mutations in the extracellular domain, which can lead to premature truncation of the transcripts and the absence of production of transmembrane BMPR-II proteins. Missense mutations involving conserved cysteine residues in the extracellular domain and missense or frame shift mutations in the kinase domain or frame shift or nonsense mutations within the cytoplasmic tail result in cytoplasmic truncation of the receptor.88 However, although mutations in BMPR-II have been strongly linked to PPH, additional environmental and genetic factors are also required for development of clinically significant PPH. Family members with identical mutations in BMPR-II have a 15% to 20% chance of developing PPH.88 In support of the importance of environmental factors, mice carrying 1 mutant allele (BMPRII⫹/⫺) exhibit increased pulmonary vascular resistance and 1717 Figure 3. BMPR-II mutations in pulmonary hypertension. Cysteine mutations in either the extracellular ligand binding or kinase domains prevent receptor trafficking to the cell membrane. Noncysteine mutations in the kinase domain result in impaired Smad phosphorylation and Smad-mediated signaling. Mutations in the C-terminal domain leads to impaired Smadindependent signaling by reducing interactions with cell cycle regulators (eg, c-Src). All mutations result in an impaired ability of BMPs to inhibit cell proliferation. thickened muscularized arteries.89 However, vascular obliteration or plexiform lesions typically found in patients with severe PPH is absent. Similarly, mice engineered to conditionally express a human dominant-negative BMPR-II mutation in smooth muscle cells also exhibit elevated pulmonary artery pressure but only mild pulmonary arterial muscularization.90 The small increase in muscularization suggests that deficiencies in BMPR-II signaling in additional cell types, such as endothelial cells and possibly fibroblasts, may also be important for induction of the vascular changes associated with PPH; BMPR-II in normal lung is predominately expressed in endothelial cells and to a lesser extent on smooth muscle cells. The apparent disparity between the rise in pulmonary pressure and extent of vessel muscularization suggests enhanced pulmonary vasoconstriction in mice carrying the dominant-negative BMPR-II mutation and is consistent with a 2-phase hypothesis for PPH in which early disease is characterized by enhanced vasoconstriction and minimal vascular remodeling and later disease by progressive remodeling and little vasoconstriction.91 Although it is clear that factors in additional to mutations in BMPR-II, possibly serotonin,92 are required to initiate the proliferation that leads to the vascular obliteration in pulmonary hypertension, defective BMP signaling allows proliferation and intimal smooth muscle cell accumulation to proceed largely unabated, obliterating small arteries. In pulmonary arterial smooth muscle cells from subjects with PPH, the actions of BMP such as induction of apoptosis, suppression of DNA synthesis and inhibition of proliferation are markedly attenuated.93 The mechanism by which BMPR-II mutants disrupt BMP/Smad signaling is heterogenous and mutation specific. Mutations in the extracellular ligand-binding domain of BMPR-II, which results in substitution of cysteine residues, prevent receptors from reaching the cell membrane, effectively reducing the number of functional receptors (Figure 3). Missense mutations in the kinase domain lead to reductions in Smad1 signaling and unopposed p38MAPK/ ERK signaling, leading to abnormal vascular cell proliferation.41 Mutations in the cytoplasmic tail of BMPR-II, includ- 1718 Arterioscler Thromb Vasc Biol. August 2006 Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 ing those responsible for truncating its unusually long cytoplasmic tail, affect other BMP signaling cascades that can also affect proliferation. Mutations in the cytoplasmic tail resulting in exon 12 deletion does not affect Smad phosphorylation or p38MAPK activation, rather it affects the phosphorylation of Tctex-1, a light chain of the motor complex Dynein; in normal lung, BMPR-II and Tctex-1 colocalize in endothelial and smooth muscle cells.94 c-Src is also an interacting partner of the C-terminal domain of BMPR-II; truncation of the C terminus disrupts their interaction, whereas missense mutation in the kinase domain reduces their interaction, impairing the ability of BMPR-II to inhibit c-Src activating phosphorylation.95 In pulmonary artery, smooth muscle serotonin activates c-Src, resulting in phosphorylation of PDGF receptor and ERK1/2 MAPK and activating cell cycle regulators, such as cyclins D and E, leading to cell proliferation. The C-terminal domain also interacts with LIM kinase 1, which regulates actin dynamics by phosphorylating cofilin. Mutations in BMPR-II, which result in even small deletions in the C-terminal region, fail to bind or inhibit LIM kinase 1, suggesting that alterations in the dynamics of the actin cytoskeleton may contribute to PPH susceptibility.96 Recently, other proteins have been shown to associate with the C-terminal tail of BMPR-II, including regulators of the cell cycle, apoptosis, cytoskeleton, and kinases, but their functional significance for PPH is yet to be elucidated. Although the functional consequences of mutations in BMPR-II are providing new insights as to how mutations in BMPR-II may predispose to PPH, many questions remain unanswered, particularly in relation to functional consequences of loss of BMPR-II signaling in other cell types such as endothelium. Mutations in ALK-1, which has been associated with HHT, have also recently been linked to PPH.97 Conclusions In conclusion, evidence from animal models and correlative data from human studies implicate TGF- superfamily members TGF- and BMPs in the regulation or development of a wide range of vascular disorders. Additional studies are required to more clearly define how alterations in TGF-/ BMP signaling contribute to these disorders and design appropriate therapeutic strategies. Studies focusing on mechanisms underlying disease heterogeneity in HHT should provide important insights as to how mutations in endoglin and ALK-1 are involved in its development. In atherosclerosis, TGF- appears to protect against the development of unstable lesions by stimulating VSMCs to produce collagen and suppressing the activity of T cells either directly or indirectly by CD4⫹CD25⫹ regulatory T cells producing TGF-. In the future, it will be of interest to determine whether therapeutic activation of the TGF- system is sufficient to alter the phenotype of an atherosclerotic lesion by promoting the transition of an unstable lesion into a stabilized lesion. Recently, a novel immunomodulating agent has been introduced: FTY720. Because FTY720 mimics TGF- responses, activating Smads and the expression of extracellular matrix proteins, this compound may be useful for testing such a hypothesis.98 In pulmonary hypertension attributable to mutations in BMPR-II, it will be important to definitively identify common downstream signaling mechanisms affected by the reported mutations. Their identification could become the staging platform for therapeutically targeting PPH in susceptible individuals through stimulators of the pathway. In restenosis, attenuating TGF- actions in the injured vessel wall, using novel agents such as the recently developed inhibitors of TGF- receptor kinases73 or a Smad3 inhibitor,99 may be therapeutically useful. References 1. Sluijter JPG, Verloop RE, Pulskens WPC, Velema E, Grimbergen JM, Quax PH, Goumans MJ, Pasterkamp G, de Kleijn PV. Involvement of furin-like proprotein convertases in the arterial response to injury. Cardiovasc Res. 2005;68:136 –143. 2. Reddi AH. Interplay between bone morphogenetic proteins and cognate binding proteins in bone and cartilage development: noggin, chordin and DAN. Arthritis Res. 2001;3:1–5. 3. Nohe A, Hassel S, Ehrlich M, Neubauer F, Sebald W, Henis YI, Knaus P. The mode of bone morphogenetic protein (BMP) receptor oligomerization determines different BMP-2 signaling pathways. J Biol Chem. 2002;277:5330 –5338. 4. ten Dijke P, Hill CS. New insights into TGF--Smad signaling. Trends Biochem Sci. 2004;29:265–273. 5. Ebisawa T, Fukuchi M, Murakami G, Ghiba T, Tanaka K, Imamura T, Miyazono K. Smurf1 interacts with transforming growth factor- type I receptor through Smad7 and induces receptor degradation. J Biol Chem. 2001;276:12477–12480. 6. Goumans MJ, Valdimarsdottir G, Itoh S, Rosendahl A, Sideras P, ten Dijke P. Balancing the activation state of the endothelium via two distinct TGF- type I receptors. EMBO J. 2002;21:1743–1753. 7. Ota T, Fujii M, Sugizaki T, Ishii M, Miyazawa K, Aburatani H, Miyazono K. Targets of transcriptional regulation by two distinct type I receptors for transforming growth factor- in human umbilical vein endothelial cells. J Cell Physiol. 2002;193:299 –318. 8. Valdimarsdottir G, Goumans MJ, Rosendahl A, Brugman M, Itoh S, Lebrin F, Sideras P, ten Dijke P. Stimulation of Id1 expression by bone morphogenetic protein is sufficient and necessary for bone morphogenetic protein-induced activation of endothelial cells. Circulation. 2002; 106:2263–2270. 9. Watabe T, Nishihara A, Mishima K, Yamashita J, Shimizu K, Miyazawa K, Nishikawa SI, Miyazono K. TGF- receptor kinase inhibitor enhances growth and integrity of embryonic stem cell-derived endothelial cells. J Cell Biol. 2003;163:1303–1311. 10. Goumans MJ, Valdimarsdottir G, Itoh S, Lebrin F, Larsson J, Mummery C, Karlsson S, ten Dijke P. Activin receptor-like kinase (ALK) 1 is an antagonist mediator of lateral TGF-/ALK5 signaling. Mol Cell. 2003;12:817–828. 11. Guerrero-Esteo M, Sanchez-Elsner T, Letamendia A, Bernabeu C. Extracellular and cytoplasmic domains of endoglin interact with the transforming growth factor- receptors II and I. J Biol Chem. 2002;277:29197–29209. 12. Yamagami S, Yokoo S, Mimura T, Amino S. Effects of TGF-2 on immune response-related gene expression profiles in the human corneal endothelium. Invest Ophthalmol Vis Sci. 2004;45:515–521. 13. Agrotis A, Samuel M, Prapas G, Bobik A. Vascular smooth muscle cells express multiple type I receptors for TGF-, activin and bone morphogenetic proteins. Biochem Biophys Res Commun. 1996;219:613– 618. 14. Seay U, Sedding D, Krick S, Hecker M, Seegar W, Ieickelberg O. TGF--dependent growth inhibition in primary vascular smooth muscle cells is p38-dependent. J Pharmacol Exp Ther. 2005;315:1005–1012. 15. Khanna A. Concerted effect of transforming growth factor-, cyclin inhibitor p21 and c-myc on smooth muscle cell proliferation. Am J Physiol. 2004;286:H1133–H1140. 16. Feinberg MW, Watanabe M, Lebedeva MA, Depina AS, Hanai J, Mammoto T, Frederick JP, Wang XF, Sukhatme VP, Jain MK. Transforming growth factor-1 inhibition of vascular smooth muscle cell activation is mediated via Smad3. J Biol Chem. 2004;279:16388 –16393. 17. Samarakoon R, Higgins CE, Higgins SP, Kutz SM, Higgins PJ. Plasminogen activator inhibitor type-I gene expression and induced migration in TGF-1–stimulated smooth muscle cells is pp60(c-Src)/MEK-dependent. J Cell Physiol. 2005;204:236 –246. 18. Hocevar BA, Prunier C, Howe PH. Disabled-2 (Dab2) mediates transforming growth factor  (TGF)-stimulated fibronectin synthesis through TGF-activated kinase ! and activation of the JNK pathway. J Biol Chem. 2005;280:25920 –25927. Bobik Transforming Growth Factor-s and Vascular Disorders Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 19. Ashcroft GS. Bidirectional regulation of macrophage function by TGF-. Microbes Infect. 1999;1:1275–1282. 20. Wahl SM, Allen JB, Weeks BS, Wong HL, Klotman PE. Transforming growth factor  enhances integrin expression and type IV collagenase secretion in human monocytes. Proc Natl Acad Sci U S A. 1993;90:4577–4581. 21. Ashcroft GS, Yang X, Glcik AB, Weinstein M, Letterio JL, Mizel DE, anzano M, Greenwell-Wild T, Wahl SM, Deng C, Roberts AB. Mice lacking Smad3 show accelerated wound healing and an impaired local inflammatory response. Nat Cell Biol. 1999;1:260 –266. 22. Sato K, Kawasaki H, Nagayama H, Enomoto M, Morimoto C, Tadokoro K, Juji T, Takahashi TA. TGF-1 reciprocally controls chemotaxis of human peripheral blood monocyte-derived dendritic cells via chemokine receptors. J Immunol. 2000;164:2285–2295. 23. Turner M, Chantry D, Feldmann M. Transforming growth factor  induces the production of interleukin 6 by human peripheral blood mononuclear cells. Cytokine. 1990;2:211–216. 24. Panousis CG, Evans G, Zuckerman SH. TGF- increases cholesterol efflux and ABC-1 expression in macrophage-derived foam cells: opposing the effects of IFN-␥. J Lipid Res. 2001;42:856 – 863. 25. Irvine SA, Foka P, Rogers SA, Mead JR, Ramji DP. A critical role for the Ap1-binding sites in the transforming growth factor-mediated inhibition of lipoprotein lipase gene expression in macrophages. Nucleic Acids Res. 2005;33:1423–1434. 26. Werner F, Jain MK, Feinberg MW, Sibinga ES, Pellacani A, Wiesel P, Chin MT, Topper JN, Perrella MA, Lee ME. Transforming growth factor-1 inhibition of macrophage activation is mediated via Smad3. J Biol Chem. 2000;275:36653–36665. 27. Mitani T, Terashima M, Yoshimura H, Nariai Y, Tanigawa Y. TGF-1 enhances degradation of IFN-␥-induced iNOS protein via proteasomes in RAW264.7 cells. Nitric Oxide. 2005;13:78 – 87. 28. Dai Y, Datta S, Novotny M, Hamilton TA. TGF inhibits LPS-induced chemokine mRNA stabilization. Blood. 2003;102:1178 –1185. 29. Gorelik L, Flavell RA. Abrogation of TGF signaling in T cells leads to spontaneous T cell differentiation and autoimmune disease. Immunity. 2000;12:171–181. 30. Nakao A, Miike S, Hatano M, Okumura K, Tokuhisa T, Ra C, Iwamoto I. Blockade of transforming growth factor /smad signaling in T cells by overexpression of smad7 enhances antigen-induced airway inflammation and airway reactivity. J Exp Med. 2000;192:151–158. 31. Cottrez F, Groux H. Regulation of TGF- response during T cell activation is modulated by IL-10. J Immunol. 2001;167:773–778. 32. Murphy KM, Reiner SL. The lineage decisions of helper T cells. Nat Rev Immunol. 2002;2:933–944. 33. Ogawa K, Chen F, Kim YJ, Chen Y. Transcriptional regulation of tristetraprolin by transforming growth factor- in human T cells. J Biol Chem. 2003;278:30373–30381. 34. Li MO, Wan YY, Sanjabi S, Robertson AKL, Flavell RA. Transforming growth factor- regulation of immune responses. Annu Rev Immunol. 2006;24:99 –146. 35. Ronger-Savle S, Valladeau J, Claudy A, Schmitt D, Peguet-Navarro J, Dezutter-Dambuyant C, Thomas L, Jullien D. TGF- inhibits CD1d expression on dendritic cells. J Invest Dermatol. 2005;124:116 –118. 36. Schramm C, Huber S, Protschka M, Czochra P, Burg J, Schmitt E, Lohse AW, Galle PR, Blessing M. TGF- regulates the CD4⫹CD25⫹ T-cell pool and the expression of Foxp3 in vivo. Int Immunol. 2004;16:1241–1249. 37. Raida M, Clement JH, Leek RD, Ameri K, Bicknell R, Niederweiser D, Harris AL. Bone morphogentic protein (BMP-2) and induction of tumour angiogenesis. J Cancer Res Clin Oncol. 2005;131:741–750. 38. Sorescu GP, Song H, Tressel SL, Hwang J, Dikalov S, Smith DA, Boyd NL, Platt MO, Lassegue B, Griendling KK, Jo H. Bone morphogenetic protein 4 produced in endothelial cells by oscillatory shear stress induces monocyte adhesion by stimulating reactive oxygen species production from a nox1-based NADPH oxidase. Circ Res. 2004;95:773–779. 39. Kiyono M, Shibuya M. Bone morphogenetic protein4 mediates apoptosis of capillary endothelial cells during rat pupillary membrane regression. Mol Cell Biol. 2003;23:4627– 4636. 40. Dorai H, Vukicevic S, Sampath TK. Bone morphogenetic protein-7 (osteogenic protein-1) inhibits smooth muscle cell proliferation and stimulates the expression of markers that are characteristic of SMC phenotype in vitro. J Cell Physiol. 2000;184:37– 45. 41. Yang X, Long L, Southwood M, Rudarakanchana N, Upton PD, Jeffery TK, Atkinson C, Chen H, Trembath RC, Morrell NW. Dysfunctional Smad signaling contributes to abnormal smooth muscle cell proliferation in familial pulmonary arterial hypertension. Circ Res. 2005;96:1053–1063. 1719 42. Bobik A, Agrotis A, Kanellakis P, Dilley R, Krushinsky A, Smirnov V, Tararak E, Condron M, Kostolias G. Distinct patterns of transforming growth factor- isoforms and receptor expression in human atherosclerotic lesions. Colocalisation implicates TGF- in fibrofatty lesion development. Circulation. 1999;99:2883–2891. 43. Cipollone F, Fazia M, Mincione G, Iezzi A, Pini B, Cuccurullo C, Ucchino S, Spigonardo F, Di Nisio M, Cuccerullo F, Mezzetti A, Porreca E. Increased expression of transforming growth factor-1 as a stabilizing factor in human atherosclerotic plaques. Stroke. 2004;35:2253–2257. 44. McCaffrey TA, Consigli S, Du B, Falcone DJ, Sanborn TA, Spokojny AM, Bush HL Jr. Decreased type II/type I TGF- receptor ratio in cells derived from human atherosclerotic lesions. Conversion from an antiproliferative to profibrotic response to TGF-. J Clin Invest. 1995;96:2667–2675. 45. Kalinina N, Agrotis A, Antropova Y, Ilyinskaya O, Smirnov V, Tararak E, Bobik A. Smad expression in human atherosclerotic lesions: evidence for impaired TGF-/Smad signaling in smooth muscle cells of fibrofatty lesions. Arterioscler Thromb Vasc Biol. 2004;24:1391–1396. 46. Amento EP, Ehsani N, Palmer H, Libby P. Cytokines and growth factors positively and negatively regulate interstitial collagen gene expression. Arterioscler Thromb Vasc Biol. 1991;11:1223–1230. 47. Mallat Z, Gojova A, Marchiol-Fournigault C, Esposito B, Kamate C, Merval R, Fradelizi D, Tedgui A. Inhibition of TGF- signaling accelerates atherosclerosis and induces an unstable plaque phenotype in mice. Circ Res. 2001;89:930 –934. 48. Lutgens E, Gijbels M, Smook M, Heeringa P, Gotwels P, Kotlaiansky VE, Daemen MJ. TGF- mediates a balance between inflammation and fibrosis during plaque progression. Arterioscler Thromb Vasc Biol. 2002;22:975–982. 49. Robertson AK, Rudling M, Zhou X, Gorelik L, Flavell RA, Hansson GK. Disruption of TGF- in T cells accelerates atherosclerosis. J Clin Invest. 2003;112:1342–1350. 50. Veillard NR, Steffens S, Burger F, Pelli G, Mach F. Differential expression patterns of proinflammatory and antiinflammatory mediators during atherogenesis in mice. Arterioscler Thromb Vasc Biol. 2004;24: 2339 –2344. 51. Ait-Oufella H, Salomon BL, Potteaux S, Roberston AKL, Gourdy P, Zoll J, Merval R, Espopsito B, Cohen JL, Fisson S, Flavell RA, Hansson GK, Klatzmann D, Tedgui A, Mallat Z. Natural regulatory T cells control the development of atherosclerosis in mice. Nat Med. 2006;12:178 –180. 52. Fahlen L, Read S, Gorlik L, Hurst SD, Coffman RL, Flavell RA, Powrie F. T cells that cannot respond to TGF escape control by CD4⫹CD25⫹ regulatory T cells. J Exp Med. 2005;201:737–746. 53. Marie JC, Letterio JJ, Gavin M, Rudensky AY. TGF-1 maintains suppressor function and Foxp3 expression in CD4⫹CD25⫹ regulatory T cells. J Exp Med. 2005;201:1061–1067. 54. Bostrom K, Watson KE, Horn S, Wortham C, Herman IM, Demer LL. Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest. 1993;91:1800 –1809. 55. Dhore CR, Cleutjens JOM, Lutgens E, Cleutjens KBJM, Geusens PPM, Kitslaar PJEHM, Tordoir JHM, Spronk HMH, Vermeer C, Daemen MJAP. Differential expression of bone matrix regulatory proteins in human atherosclerotic plaques. Arterioscler Thromb Vasc Biol. 2001;21:1998–2003. 56. King KE, Iyemere VP, Weissberg PL, Shanahan CM. Kruppel-like factor 4 (KLF4/GKLF) is a target of bone morphogenetic proteins and transforming growth factor 1 in the regulation of vascular smooth muscle phenotype. J Biol Chem. 2003;278:11661–11669. 57. Tyson KL, Reynolds JL, McNair R, Zhang Q, Weissberg PL, Shanahan CM. Osteo/chondrocytic transcription factors and their target genes exhibit distinct patterns of expression in human arterial calcification. Arterioscler Thromb Vasc Biol. 2003;23:489 – 494. 58. Hao H, Hirota S, Ishibashi-Ueda H, Kushiro T, Kanmatsuse K, Yutani C. Expression of matrix Gla protein and osteonectin mRNA by human aortic smooth muscle cells. Cardiovasc Pathol. 2004;13:195–202. 59. Wu XB, Li Y, Schneider A, Yu W, Rajendren G, Iqbal J, Yamamotot M, Alam M, Brunet LJ, Blair HC, Zaidi M, Abe E. Impaired osteoblastic differentiation, reduced bone formation and severe osteoporosis in noggin-overexpressing mice. J Clin Invest. 2003;112:924 –934. 60. Davies MR, Lund R, Kruska KA. BMP-7 is an efficacious treatment of vascular calcification in a murine model of atherosclerosis and chronic renal failure. J Am Soc Nephrol. 2003;14:1559 –1567. 61. Ward MR, Agrotis A, Kanellakis P, Dilley R, Jennings G, Bobik A. Inhibition of protein tyrosine kinases attenuates increases in expression of transforming growth factor- isoforms and their receptors after arterial injury. Arterioscler Thromb Vasc Biol. 1997;17:2461–2470. 1720 Arterioscler Thromb Vasc Biol. August 2006 Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 62. Assoain RK, Sporn MB. Type  transforming growth factor in human platelets: release during platelet degranulation and action on vascular smooth muscle cells. J Cell Biol. 1986;102:1217–1223. 63. Hoying JB, Yin M, Diebold R, Ormsby I, Becker A, Doetschman T. Transforming growth factor 1 enhances platelet aggregation through a non-transcriptional effect on the fibrinogen receptor. J Biol Chem. 1999; 274:31008 –31013. 64. Wassmer SC, de Souza JB, Frere C, Candal FJ, Juhan-Vague I, Grau GE. TGF-1 released from activated platelets can induce TNF-stimulated human brain endothelium apoptosis: a new mechanism for microvascular lesion during cerebral malaria. J Immunol. 2006;176:1180 –1184. 65. Pollman MJ, Naumovski L, Gibbons GH. Vascular cell apoptosis: cell type-specific modulation by transforming growth factor-1 in endothelial cells versus smooth muscle cells. Circulation. 1999;99:2019 –2026. 66. Ikeda Y, Imai Y, Kumagai H, Nosaka T, Morikawa Y, Hisaoka T, Manabe I, Maemura K, Nakaoka T, Imamura T, Miyazono K, Komuro I, Nagai R, Kitamura T. Vasorin, a transforming growth factor -binding protein expressed in vascular smooth muscle cells, modulates the arterial response to injury in vivo. Proc Natl Acad Sci U S A. 2004;101:10732–10737. 67. Nabel EG, Shum L, Pompili VJ, Yang ZY, San H, Shu HB, Liptay S, Gold L, Gordon D, Derynck R, et al. Direct transfer of transforming growth factor-1 gene into arteries stimulates fibrocellular hyperplasia. Proc Natl Acad Sci U S A. 1993;90:10759 –10763. 68. Yamamoto K, Morishita R, Tomita N, Shimozato T, Nakagami H, Kikuchi A, Aoki M, Higaki J, Kaneda Y, Ogihara T. Ribozyme oligonucleotides against transforming growth factor- inhibited neointimal formation after vascular injury in rat model. Circulation. 2000;102:1308–1314. 69. Ward MR, Agrotis A, Kanellakis P, Hall J, Jennings G, Bobik A. Tranilast prevents activation of transforming growth factor system, leukocyte accumulation and neointimal growth in porcine coronary arteries after stenting. Arterioscler Thromb Vasc Biol. 2002;22:940 –948. 70. Battegay EJ, Raines EW, Seifert RA, Bowen-Pope DF, Ross R. TGF- induces bimodal proliferation of connective tissue cells via complex control of an autocrine PDGF loop. Cell. 1990;63:515–524. 71. Khalil N, Xu YD, O’Connor R, Duronio V. Proliferation of pulmonary interstitial fibroblasts is mediated by TGF- induced release of extracellular FGF-2 and phosphorylation of p38MAPK and JNK. J Biol Chem. 2005;280:43000 – 43009. 72. Sturrock A, Cahill B, Norman K, Huecksteadt TP, Hill K, Sanders K, Karwande SV, Stringham JC, Bull DA, Gleich M, Kennedy TP, Hoidal JR. Transforming growth factor-beta1 induces Nox4 NAD(P)H oxidase and reactive oxygen species-dependent proliferation in human pulmonary artery smooth muscle cells. Am J Physiol Cell Mol Physiol. 2006;290:L661–L673. 73. Peng SB, Yan L, Xia X, Watkins SA, Brooks HB, Beight D, Herron DK, Jones ML, Lampe JW, McMillen WT, Mort N, Sawyer JS, Yingling JM. Kinetic characterization of novel pyrazole TGF- receptor I kinase inhibitors and their blockade of epithalial mesenchymal transition. Biochemistry. 2005;44:2293–2304. 74. McAllister KA, Grogg KM, Johnson DW, Gallione CJ, Baldwin MA, Jackson CE, Helmbold EA, Markel DS, McKinnon WC, Murrell J et al. Endoglin, a TGF- binding protein of endothelial cells, is the gene for hereditary haemorrhagic telangiectasia type 1. Nat Genet. 1994;8:345–351. 75. Berg JN, Gallione CJ, Stenzel TT, Johnson DW, Allen WP, Schwartz CE, Jackson CE, Porteous ME, Marxhuk DA. The activin receptor-like kinase 1 gene: genomic structure and mutations in hereditary hemorrhagic telangiectasia. Am J Hum Genet. 1997;61:60 – 67. 76. Harrison RE, Flanagan JA, Sankelo M, Abdalla SA, Rowell J, Machado RD, Elliott CG, Robbins IM, Olschewski H, McLaughlin V, Gruenig E, Kermeen F, Laitinen T, Morrell NW, Trembath RC. Molecular and functional analysis identifies ALK-1 as the predominant cause of pulmonary hypertension related to hereditary haemorrhagic telangiectasia. J Med Genet. 2003;40:865– 871. 77. Berg J, Guttmacher A, Marchuk D, Porteous ME. Clinical heterogeneity in hereditary haemorrhagic telangiectasia: are pulmonary arteriovenous malformations more common in families linked to endoglin? J Med Genet. 1996;33:256 –257. 78. Bourdeau A, Faughnan ME, Letarte M. Endoglin-deficient mice, a unique model to study heteritart hemorrhagic telangiectasia. Trends Cardiovasc Med. 2000;10:279 –285. 79. Urness LD, Sorensen LK, Li DY. Arteriovenous malformations in mice lacking activin receptor-like kinase-1. Nat Genet. 2000;26:328 –331. 80. Sorensen LK, Brooke BS, Li DY, Urness LD. Loss of distinct arterial and venous boundaries in mice lacking endoglin, a vascular-specific TGF coreceptor. Dev Biol. 2003;261:235–250. 81. Carvalho RL, Jonker L, Goumans MJ, Larsson J, Bouman P, Karlsson S, ten Dijke P, Arthus HM, Mummery CL. Defective paracrine signaling by TGF in yolk sac vasculature of endoglin mutant mice: a paradigm for hereditary haemorrhagic telangiectasia. Development. 2004;131:6237–6247. 82. Lebrin F, Deckers M, Bertolino P, Ten Dijke P. TGF- receptor function in the endothelium. Cardiovasc Res. 2005;65:599 – 608. 83. Letarte M, McDonald LM, Li C, Kathirkamathamby K, Vera S, PeceBarbara N, Kumar S. Reduced endothelial secretion and plasma levels of transforming growth factor-1 in patients with hereditary hemorrhagic telangiectasia type 1. Cardiovasc Res. 2005;68:155–164. 84. Toporsian M, Gros R, Kabir MG, Vera S, Govindaraju K, Eidelman DH, Husian M, Letarte M. A role for endoglin in coupling eNOS activity and regulating vascular tone revealed in hereditary hemorrhagic telangiectasia. Circ Res. 2005;96:684 – 692. 85. Bourdeau A, Faughnan ME, McDonald ML, Paterson AD, Wanless IR, Letarte M. Potential role of modifier genes influencing transforming growth factor-1 levels in the development of vascular defects in endoglin heterozygous mice with hereditary hemorrhagic telangiectasia. Am J Pathol. 2001;158:2011–2020. 86. Gallione CJ, Repetto GM, Legius E, Rustgi AK, Schelley SL, Tejpar S, Mitchell G, Droulin E, Westermann CJJ, Marchuk DA. A combined syndrome of juvenile polyposis and hereditary haemorrhagic telangiectasia with mutations in MADH4 (SMAD4). Lancet. 2004;363:852–859. 87. Lane KB, Machado RD, Pauciulo MW, Thomson JR, Phillips JA III, Loyd JE, Nichols WC, Trembath RC; International PPH Consortium. Heterozygous germline mutations in BMPR2, encoding a TGF- receptor, cause familial primary pulmonary hypertension. Nat Genet. 2000;26:81–84. 88. Newman JH, Trembath RC, Morse JA, Grunig E, Loyd JE, Adnot C, Coccolo F, Ventura C, Phillips JA III, Knowles JA, Janssen B, Eickelberg O, Eddahibi S, Herve P, Nichols WC, Elliott G. Genetic basis of pulmonary arterial hypertension: current understanding and future directions. J Am Coll Cardiol. 2004;43(suppl 12):33S–39S. 89. Beppu H, Ichinose F, Kawai N, Jones RC, Yu PB, Zapol WM, Miyazono K, Li E, Blcoh KD. BMPR-II heterozygous mice have mild pulmonary hypertension and impaired pulmonary vascular remodeling response to prolonged hypoxia. Am J Physiol. 2004;287:L1241–L1247. 90. West J, Fagan K, Steudel W, Fouty B, Lane K, Harral J, Hoedt-Miller M, Tada Y, Ozimek J, Tuder E, Rodman DM. Pulmonary hypertension in transgenic mice expressing a dominant-negative BMPRII gene in smooth muscle. Circ Res. 2004;94:1109 –1114. 91. Reeves JT, Groves BM, Turkevich D. The case for treatment of selected patients with primary pulmonary hypertension. Am Rev Respir Dis. 1986;134:342–346. 92. Launay JM, Herve P, Peoch K, Tournois C, Callebert J, Nebigil CG, Etienne N, Drouet L, Humbert M, Simonneau G, Maroteaux L. Function of the serotonin 5-hydroxytryptamine 2B receptor in pulmonary hypertension. Nat Med. 2002;8:1129 –1135. 93. Morrell NW, Yang X, Upton PD, Jourdan KB, Morgan N, Sheares KK, Trembath RC. Altered growth responses of pulmonary artery smooth muscle cells from patients with primary pulmonary hypertension to transforming growth factor-1 and bone morphogenetic proteins. Circulation. 2001;104:790 –795. 94. Machado RD, Rudarakanchana N, Atkinson C, Flanagan JA, Harrison R, Morrell NW, Trembath RC. Functional interaction between BMPR-II and Tctex-1, a light chain of dynein, is isoforms-specific and disrupted by mutations underlying primary pulmonary hypertension. Hum Mol Genet. 2003;12: 3277–3286. 95. Wong WK, Knowles JA, Morse JH. Bone morphogenetic protein receptor type II C-terminus interacts with c-Src. Am J Respir Cell Mol Biol. 2005;33:438 – 446. 96. Foletta V, Lim MA, Soosairaiah J, Kelly AP, Stanely EG, Shannon M, He W, Das S, Massague J, Bernard O. Direct signaling by the BMP type II receptor via the cytoskeletal regulator LIMK1. J Cell Biol. 2003;162:1089–1098. 97. Harrison RE, Berger R, Haworth SG, Tulloh R, Mache CJ, Morrell NW, Aldred MA, Trembath RC. Transforming growth factor- receptor mutations and pulmonary arterial hypertension in childhood. Circulation. 2005;111:435– 441. 98. Xin C, Ren S, Eberhardt W, Pfeilschifter J, Huwiler A. The immunomodulator FTY720 and its phosphorylated derivative activate the Smad signaling cascade and upregulate connective tissue growth factor and collagen type IV expression in renal mesangial cells. Br J Pharmacol. 2006;147:164 –174. 99. Jinnin M, Ihn H, Tamaki K. Characterization of SIS3, a novel specific inhibitor of smad3 and its effects on transforming growth factor-1-induced extracellular matrix expression. Mol Pharmacol. 2006;69:597–607. Downloaded from http://atvb.ahajournals.org/ by guest on June 16, 2017 Transforming Growth Factor-βs and Vascular Disorders Alex Bobik Arterioscler Thromb Vasc Biol. 2006;26:1712-1720; originally published online May 4, 2006; doi: 10.1161/01.ATV.0000225287.20034.2c Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2006 American Heart Association, Inc. All rights reserved. Print ISSN: 1079-5642. Online ISSN: 1524-4636 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://atvb.ahajournals.org/content/26/8/1712 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online at: http://atvb.ahajournals.org//subscriptions/