Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
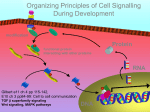
See related articles, pages 342–350 and 351–360 GDF15, a Cardioprotective TGF- Superfamily Protein Tetsuro Ago, Junichi Sadoshima he transforming growth factor- (TGF-) superfamily proteins, comprising more than 40 members (broadly divided into the TGF-s/activins/nodal family and the bone morphogenetic proteins [BMPs]/Müllerrian inhibiting substance/growth and differentiation factors [GDFs] family), were originally identified as molecules important for regulating development, differentiation, and tissue repair in various organs.1 TGF-1, a founding member of the TGF- superfamily, plays a key role in mediating cardiac hypertrophy2 and remodeling after myocardial infarction (MI) as an autocrine/paracrine factor.3 Increased TGF-1 expression is considered one of the few molecular markers that potentially discriminate between compensated and decompensated cardiac hypertrophy.3 Although TGF-1 may function protectively after MI by promoting scar formation, inhibiting neutrophil infiltration, and facilitating cardiomyogenic differentiation of adult hematopoietic stem cells,4 such beneficial effects last only briefly and sustained activation of TGF-1 causes structural remodeling, eventually leading to cardiac failure.5 Thus, TGF-1 is generally regarded as detrimental, inducing cardiac hypertrophy and failure in the adult heart. Compared with the wealth of knowledge regarding the effects of TGF-1 on the heart, much less is known as to how other members of the TGF- superfamily affect cardiac hypertrophy and failure.6 In this issue of Circulation Research, two companion articles report the effect of growth and differentiation factor 15 (GDF15), a 12-kDa secreted protein (and a 25-kDa disulfide-linked dimer) belonging to the TGF- superfamily, on cardiac hypertrophy and apoptosis.7,8 GDF15 is highly expressed in the placenta and the prostate, but not normally in many other organs, including the heart.9,10 However, expression of GDF15 is induced rapidly by IL-1, TNF␣, and TGF- in macrophages, thereby limiting macrophage activation and inflammation (Figure 1).9 In addition, p53, a tumor suppressor protein, induces expression of GDF15, which acts as a growth inhibitory molecule in tumor cells (Figure 1).10 Such growth inhibitory actions of GDF15 are unique compared with those of other targets of p53, such as p21/Waf-1, because GDF15 can act on neighboring cells as an “extracellular” messenger after being T Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 secreted. Kemph et al found that expression of GDF15 is induced rapidly in cardiomyocytes on ischemia/reperfusion (I/R) via the nitric oxide-peroxynitrite-dependent signaling pathway.8 GDF15 is also upregulated by other cardiovascular events triggering oxidative stress, including pressure overload, heart failure,7 and atherosclerosis11 (Figure 1). In the heart, Gdf15 gene targeted mice exhibited greater hypertrophy, which could also be attributable to exaggerated hyperplasia, with reduced left ventricular function in response to pressure-overload,7 and a greater MI and apoptosis after I/R.8 This is in striking contrast with Tgfb1 gene targeted mice, in which angiotensin II–induced hypertrophy is abrogated.2 Conversely, heart-specific GDF15-overexpressing mice are resistant to pressure overload-induced hypertrophy.7 These results are consistent with the notion that GDF15 is a protective molecule for the heart. This leads to the question as to why GDF15 exerts cardioprotective effects whereas TGF-1 does the opposite, despite the fact that both activate similar downstream signaling pathways, including the Smad (Small mother against decapentaplegic)-dependent signaling pathway. TGF- family proteins bind to distinct type I and type II serine/threonine kinase receptors. The specificity of the intracellular signaling is mainly determined by type I receptors (ALK1 to ALK7). Intracellular signaling mechanisms induced by the TGF- superfamily are broadly divided into Smad-dependent and -independent pathways (Figure 2).12 Receptor-activated Smads, including Smad2/3 and Smad1/ 5/8, are phosphorylated by type I receptors and, after forming a heterotrimeric complex with the common mediator Smad, namely Smad4, they are translocated into the nucleus and modulate transcription. The molecules activated by the Smadindependent pathway include MAPKs, TAK-1, and PI3K/ Akt, although the precise mechanisms by which TGF- receptors activate these molecules are not clearly understood.12 Is the Smad-Dependent Pathway Good or Bad for the Heart? Because the Smad-dependent pathway, the canonical TGF- signaling mechanism, is activated under several pathological conditions in the heart,13 it was postulated that the Smaddependent pathway mediates detrimental functions of TGF1. However, recent studies showed that this hypothesis may not necessarily be true. Wang et al reported a surprising observation that cardiac-specific Smad4 knockout mice resulted in cardiac hypertrophy and heart failure.14 Because Smad4 is considered the common transcriptional mediator of the Smad-dependent pathway, the observation by Wang et al suggests that the Smad-dependent pathway rather inhibits cardiac hypertrophy, apoptosis, and fibrosis, thereby acting in a protective manner. Although this observation does not The opinions expressed in this editorial are not necessarily those of the editors or of the American Heart Association. From the Cardiovascular Research Institute, Department of Cell Biology and Molecular Medicine, UMDNJ, New Jersey Medical School, Newark. Correspondence to Junichi Sadoshima, Cardiovascular Research Institute, Department of Cell Biology and Molecular Medicine, UMDNJ, New Jersey Medical School, 185 South Orange Avenue, MSB G-609, Newark, NJ 07103. E-mail [email protected] (Circ Res. 2006;98:294-297.) © 2006 American Heart Association, Inc. Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/01.RES.0000207919.83894.9d 294 Ago and Sadoshima TGF- Signaling in the Adult Heart 295 Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 Figure 1. Known upstream stimulators and functions of GDF15 exclude the participation of active Smads in hypertrophy and failure, the disadvantage caused by the lack of Smad4 overwhelms the few, if any, advantages to abolishing active Smad signaling in the heart. Xu et al found that Smad2 and Smad3 are phosphorylated on GDF15 treatment in cultured cardiomyocytes.7 Furthermore, adenovirus-mediated Smad2 overexpression suppressed hypertrophic responses, mimicking the effect of GDF15 overexpression.7 Together with the finding that GDF15 and Smad2 failed to show additive effects,7 these results strongly suggest that Smad2/3 mediate antihypertrophic and other cardioprotective effects of GDF15. Masaki et al reported that Smad1 is activated by I/R, which in turn reduces the size of MI and the amount of apoptotic cell death through upregulation of Bcl-xL and -catenin.15 Moreover, the loss of Smad5 also results in increased apoptosis in cardiomyocytes.16 Taken together, the Smad-dependent pathway appears to play antihypertrophic and antiapoptotic roles, thereby mediating the protective effect of GDF15 while counteracting the detrimental aspect of TGF-1 in the heart. Besides GDF15, BMP-2 seems to have an antiapoptotic effect through activation of Smad1.6 However, the protective effects for the heart in vivo caused by BMP-2 remain to be shown. Thus, to our knowledge, GDF15 is the first TGF- superfamily protein that plays a cardioprotective role in vivo in the adult heart. Because GDF15 activates Smad2 and Smad3,7 ALK-4/5/7 could be the candidate receptors for GDF15. Alternatively, judging from the similarity in the primary structure and Smads activation, GDF15 may be closer to the BMP subfamily than to the TGF- subfamily.1 Because BMP-2 activates ALK-2/3/6, which in turn phosphorylate Smad1/5, GDF15 may also activate one of these type I receptors and Smad1/Smad5 as well. What, then, is the signaling mechanism mediating the detrimental effects of the TGF- family? Among the various signaling mechanisms activated by TGF-1, the role of TAK-1 in mediating pathologic hypertrophy seems best established. TAK-1 is rapidly activated by TGF-1, and overexpression of TAK-1 in the heart causes cardiac hypertrophy and failure.17 Alternatively, the Smad-dependent mechanism may cooperatively mediate pathological hypertrophy in the presence of TAK-1 activation.13 In any case, it is possible that the Smad-independent pathway may determine whether each member of the TGF- superfamily mediates protective or detrimental functions in the adult heart. Interestingly, both ERKs and Akt, protective molecules for the heart, are activated by GDF15. In this regard, it would be interesting to confirm that TAK-1/p38 MAPK signaling is not actually activated by GDF15 in cardiomyocytes. Perspectives In summary, the studies reported by Xu et al7 and Kemph et al8 indicate that GDF15 is a promising cardioprotective agent against heart failure and I/R. A cautionary note is that GDF15 induces apoptosis in some cancer cells.18 Thus, the function of GDF15 may depend on the availability of type I and II receptors and/or Smads and concomitant activation of Smadindependent signaling mechanisms. Identifying the receptor 296 Circulation Research February 17, 2006 Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 Figure 2. Intracellular signaling pathways of TGF- superfamily members and their cardiac effects. Bold lines indicate putative GDF15activated pathways. Note that some Smads may mediate hypertrophy and apoptosis in the presence of additional signaling mechanisms and transcription factors. subtype, the underlying signaling mechanism, and further downstream targets of GDF15 should be useful for further elucidation of the cardioprotective mechanism in various pathological conditions. It is advisable that the long-term protective effects of GDF15 overexpression on cardiac function after MI should be confirmed using GDF15 overexpression mice. Recently, several diffusible molecules, whose expression is strongly upregulated by cardiac stresses, have been identified as powerful cardioprotective factors.19,20 Because multicellular organisms are known to acquire “stress resistance” through stress-induced upregulation of diffusible factors which not only protect the cells under stress but also alert surrounding cells to prepare for coming disasters, identifying such molecules through expression profile analyses will continue to be a fruitful approach for future drug discovery. Acknowledgments We thank Dr Stephen F. Vatner and Daniela Zablocki for critical reading of the manuscript. References 1. Shi Y, Massague J. Mechanisms of TGF-beta signaling from cell membrane to the nucleus. Cell. 2003;113:685–700. 2. Schultz Jel J, Witt SA, Glascock BJ, Nieman ML, Reiser PJ, Nix SL, Kimball TR, Doetschman T. TGF-beta1 mediates the hypertrophic cardiomyocyte growth induced by angiotensin II. J Clin Invest. 2002;109: 787–796. 3. Swynghedauw B. Molecular mechanisms of myocardial remodeling. Physiol Rev. 1999;79:215–262. 4. Li TS, Hayashi M, Ito H, Furutani A, Murata T, Matsuzaki M, Hamano K. Regeneration of infarcted myocardium by intramyocardial implantation of ex vivo transforming growth factor-beta-preprogrammed bone marrow stem cells. Circulation. 2005;111:2438 –2445. 5. Ikeuchi M, Tsutsui H, Shiomi T, Matsusaka H, Matsushima S, Wen J, Kubota T, Takeshita A. Inhibition of TGF-beta signaling exacerbates early cardiac dysfunction but prevents late remodeling after infarction. Cardiovasc Res. 2004;64:526 –535. 6. Izumi M, Fujio Y, Kunisada K, Negoro S, Tone E, Funamoto M, Osugi T, Oshima Y, Nakaoka Y, Kishimoto T, Yamauchi-Takihara K, Hirota H. Bone morphogenetic protein-2 inhibits serum deprivation-induced apoptosis of neonatal cardiac myocytes through activation of the Smad1 pathway. J Biol Chem. 2001;276:31133–31141. 7. Xu J, Kimball TR, Lorenz JN, Brown DA, Bauskin AR, Klevitsky R, Hewett TE, Breit SN, Molkentin JD. GDF15/MIC-1 functions as a protective and antihypertrophic factor released from the myocardium in association with SMAD protein activation. Circ Res. 2006;98:342–350. 8. Kempf T, Eden M, Strelau J, Naguib M, Willenbockel C, Tongers J, Heineke J, Kotlarz D, Xu J, Molkentin JD, Niessen HW, Drexler H, Wollert KC. Transforming growth factor-{beta} superfamily member growth-differentiation factor-15 protects the heart from ischemia/ reperfusion injury. Circ Res. 2006;98:351–360. 9. Bootcov MR, Bauskin AR, Valenzuela SM, Moore AG, Bansal M, He XY, Zhang HP, Donnellan M, Mahler S, Pryor K, Walsh BJ, Nicholson RC, Fairlie WD, Por SB, Robbins JM, Breit SN. MIC-1, a novel macrophage inhibitory cytokine, is a divergent member of the TGF-beta superfamily. Proc Natl Acad Sci U S A. 1997;94:11514 –11519. 10. Tan M, Wang Y, Guan K, Sun Y. PTGF-beta, a type beta transforming growth factor (TGF-beta) superfamily member, is a p53 target gene that inhibits tumor cell growth via TGF-beta signaling pathway. Proc Natl Acad Sci U S A. 2000;97:109 –114. Ago and Sadoshima 11. Brown DA, Breit SN, Buring J, Fairlie WD, Bauskin AR, Liu T, Ridker PM. Concentration in plasma of macrophage inhibitory cytokine-1 and risk of cardiovascular events in women: a nested case-control study. Lancet. 2002;359:2159 –2163. 12. Derynck R, Zhang YE. Smad-dependent and Smad-independent pathways in TGF-beta family signalling. Nature. 2003;425:577–584. 13. Euler-Taimor G, Heger J. The complex pattern of SMAD signaling in the cardiovascular system. Cardiovasc Res. 2006;69:15–25. 14. Wang J, Xu N, Feng X, Hou N, Zhang J, Cheng X, Chen Y, Zhang Y, Yang X. Targeted disruption of Smad4 in cardiomyocytes results in cardiac hypertrophy and heart failure. Circ Res. 2005;97:821– 828. 15. Masaki M, Izumi M, Oshima Y, Nakaoka Y, Kuroda T, Kimura R, Sugiyama S, Terai K, Kitakaze M, Yamauchi-Takihara K, Kawase I, Hirota H. Smad1 protects cardiomyocytes from ischemia-reperfusion injury. Circulation. 2005;111:2752–2759. 16. Sun Y, Zhou J, Liao X, Lu Y, Deng C, Huang P, Chen Q, Yang X. Disruption of Smad5 gene induces mitochondria-dependent apoptosis in cardiomyocytes. Exp Cell Res. 2005;306:85–93. TGF- Signaling in the Adult Heart 297 17. Zhang D, Gaussin V, Taffet GE, Belaguli NS, Yamada M, Schwartz RJ, Michael LH, Overbeek PA, Schneider MD. TAK1 is activated in the myocardium after pressure overload and is sufficient to provoke heart failure in transgenic mice. Nat Med. 2000;6:556 –563. 18. Liu T, Bauskin AR, Zaunders J, Brown DA, Pankhurst S, Russell PJ, Breit SN. Macrophage inhibitory cytokine 1 reduces cell adhesion and induces apoptosis in prostate cancer cells. Cancer Res. 2003;63: 5034 –5040. 19. McGrath MF, Kuroski de Bold ML, de Bold AJ. The endocrine function of the heart. Trends Endocrinol Metab. 2005;16:469 – 477. 20. Tao L, Gao E, Bryan NS, Qu Y, Liu HR, Hu A, Christopher TA, Lopez BL, Yodoi J, Koch WJ, Feelisch M, Ma XL. Cardioprotective effects of thioredoxin in myocardial ischemia and reperfusion: role of S-nitrosation. Proc Natl Acad Sci U S A. 2004;101:11471–11476. KEY WORDS: GDF15 䡲 TGF- superfamily 䡲 hypertrophy 䡲 heart failure 䡲 Smad 䡲 MAPK Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 GDF15, a Cardioprotective TGF-β Superfamily Protein Tetsuro Ago and Junichi Sadoshima Downloaded from http://circres.ahajournals.org/ by guest on June 16, 2017 Circ Res. 2006;98:294-297 doi: 10.1161/01.RES.0000207919.83894.9d Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2006 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/98/3/294 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/