Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Gene expression profiling wikipedia , lookup
Gene therapy of the human retina wikipedia , lookup
DNA vaccination wikipedia , lookup
Microevolution wikipedia , lookup
Frameshift mutation wikipedia , lookup
Nutriepigenomics wikipedia , lookup
Neuronal ceroid lipofuscinosis wikipedia , lookup
Epigenetics of neurodegenerative diseases wikipedia , lookup
Gene nomenclature wikipedia , lookup
Therapeutic gene modulation wikipedia , lookup
Artificial gene synthesis wikipedia , lookup
Protein moonlighting wikipedia , lookup
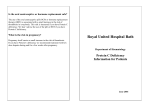
From www.bloodjournal.org by guest on June 16, 2017. For personal use only. Severe Perinatal Thrombosis in Double and Triple Heterozygous Offspring of a Family Segregating Two Independent Protein S Mutations and a Protein C Mutation By Caroline J. Formstone, Paula J. Hallam, Edward G.D. Tuddenham, Jennifer Voke, Mark Layton, Kypros Nicolaides, Ian M. Hann, and David N. Cooper Molecular genetic and phenotypic analyses were performed in a highly unusual case of combined protein S and protein C deficiency manifesting in a family in which a child had died perinatally from renal vein thrombosis. Antenatal diagnosis in a second pregnancy was initially performed by indirect restriction fragment length polymorphism (RFLP) tracking using a neutral dimorphism within the PROS gene and served t o exclude severe protein S deficiency. An umbilical vein blood sample at 22 weeks gestation showed isolated protein C deficiency. This pregnancy proceeded t o a fullterm delivery without thrombotic complications. Molecular genetic analysis of the PROC and PROS genes segregating in the family then yielded one PROCgene lesion in the father and two PROS gene lesions, one in each parent. These lesions were shown t o segregate with the respective deficiency states through the family pedigree. Analysis of DNA from paraffin-embedded liver tissue taken from the deceased child showed the presence of both PROS mutations, as well as the PROC mutation. Genotypic analysis of the second child showed a PROC mutation, but neither PROS mutation consistent with its possession of normal protein S levels and a lowlborderline protein C level. Antenatal diagnosis was then performed in a third pregnancy by direct mutation detection. However, although the fetus carried only the paternal PROS and PROC gene lesions, the child developed renal thrombosis in utero. It may be that a further genetic lesion at a third locus still remains t o be defined. Alternatively, the intrauterine development of thrombosis in this infant could have been caused, at least in part, by a transplacental thrombotic stimulus arising in the protein Sdeficient maternal circulation. This analysis may, therefore, serve as a warning against extrapolating too readily from genotype t o phenotype in families with a complex thrombotic disorder. 0 7996 by The American Society of Hematology. T Estimates of the prevalence of clinically symptomatic deficiencies of protein C in the general population lie between 1:16000 and 1:36000,’5.’6while the frequency of symptomatic protein S deficiency is 1:20000.’2Although most often found in the heterozygous state, severe homozygous or compound heterozygous deficiencies of both protein C‘”“ and protein SZ2-”have been reported and are usually associated with severe early onset venous thrombosis. The characterization of several severe forms of both protein CZ5and protein SZ6deficiencies at the DNA level has been initiated. We describe here the clinical features together with the labora- HE PROTEIN C anticoagulant pathway represents an important control mechanism in hemostasis. Protein C, a vitamin K-dependent glycoprotein and zymogen of a serine proteinase, is activated at the endothelial cell surface by the thrombidthrombomodulin complex and proteolytically cleaves and inactivates procoagulant factors Va and VIIIa. Protein S acts as a cofactor to activated protein C (APC) by enhancing the rate of inactivation of these Protein S also serves to regulate hemostasis via an APC-independent me~hanism.~.~ Approximately 60% of protein S in plasma is noncovalently complexed with C4b binding protein (C4bBP),’ while the remainder is unbound (‘free’). The interaction of functional free protein S with C4bBP abolishes the anticoagulant activity of the former.’ The protein C (PROC) gene resides on chromosome 2 and comprises 9 exons.9 The protein S (PROS) gene is located on chromosome 3, comprises 15 exons, and is closely linked to a highly homologous pseudogene.lo Hereditary deficiencies of both protein C and protein S are well-documented, and both are associated with an increased risk of venous thrombosis.” Together they account for between 6% and 10% of families with hereditary thrombophilia.” Two distinct types of hereditary protein C deficiency are recognized’? type I, the most common, is characterized by a parallel reduction in protein C activity and antigen levels, whereas type I1 exhibits a greater reduction in activity than antigen. The classification of protein S deficiency is complicated by the presence of C4bBP-bound protein S in plasma. However, three types have been distinguished phen~typically’~: type I deficiency is characterized by reduced total and free antigen levels together with reduced anticoagulant activity. In type I1 deficiency, protein S activity is reduced, although total and free antigen levels are normal, whereas in type 111 deficiency, the total protein S antigen level is normal, but free protein S antigen and activity are reduced. ’ Blood, Vol 87, No 9 (May 1). 1996: pp 3731-3737 From the Department of Biochemistry, Imperial College, London; Academic Unit of Medical and Community Genetics, Kennedy Galton Centre, Harrow; Haemostasis Research Group, Clinical Sciences Centre, Hammersmith Hospital, London; Haematology Department, Luton and Dunstable Hospital, Luton; Haematology Department, King’s College Hospital, London; Harris Birthright Research Centre for Fetal Medicine, King’s College Hospital, London; Haematology Department, Great Ormond Street Hospital for Children, London; and Institute of Medical Genetics, University oj Wales College of Medicine, Card18 UK. C.J.F., P.J.H., and D.N.C. were previously at Thrombosis Research Institute, London, UK. Submitted July 18, 1995; accepted December 6, 1995. Supported by the Thrombosis Research Trust, Charter plc, and the Sun-Life Assurance Co Lid. Address reprint requests to Paula J. Hallam, PhD, Academic Unit of Medical and Community Genetics, Kennedy Galton Centre, Level 8V, Northwick Park Hospital, Watford Rd, Harrow, Middlesex HA1 3UJ, UK. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact. 0 1996 by The American Society of Hematology. 0006-4971/96/8709-00$3.00/0 3731 From www.bloodjournal.org by guest on June 16, 2017. For personal use only. FORMSTONE ET AL 3732 Table 1. Phenotypic and Genotypic Data From Family Members Family Member PC Activity (NR 73-121) PC Antigen (NR 61-142) PROC Mutation PS Total (NR 77-100) PS Free (NR 81-113) 1.2 11.1 11.2 11.3 11.4 11.5 111.1 111.2 111.3 111.4 111.5 87 81 37 60 82 100 106 3t 85 76 59 128 88 60 64 109 125 76 16t 98 64 77 NT NT e NT NT NT NT e 82 134 74 106 38 94 114 24t 44 58 39 15 58 54 120 30 127 82 <lot 13 NT NT 31 4 PROS Mutation NT - + NT NT + + + +, Abbreviations: 0. Arg 169 Gln (PROO; D. Met 570 Thr (PROS); 2-bp deletion [codons 547/5481(PROS); NR, normal range for healthy adults; t, on warfarin treatment when tested; NT, not tested; -, no genetic lesion found. + + tory and molecular genetic analysis of a highly unusual family in which one PROC and two nonidentical PROS gene lesions are segregating. MATERIALS AND METHODS Family hisfory. The first child, 1V.I (Fig l), died at age 1 week from bilateral renal vein thrombosis. Although she showed no evidence of purpura fulminans, one kidney was fibrotic at postmortem with evidence of intrauterine thrombosis. The other kidney showed evidence of recent infarction with renal vein thrombosis. Thrombosis was also present in the major cerebral veins. Pretransfusion blood samples from IV.1 were not available for analysis. Several members of this English family had also experienced thrombotic manifestations and/or low levels of both protein C and protein S (Fig 1, Table 1). 1.2 experienced several episodes of phlebitis while 11.6 suffered a deep vein thrombosis after surgery and has also experienced a pulmonary embolism. 111.2, the propositus, experienced two ileofemoral thromboses as a teenager, the first at the age of 13 following traumatic injury sustained while playing football, the second at the age of 20, which was apparently spontaneous. He is currently on long-term warfarin prophylaxis. The mother of the deceased child (111.3) possessed levels of protein S consistent with an heterozygous type I deficiency state (Table I). Measured protein C and S values for the father (III.2) (Table 1) were not useful because this individual had received anticoagulant therapy as he initially presented with clinical symptoms. His father (11.2) exhibited both protein C and protein S deficiency phenotypes (types I1 and 111, respectively) (Table l). Although matemal (111.3) protein C levels appeared normal, several of her immediate relatives (11.3, III.4, and 111.5) possessed borderline normal protein C activity and/or antigen levels (Table 1). During a second pregnancy (IV.2), fetal blood sampling (cordocentesis) at 22 weeks gestation showed protein S activity and free protein S antigen levels of 29 U/dL (normal range [NR], 23 to 30) and 33 U/dL (NR, 35 to 41), respectively (Table 2), both of which were normal for gestational age. Protein C activity, however, was lower than normal for gestational age (5 U/dL, NR, 9.5 to 13.5). The pregnancy was uneventful and a clinically normal baby was born at 39 weeks gestation. At term, protein C activity was still low (8 U/dL, NR, 21 to 65), while total protein S antigen remained within the normal range (43 U/dL, NR, 20 to 64). Although protein S values were unchanged by 16 months of age, protein C antigen and activity levels were borderline normal (Table 2). It is unclear, however, why protein C activity and antigen levels are very similar in IV.2. This child is still healthy. A third pregnancy (IV.3) was monitored very carefully. Chorionic villus sampling was performed at 14 weeks gestation. Delivery was by emergency Caesarean section at 38 weeks due to decreased fetal movement. Cord blood taken at the time of delivery contained a protein C activity level of 4 U/dL [NR, 24 to 38 weeks gestation, fetuses, and neonates, 8.1 to 22.91;’ and a borderline normal protein C antigen level of 17 U/dL [NR day 1 (full-term), 17 to 531. Total and free protein S antigen levels were found to be 14 U/dL [NR day 1 (full-term), 17 to 531 and 2 U/dL [NR day 1 (full-term), 32 to 841, respectively, while protein S activity was 24 U/dL (NR, 55 to 119). A palpable kidney at 12 hours of age was investigated further by ultrasound imaging that showed left renal vein thrombosis, left adrenal hemorrhage, thrombosis in the inferior vena cava, and a thrombus in the bladder. Because protein C deficiency was felt to be his major problem, initial treatment was with intravenous fresh frozen plasma and heparin and then a few days later with protein C concentrate. His plasma protein C levels increased accordingly. A right atrial Hickman catheter was inserted at the age of 2 weeks for the regular administration of protein C concentrate and heparin. This was subsequently removed at the age of 6 weeks, protein C concentrate and heparin were withdrawn, and warfarin therapy commenced. The Intemational Normalized Ratio is being maintained between 3.0 and 3.5, and it is planned to continue this treatment indefinitely. At the time of writing, at the age of 9 months, there have been no further thrombotic episodes. The child i s thriving despite the functional loss of about 90% of his left kidney. Immunological assays. Protein C and protein S antigen levels (total and free) were assayed by standard enzyme-linked immunosorbent assay (ELISA) (Dako, High Wycombe, UK) using a rabbit polyclonal antibody. Protein S and protein C activities were measured using the Stago kit (Diagnostica Stago, Asnikres, France). DNA extracfion from parafin-embedded tissue. Only paraffinembedded liver tissue was available for DNA analysis from the deceased child, IV. 1. Under sterile conditions, sections were removed and transferred to 1.5 mL Eppendorf tubes, previously washed in 10 mmol/L HC1 followed by oven-drying. DNA extraction was performed using the procedure of L.S. Young (unpublished method): briefly, paraffin sections were incubated at room temperature for 5 minutes in 1 mL xylene (BDH, Poole, Dorset) and then centrifuged at 13,000 rpm for 10 minutes. The xylene was removed and the above procedure repeated. The resulting pellet was washed three times in ethanol and the final pellet dried overnight at 37°C. A total of 400 pL 1x polymerase chain reaction (PCR) buffer (Promega, Southampton, UK) together with 100 pg/mL proteinase K From www.bloodjournal.org by guest on June 16, 2017. For personal use only. 3733 COMBINED PROTEIN S AND PROTEIN C DEFICIENCY (GIBCO-BRL, Middlesex, UK) were added to the dried pellet, and the mixture incubated at 55°C for 1 hour followed by 95°C for 10 minutes. A control tube containing no paraffin section was treated in a similar manner. The resulting solutions were used as templates for PCR amplification. PROS gene: Pro626 polymorphism analysis. The alleles of the exon XV Pro626 polymorphism were determined at the level of both genomic DNA and mRNA (cDNA) by restriction fragment length polymorphism (RFLP) analysis as described.” PCWdirect sequencing analysis of exon-containing DNA fragments. Genomic DNA extraction from family members, DNA amplification, and PCWdirect sequencing were performed as des ~ r i b e d .The ~ ~ PROC . ~ ~ gene exon VI1 and the PROS gene exon XIV from the deceased child (IV. 1) were PCR amplified from paraffinembedded liver tissue DNA in tubes washed previously in 10 mmoV L HCI and oven-dried. PCR amplification was performed as des ~ r i b e d , 2but ~ * following ~~ the recommendations of Woodward et a13’; 20 pL of a 1: 10 dilution of both control and paraffin section samples were used for PCR amplification of PROC and PROS gene exons. DNA samples from IV.2 and IV.3 were derived from chorionic villus samples, cord blood, and venipuncture after birth. Reverse-transcription (RT) PCR analysis for the PROS gene. Platelets from 11.4 were separated from whole blood” and RNA extracted.” The specific reverse transcription of PROS mRNA and subsequent PCR amplification of cDNA fragments were performed as described.28 Screening for APC resistance and factor V Leiden. Activated protein C ( A X ) resistance assays and screening for the common factor V Leiden lesion (CGA -+ CAA converting Arg 506 to Gln) were performed essentially as d e ~ c r i b e d . ~ ~ . ~ ~ RESULTS Studies on the segregation of PROS gene Lesions by RFLP tracking and PCWdirect sequencing. Prior to the identification by PCWdirect sequencing analysis of the PROS gene lesions segregating in this family, indirect PROS RFLP analysis was performed to attempt a rapid antenatal exclusion of severe protein S deficiency in individual IV.2. Family members spanning four generations were typed for the CCA/ CCG (henceforth termed A and G) alleles of the neutral dimorphism at Pro626 in exon XV of the PROS gene.35 This dimorphism is detectable directly by restriction enzyme (BstXZ) cleavage of PCR-amplified exon XV. The segregation pattern of the Pro626 RFLP alleles in this family is shown in Fig 1. Both the maternal and paternal defective PROS alleles cosegregated with the Pro626 A allele. The possibility of severe protein S deficiency in IV.2 was excluded antenatally by the Pro626 RFLP analysis since the maternal A allele was absent in the fetal material (Fig 1). Pro626 RFLP data for individuals 1.2, 11.4, 11.6, III.2, and 111.3 have been presented previously.’8 This previous publication” also described the detection and characterization of two different inherited PROS gene lesions in exon XIV from certain members of this family. PCWdirect sequencing of the 15 exons and splice junctions of the PROS gene identified a Met570 Thr (ATG ACG) substitution in 111.2 and a short deletion (1908 del AC) in 111.3. The Met570 Thr substitution and the 2bp deletion were also detected in 11.2 and II.4, respectively.28For the purposes of this study, the presence or absence of the two PROS gene mutations in further family members was deter+ + + 1 I M I Adkkiw IV M AG AG Fig 1. Family pedigree. Semishaded symbols denote clinicalty affected individuals. A diagonal line through a symbol denotes indvidual deceased. 0 denotes proven carrier of the Argl69 Gin mutation and respectively, denote within exon VI1 of the PROC gene. proven carriers of the Met570 Thr mutation and the 2-bp deletion et position 1908, both of which lie within axon XIV of the PROSgene. AA and GO, respectively, denote homozygority for the CCA and CCG alleles at Pro626 of the PROS gene, while AG denotes heterozygosity. NT denotes PROS gene not analyzed by PCR/dirat sequencing. Data on allelic exclusion for PROS mRNA also provided for Individuals 11.4 and 111.3. Individual 111.2 was on warfarin prophylaxis. - +, - mined by PCWdirect sequencing of PROS exon XIV in these individuals (Fig 1, Table 1). Additional evidence for the Met570 Thr substitution being the pathological lesion in the family was provided by sequence analysis of exon XIV from 50 controls (of Caucasian origin with no history of venous thrombosis), which failed to detect another example of the Met570 Thr substitution. This mutation does not appear to be a common polymorphism. Moreover, its presence is associated with the clinical phenotype in the family through two generations (Fig 1). The maternal 2-bp deletion was detected in individuals 111.4, III.5, and IV.1, but not in 1.2 or IV.2. Thus, the deceased child (IV.l) possessed both paternal and maternal PROS gene lesions (Fig 1, Table 2). Cord blood DNA was used to PCR amplify exon XIV from the second child (IV.2). Neither PROS gene lesion was detected in IV.2, an observation consistent with (1) the normal levels of total and free protein S noted in this child and (2) the absence of the maternal A allele demonstrated previously by antenatal Pro626 RFLP tracking analysis (see above). In the case of the third child (IV.3), antenatal screening for the presence of PROS gene mutations showed only the paternal Met570 -+ Thr mutation, the maternal PROS gene lesion being absent. Genotypic and phenotypic data obtained from the siblings in generation IV are summarized in Table 2. It was previously demonstrated that individual III.3, who was heterozygous A/G for the Pro626 PROS RFLP at the genomic DNA level, exhibited the loss of the A allele at the mRNA level [“allelic e~clusion”].’~The A allele was in phase with the 2-bp PROS gene deletion identified in this individual. Loss of the PROS mRNA species bearing this mutation was consistent with her type I protein S deficiency state. The absence of the 2-bp deletion in II.4cDNA (Fig 1) was also demonstrated by PCWdirect sequencing of plateletderived cDNA from this individual. The demonstration of the loss of the A allele for the Pro626 RFLP by PCWdirect -+ -+ From www.bloodjournal.org by guest on June 16, 2017. For personal use only. 3734 FORMSTONE ET AL Table 2. Phenotypic Data From Siblings IV.l, IV.2, and IV.3 Family Member IV.1 Weeks GestationIAge 1 wk IV.2 22/40 IV.3 38/40 (term) 16 m o 38/40 (term) PC Activity (U/dL) (NR) PC Antigen WdL) (NR) PROC Mutation 23 (8.1-22.91 23 (17-53) a a 5 (9.5-13.5) 8 (21-65) 66 (70-140) 4 (8.1-22.9) PS Activity (U/dL) (NRI PS Antigen WdL) (NR) 29 (23-30) 28++ (17-53) total 16++ (32-84) free 33 (35-41) free PROS Mutation a+ - 43 (20-64) total 67 (61-142) 17 (17-53) 88 (55-119) 24 (55-119) a 14 (17-53) total 2 (32-84) free Abbreviations: ++, Phenotypic analysis performed posttransfusion of fresh plasma. No pretransfusion plasma available for phenotypic analysis; NR, normal ranges for gestational age/age of child. sequencing and RFLP analysis confirmed “allelic exclusion” in 11.4. Direct detection of the pathological lesion in the PROC gene. PCWdirect sequencing of all nine exons and splice junctions of the PROC genes of individual 111.2 yielded only one deviation from the wild-type sequence: a heterozygous CGG CAG transition in exon VII, which predicts an arginine to glutamine substitution at amino acid residue 169. The authenticity of this lesion was confirmed by sequencing the antisense DNA strand. This substitution was also found in individuals 11.2, IV.2, IV.3, and the deceased child 1V.I (Fig 1) and, therefore, segregates with the protein C deficiency state through the family. By contrast, PCWdirect sequencing of all nine exons and splice junctions of the PROC genes of individual 111.3 did not yield any deviation from the wild-type sequence. Factor V Leiden screening. For individuals 111.2, 111.3, and IV.3, the presence of APC resistance3‘ was excluded by direct screening for the common factor V Leiden mutation and/or by means of the APC resistance assay. -+ DISCUSSION R E P tracking was partially successful in that severe protein S deficiency was rapidly excluded in individual IV.2 during the second trimester. PCWdirect sequencing of PROC and PROS genes from family members was then employed to detect and characterize the underlying pathological lesions. Three mutations were found, one in the PROC gene and two in the PROS gene. The PROC mutation identified (Arg169 Gln) has been reported at least three times previously in individuals with type I1 protein C defi~iency.’~ Its location within the Arg169-Leu170 activation site of protein C explains its association with a type I1 deficiency state. The detection and characterization of the PROS gene lesions has been reported previously.28In that study, we confirmed the authenticity of both lesions by sequencing the antisense DNA strand. In addition, no further deviations from the wildtype sequence were present in any of the other 14 exons and splice junctions of the PROS gene.28The 2-bp PROS gene deletion generated an in-frame TAA termination codon just three amino acids C-terminal to the lesion, and this accounts both for the type I protein S deficiency observed in maternal family members and for the allelic exclusion noted in 11.4 and 111.3. The paternal Met570 Thr substitution occurred in a residue that is conserved in both rabbita and bovine4’ protein S and in the homologous human protein, sex hormone binding globulin!’ The amino acid environment of Met570 appears hydrophobic, which suggests that this region is internal to the protein. The present study provided further support for the conclusion that Met570 Thr is the pathological mutation by demonstrating its absence in 100 normal alleles. In addition, the presence of this PROS gene lesion is associated with the clinical phenotype in two generations of this kindred. We have previously suggested that the Met570 Thr substitution may be associated with type 111 protein S deficiency.28Total and free protein S antigen levels from individual IV.3 are also consistent with a type 111 deficiency. However, the biochemical characterization of an in vitro-expressed protein should establish whether the Met570 -+ Thr substitution is indeed a disease-causing mutation and possibly the pathological mechanism underlying this disorder. The genotypic data from family members broadly confirmed our initial assumptions made regarding the number and nature of the gene defects and their pattern of inheritance. The deceased child’s father (111.2) had correctly been predicted to be doubly heterozygous for mutations in both + + Few families with a thrombotic diathesis and two distinct prothrombotic defects have been reported to date.37However, the recent discovery of the common factor V Leiden variant (present in between 2% and 7% of individuals in European populations) has shown that combined deficiency states may not be as rare as was originally Two cases of a triple deficiency have been reported from a single Canadian kindred: one individual was deficient in antithrombin 111, protein C, and heparin cofactor 11, and the other was deficient in antithrombin 111, protein S, and heparin cofactor II.38 Such cases are, however, exceptionally rare, and none have been characterized at the DNA level. We report here the molecular genetic analysis of, and antenatal diagnosis in, a family with combined protein C and protein S deficiency in which three different gene defects are segregating. The phenotypic data collected from family members indicated the complexity of antenatal diagnosis and the difficulty in counselling the parents of the deceased child in subsequent pregnancies. Since phenotypic data may be considered to be particularly unreliable in the case of fetal blood sampling owing to the low plasma protein levels at early gestational age,27molecular genetic analysis was employed in the hope of improving diagnostic accuracy. .--) -+ From www.bloodjournal.org by guest on June 16, 2017. For personal use only. 3735 COMBINED PROTEIN S AND PROTEIN C DEFICIENCY PROC and PROS genes and her mother (111.3) to be heterozygous for a PROS mutation. The deceased child was shown to have possessed all three gene lesions segregating in this family and was thus compound heterozygous for protein S deficiency and heterozygous for protein C deficiency. This explanation for the clinical severity manifested by IV.1 suggested that predictions regarding clinical severity might be possible on the basis of genotype in other family members. This appears to be the case at least for the second child, IV.2, who is asymptomatic. She possesses the PROC gene lesion, but neither PROS mutation. Fetal and neonatal assays for IV.2 are consistent with the genotypic data, but her protein C activity level at age 16 months fell just outside the normal range for her age. Some considerable overlap between plasma protein C levels exhibited by heterozygotes and normals has been and IV.2 may represent another example of this phenomenon. Antenatal diagnosis was performed on a third child (IV.3) who was found to be heterozygous for the paternal PROS gene lesion, but lacked the maternal PROS gene lesion. That IV.3 also possessed the PROC gene lesion was only established after birth owing to the time required to detect and characterize this lesion. Since this child’s father (111.2) and grandfather (11.2) possessed both PROC and PROS gene lesions and were either clinically normal or only affected after childhood, it was reasoned that there should not be any thrombotic manifestations in the neonatal period. The inaccuracy of this prognosis rapidly became apparent when the child suffered severe early onset venous thrombosis. Phenotypic data from individual IV.3, derived from cord blood and taken at the time of delivery, were consistent with his possession of the paternal PROS gene lesion (Table 2). His protein S activity was reduced to below 50% of the normal range for age (NR, 55 to 119). In addition, the protein S antigen levels (total and free) of IV.3 suggested that he manifested a similar type of protein S deficiency to his grandfather (11.2) [type 1111. The protein C phenotype of this child (type I1 deficiency) was also similar to that of 11.2. The presence of protein C deficiency in IV.3 was confirmed by the detection of the Arg169 Gln mutation in his PROC gene. Despite the wealth of clinical, phenotypic, and genetic data generated by this study, prognostic accuracy was still limited. One possible explanation for our inability to predict the clinical severity of individual IV.3 would be the presence of a second PROC gene lesion in both 111.3 and IV.3. Although 111.3 possessed normal levels of protein C activity and antigen, several of her relatives exhibited protein C levels, which were borderline normal (11.3, 111.4, and 111.5). However, sequencing of the PROC genes from both 111.3 and IV.3 failed to detect another lesion. The low protein C values apparent in 11.3, 111.4 and 111.5 could in principle be attributable to another lesion in the PROC gene. There is no evidence to suggest, however, that the low protein C levels in 11.3 are heritable. 11.3 is unrelated to 111.4, and 111.5 who are full sisters and the remaining maternal family members (1.2, 11.4, 11.6, and 111.3) exhibit normal protein C levels. No information is available on indi- - vidual 11.5 (Fig 1: father of 111.4 and 111.5). Since no PROC gene lesion was identified in 111.3, further analysis of the PROC gene from individuals 11.3,111.4,and 111.5 was deemed unnecessary for the purposes of this diagnostic analysis. Alternatively their protein C deficiency phenotype may have been acquired. The severe clinical phenotype manifested by IV.3 could also be explained by a further genetic lesion at a third locus (possibly as yet unknown); the presence of the relatively common factor V Leiden lesion was, however, excluded. Another possible explanation is that the doubly heterozygous fetus, IV.3, was being carried by a mother (111.3) who was herself known to be predisposed to thrombotic events by virtue of her possession of a PROS gene lesion. Exposure of the fetus to a potentially prothrombotic intrauterine environment might have served as a trigger for the early development of thrombotic symptoms. Two further anomalies were encountered in our attempts to correlate genotype with phenotype in this family. Firstly, individual 11.6 is clinically symptomatic yet her protein C and protein S levels are well within the normal range. This could conceivably be explained by the presence of another lesion in an as yet unidentified gene acting as an additional risk factor. Alternatively, her thrombosis may have been triggered by the acquired deficiency of an as yet unidentified anticoagulant factor. Secondly, while individual 1.2 is clinically symptomatic (she also possesses a very low free protein S level and bears the PROS Pro626 A allele associated with the type I protein S deficiency state), we were unable to detect the 2-bp deletion within a sample of her lymphocyte DNA. The absence of the PROS gene deletion in 1.2 may indicate de novo mutation in her germline giving rise to the lesion carried by her daughter 11.4 and subsequently transmitted through the pedigree. Because neither phenotypic data nor blood samples were available from her father (Ll), the possibility that the lesion was passed down from him cannot be excluded. An intragenic recombination event occurring between the mutation and the polymorphic marker at codon 626 is unlikely, however, as these two sites are separated by only 556 bp. Although highly unusual in terms of its complexity, this analysis and diagnosis should thus serve as a warning against extrapolating too readily from genotype to phenotype in kindreds with a multifactorial disorder, such as venous thrombosis. Clearly, the considerable clinical and phenotypic variability evident from this analysis must be taken into account in counselling families as complex as the one illustrated here. ACKNOWLEDGMENT We thank Lawrence S. Young for provision of the protocol for DNA extraction from paraffin-embedded tissue, Elaine Jenkins and Jane Clark for performing fetal coagulation studies, and Dan Thompson and Michael Chapple for clinical referral and liaison. REFERENCES 1. Dahlback B, Stenflo J: A natural anticoagulant pathway: Pro- teins C, s, C4b-binding protein and thrombomodulin, in Bloom AL, From www.bloodjournal.org by guest on June 16, 2017. For personal use only. 3736 Forbes CD, Thomas DP, Tuddenham EGD (eds): Haemostasis and Thrombosis (ed 3). Edinburgh, Scotland, Churchill Livingstone, 1994, p 671 2. Dahlback B: Protein S and C4b-binding protein: Components involved in the regulation of the protein C anticoagulant system. Thromb Haemost 66:49, 1991 3. Shen L, Dahlback B: Factor V and protein S as synergistic cofactors to activated protein C in degradation of factor VIIIa. J Biol Chem 269:18735, 1994 4. Heeb MJ, Mester RM, Tans G, Rosing J, Griffin JH: Binding of protein S to factor Va associated with inhibition of prothrombinase that is independent of activated protein C. J Biol Chem 268:2872, 1993 5. Heeb MJ, Rosing J, Bakker HM, Femandez JA, Tans G, Griffin JH: Protein S binds to and inhibits Factor Xa. Proc Natl Acad Sci USA 91:2728, 1994 6. Koppelman SJ, Hackeng TM, Sixma JJ, Bouma BN: Inhibition of the intrinsic Factor X activating complex by protein S: Evidence for a specific binding of protein S to factor VIII. Blood 86:1062, 1985 7. Dahlback B, Stenflo J: High molecular weight complex in human plasma between vitamin K-dependent protein S and complement component C4b-binding protein. Proc Natl Acad Sci USA 78:2512, 1981 8. Dahlback B: Inhibition of protein Ca cofactor function of human and bovine protein S by C4b-binding protein. J Biol Chem 26 1:12022, 1986 9. Plutzky J, Hoskins JA, Long GL, Crabtree GR: Evolution and organization of the human protein C gene. Proc Natl Acad Sci USA 83546, 1986 IO. Schmidel DK, Tatro AV, Phelps LG, Tomczak JA, Long GL: Organization of the human protein S genes. Biochemistry 29:7845, 1990 11. Henkens CMA, van der Meer J, Hillege JL, van der Schaaf W, Bom VJJ, Halie MR: The clinical expression of hereditary protein C and protein S deficiency: A relation to clinical thrombotic risk factors and to levels of protein C and S? Blood Coagul Fibrinolysis 4555, 1993 12. Bertina R: Prevalence of hereditary thrombophilia and the identification of genetic risk factors. Fibrinolysis 2:7, 1988 (Suppl 2) 13. Bertina RM, Broekmans AW, Krommeuhaevan ESC, van Wijngaarden A: The use of a functional and immunologic assay for plasma protein C in the study of the heterogeneity of congenital protein C deficiency. Thromb Haemost 5 1 :I , 1984 14. Scientific and Standardisation Committee of the International Society of Thrombosis and Haemostasis Subcommittee on protein C and protein S, Miinchen, July 1992 15. Broekmans AW, Veltkamp JJ, Bertina RM: Congenital protein C deficiency and venous thromboembolism. New Engl J Med 309:340, 1983 16. Gladson CL, Scharrer I, Hach V, Beck KH, Griffin JH: The frequency of type 1 heterozygous protein S and protein C deficiency in 141 unrelated young patients with venous thrombosis. Thromb Haemost 59:18, 1988 17. Branson HE, Kaze J, Marble R, Griffin JH: Inherited protein C deficiency and coumarin responsive chronic relapsing purpura fulminans in a newbom infant. Lancet 2.1 165, 1983 18. Marlar RA, Montgomery RR, Broekmans AW: Diagnosis and treatment of homozygous protein C deficiency. J Pediatr 114528, 1989 19. Seligsohn U, Berger A, Abend M, Rubin L, Attias D, Zivelin A, Rapaport SI: Homozygous protein C deficiency manifested by massive thrombosis in the newbom. New Engl J Med 310:559, 1984 FORMSTONE ET AL 20. Marciniak E, Wilson HD, Marlar RA: Neonatal purpura fulminans: A genetic disorder related to the absence of protein C i n blood. Blood 65:15, 1985 21. Manco-Johnson MJ, Marlar RA, Jacobson LJ, Hays T, Waraday BA: Severe protein C deficiency in newborn infants. J Pediatr 113:359, 1988 22. Mahasandana C, Suvatte V, Marlar RA, Manco-Johnson MJ, Jacobson LJ, Hathaways WE: Neonatal purpura fulminans associated with homozygous protein S deficiency. Lancet 335:61, 1990 23. Pegelow CH, Ledford M, Young J, Zilleruelo G: Severe protein S deficiency in a newborn. Pediatrics 89:674, 1992 24. Marlar RA, Neumann A: Neonatal purpura fulminans due to homozygous protein C or protein S deficiency. Seinin Thromb Hrmost 16:299, 1990 25. Reitsma PH, Bernardi F, Doig RG, Gandrille S, Greengard JS, Ireland M, Lind B, Long GL, Poort SR, Saito H, Sala N, Witt I, Cooper DN: Protein C deficiency: A database of mutations, 1995 update. Thromb Haemost 73:876, 1995 26. Gomez E, Ledford MR, Pegelow CH, Reitsma PH, Bertina RM: Homozygous protein S deficiency due to a one base pair deletion that leads to a stop codon in exon 111 of the protein S gene. Thromb Haemost 7 I :723, I994 27. Melissari E, Nicolaides KH, Scully MF, Kakkar VV: Protein S and C4b-binding protein in fetal and neonatal blood. Br J Haematol 70:199, 1988 28. Formstone CJ, Wacey AI, Berg L-P, Rahman S, Bevan D, Rowley M, Voke J, Bernardi F, Legnani C, Simioni P, Girolami A, Tuddenham EGD, Kakkar VV. Cooper DN: Detection and characterization of seven novel protein S (PROS) gene lesions: Evaluation of RT-PCR as a mutation screening strategy. Blood 86:2623, 1995 29. Hallam PJ, Wacey AI, Manucci PM, Legani C, Kiihnau W. Krawczak M, Kakkar VV, Cooper DN: A novel missense mutation (Thr 176 + Ile) at the putative hinge of the neo N-terminus of activated protein C. Hum Genet 95:447, 1995 30. Woodward SR, Weyward NJ, Bunnell M: DNA sequence from Cretaceous period bone fragments. Science 266: 1229, 1994 3 1. Ginsberg D, Konkle BA, Gill JC, Montgomery RR, Bockenstedt PL, Johnson TA, Yang AY: Molecular basis of human von Willebrand disease: Analysis of platelet von Willebrand factor mRNA. Proc Natl Acad Sci USA 86:3723, 1989 32. Chomczynski P, Sacchi N: Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal Biochem 162:156, 1987 33. Bertina RM, Koeleman BPC, Koster T, Rosendal FR, Dirren RJ, de Ronde H, van der Velden PA, Reitsma PH: Mutation in the blood coagulation factor V associated with resistance to activated protein C. Nature 369:64, 1994 34. Hallam PJ, Millar DS, Krawczak DS, Krawczak M, Kakkar VV, Cooper DN: Population differences in the frequency of the factor V Leiden variant among people with clinically symptomatic protein C deficiency. J Med Genet 32543, 1995 35. Diepstraten CM, Ploos van Amstel HK, Reitsma PH, Bertina RM: A CCA/CCG neutral dimorphism in the codon for Pro626 of the human protein S gene PS alpha (PROSI). Nucleic Acids Res 19:5091, 1991 36. Svensson PJ, Dahlback B: Resistance to activated protein C is a basis for venous thrombosis. New Engl J Med 330:517, 1994 37. Jobin F, Vu L, Lessard M: Two cases of inherited triple deficiency in a large kindred with thrombotic diathesis and deficiencies of antithrombin 111, heparin cofactor 11, protein C and protein S. Thromb Haemost 66:295, 1991 38. Koeleman BPC, Reitsma PH, Allaart CF, Bertina RM: Acti- From www.bloodjournal.org by guest on June 16, 2017. For personal use only. COMBINED PROTEIN S AND PROTEIN C DEFICIENCY vated protein C resistance as an additional risk factor for thrombosis in protein C-deficient families. Blood 84:1031, 1994 39. Van Boven HH, Reitsma PH, Rosendaal FR, Briet E, Vandenbroucke JP, Bayston TA, Chowdhury V, Bauer K, Scharrer I, Lane DA: Interaction of factor V Leiden with inherited antithrombin deficiency. Blood Coagul Fibrinolysis 6:153, 1995 40. He X, Dahlback B: Molecular cloning, expression and functional characterization of rabbit anticoagulant vitamin K-dependent protein S. Eur J Biochem 217:857, 1993 41. Dahlback B, Lundwall A, Stenflo J: Primary structure of bovine vitamin K-dependent protein S. Proc Natl Acad Sci USA 83:4199, 1986 42. Gershagen S, Fernlund P, Lundwall A: A cDNA coding for 3731 human sex hormone-binding globulin. Homology to vitamin K-dependent protein S. FEBS Lett 220:129, 1987 43. Allaart CF. Poort SR, Rosendaal FR, Reitsma PH, Bertina RM, Briet E: Increased risk of venous thrombosis in carriers of hereditary protein C deficiency defect. Lancet 341: 134, 1993 44. Pabinger I, Allaart CF, Hermans J, Briet E, Bertina RM, Conard J, Hach-Wunderle V, Kemkes-Matthes B, Mannucci PM, Sala N, Scharrer I, Shulman S, Tripodi A: Hereditary protein Cdeficiency: Laboratory values in transmitters and guidelines for the diagnostic procedure. Thromb Haemost 68:470, 1992 45. Montgomery RR, Scott JP: Hemostasis: Diseases of the fluid phase, in Nathan DG, Oski FA (eds): Hematology of Infancy and Childhood (ed 4). Philadelphia, PA, Saunders, 1992, p 1605 From www.bloodjournal.org by guest on June 16, 2017. For personal use only. 1996 87: 3731-3737 Severe perinatal thrombosis in double and triple heterozygous offspring of a family segregating two independent protein S mutations and a protein C mutation CJ Formstone, PJ Hallam, EG Tuddenham, J Voke, M Layton, K Nicolaides, IM Hann and DN Cooper Updated information and services can be found at: http://www.bloodjournal.org/content/87/9/3731.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.