Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Signal transduction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuroscience in space wikipedia , lookup
Molecular neuroscience wikipedia , lookup
End-plate potential wikipedia , lookup
Caridoid escape reaction wikipedia , lookup
Central pattern generator wikipedia , lookup
Electromyography wikipedia , lookup
Neuromuscular junction wikipedia , lookup
Synaptogenesis wikipedia , lookup
Stimulus (physiology) wikipedia , lookup
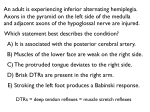
Motor Function Reflexes Reflexes are involuntary and relatively stereotyped responses to specific stimuli. Afferent nerve fibers conduct the impulses generated by activated receptors to neurons in the central nervous system, which fire impulses that are then transmitted through efferent nerve fibers to the cells, muscles, or organs that carry out the reflex response. The pathway as a whole is known as the reflex arc. Receptors are found at the origin of all sensory pathways—in the skin, mucous membranes, muscles, tendons, and periosteum, as well as in the retina, inner ear, olfactory mucosa, and taste buds. A reflex response may involve the somatic musculature or the internal organs. Most reflexes are relatively independent of the state of consciousness. An interruption of the reflex arc at any point weakens or abolishes the reflex. Intrinsic reflexes are those whose receptors and effectors are located in the same organ (e. g., the quadriceps reflex), while the receptors and effectors of extrinsic reflexes are in different organs (e. g., the oculovestibular reflex). Reflexes are important for normal function (e. g., for postural control and goal-directed movement), and an impaired reflex is an important objective finding in clinical neurological examination. Intrinsic Muscle Reflexes (Phasic Stretch Reflexes, Tendon Reflexes) 40 Intrinsic muscle reflexes are triggered by stretch receptors within the muscle (annulospiral nerve endings of muscle spindles). The impulses generated at the receptors are conveyed via afferent fast-twitch Ia fibers to spinal alpha-motor neurons, whose efferent α1 processes excite the agonistic muscle of an opposing muscle pair. The antagonistic muscle is simultaneously inhibited by spinal interneurons. The resulting muscle contraction relaxes the muscle spindles, thereby stopping impulse generation at the stretch receptors. The spinal reflex arc is also under the influence of higher motor centers. Abnormal reflex responses imply an abnormality of the musculature, the reflex arc, or higher motor centers. The most important reflexes in clinical diagnosis are the biceps (C5–C6), brachioradialis (C5–C6), triceps (C7–C8), adductor (L2–L4), quadriceps (L2/3–L4), posterior tibial (L5), and Achilles (S1–S2) reflexes. Extrinsic Reflexes Intrinsic muscle reflexes, discussed above, are monosynaptic, but extrinsic reflexes are polysynaptic: between their afferent and efferent arms lies a chain of spinal interneurons. They may be activated by stimuli of various types, e. g., muscle stretch, touch on the skin (abdominal reflex) or cornea (corneal reflex), mucosal irritation (sneezing), light (eye closure in response to a bright flash), or sound (acoustic reflex). The intensity of the response diminishes if the stimulus is repeated (habituation). Because they are polysynaptic, extrinsic reflexes have a longer latency (stimulus-to-response interval) than intrinsic reflexes. Some important extrinsic reflexes for normal function are the postural and righting reflexes, feeding reflexes (sucking, swallowing, licking), and autonomic reflexes (p. 110). The flexor reflex is triggered by noxious stimulation, e. g., from stepping on a tack. Excitatory interneurons activate spinal cord alpha-motor neurons, which, in turn, excite ipsilateral flexor muscles and simultaneously inhibit ipsilateral extensor muscles via inhibitory interneurons. Meanwhile, the contralateral extensors contract, and the contralateral flexors relax. The response does not depend on pain, which is felt only when sensory areas in the brain have been activated, by which time the motor response has already occurred. This spinal reflex arc, like that of the intrinsic muscle reflexes, is under the influence of higher motor centers. Abnormalities of the extrinsic reflexes imply an interruption of the reflex arc or of the corticospinal tracts (which convey impulses from higher motor centers). Some clinically important extrinsic reflexes are the abdominal (T6– T12), cremasteric (L1–L2), bulbocavernosus (S3– S4), and anal wink (S3–S5) reflexes. Reflexes that can be elicited only in the diseased state are called pathological reflexes. Pathological reflexes indicating dysfunction of the pyramidal (corticospinal) tract include the Babinski sign (tonic dorsiflexion of the great toe on stimulation of the lateral sole of the foot), the Gordon reflex (same response to squeezing of the calf muscles), and the Oppenheim reflex (same response to a downward stroke of the examiner’s thumb on the patient’s shin). Rohkamm, Color Atlas of Neurology © 2004 Thieme All rights reserved. Usage subject to terms and conditions of license. Reflexes Symbol 0 Can only be elicited by maneuvers (e.g., Jendrassik maneuver) + _ Diminished Normal intensity Heightened Persistent clonus 1 2 3 4 Extensor muscle Reflex response (Proprioceptive muscle reflex) Afferent (Ia) fiber Efferent fiber (excitatory) Efferent fiber (inhibitory) Flexor muscle Pseudounipolar nerve cells in spinal ganglion Supraspinal control (inhibitory) Afferent fiber Proprioceptive (intrinsic) muscle reflex Motor Function Reflex response Absent, cannot be elicited by maneuvers Efferent to extensors Annulospiral ending of muscle spindle Extensor Excitatory synapse Efferent fibers to contralateral extensors and flexors Interneuron Flexor Inhibitory synapse Efferent fibers to ipsilateral flexors and extensors Efferent to flexors Afferent (Ia) fiber Free ending of afferent fiber (pain, temperature) Supraspinal control (inhibitory) Interneurons Pressure receptor (Vater-Pacini corpuscle) Afferent fiber Fibers to contralateral side of commissural cell Inhibitory synapse Excitatory synapse Extrinsic muscle reflex Extensor muscle Rohkamm, Color Atlas of Neurology © 2004 Thieme All rights reserved. Usage subject to terms and conditions of license. Flexor muscle 41