Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Causes of transsexuality wikipedia , lookup
Externalizing disorders wikipedia , lookup
Neuroplasticity wikipedia , lookup
Neuropsychology wikipedia , lookup
Brain morphometry wikipedia , lookup
Clinical neurochemistry wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Persistent vegetative state wikipedia , lookup
Neurogenomics wikipedia , lookup
Visual selective attention in dementia wikipedia , lookup
Emotional lateralization wikipedia , lookup
Emergency psychiatry wikipedia , lookup
Biology of depression wikipedia , lookup
Aging brain wikipedia , lookup
Dual consciousness wikipedia , lookup
Abnormal psychology wikipedia , lookup
History of neuroimaging wikipedia , lookup
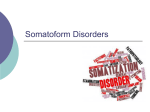
Araştırmalar / Original Papers A Volumetric MRI Analysis of Hypochondriac Patients Murad Atmaca1, Semih Sec2, Hanefi Yildirim3, Alperen Kayali4, Sevda Korkmaz2 ÖZET: Hipokondriak hastalarda volümetrik MRG analizi Hipokondriak hastalarda şu ana kadar gerçekleştirilmiş volümetrik manyetik rezonans görüntüleme (MRG) çalışması bulunmamaktadır. Bu çalışmada, bu hasta grubunda orbito-frontal korteks (OFK), anteriyor singulat, kaudat ve talamus hacimlerini değerlendirmeyi amaçladık. Onaltı hasta ve kontrolde OFK, anteriyor singulat, kaudat ve talamus hacimleri T1-ağırlıklı koronal MRG imajları ile 1.5 mm kalınlıklı kesitlerle değerlendirildi. Hipokondriak hastalar daha küçük sol ve sağ OFK ve daha büyük sol talamus hacimlerine sahipti. Kaudat ve anteriyor singulat hacimleri açısından gruplar arasında farklılık yoktu. Hamilton Depresyon Ölçme Skalası (HDRS) skorları ölçülen herhangi bir parametre ile ilişkili değildi. Hastalık başlangıç yaşı sol ve sağ OFK ile ilişkiliydi. Hastalık süresi de sol OFK ve sol talamusla anlamlı korelasyon gösterdi. Sonuç olarak, bu morfometrik çalışma, hipokondriyazisli hastaların daha küçük sol ve sağ OFK ve daha geniş sol talamus hacimlerine sahip olduğunu ortaya koymuştur. Bütün bunlar sonucunda, bulgularımız OFK ve talamusun hipokondriyazis patofizyolojisinde önemli bir yere sahip olabileceğini düşündürmektedir. Anahtar sözcükler: MRG, Volümetrik, Hipokondriyazis, Anteriyor singulat, OFK, Talamus, Kaudat Klinik Psikofarmakoloji Bülteni 2010;20:293-299 ABSTRACT: A volumetric MRI analysis of hypochondriac patients No volumetric brain magnetic resonance imaging (MRI) study has been performed in hypochondriac patients to date. In the present study, we aimed to volumetrically evaluate the orbito-frontal cortex (OFC), anterior cingulate, caudate nucleus, and thalamus. The volumes of the OFC, thalamus, caudate nucleus, and anterior cingulate cortex were measured in 16 treatment-naive hypochondriac patients and 16 healthy control subjects. Volumetric measurements were made with T1-weighted coronal MRI images, with 1.5-mm-thick slices, at 1.5T and were done blindly. Hypochondriac patients had significantly smaller mean left and right OFC, and greater left but not right thalamus volumes compared with healthy controls. There was no difference in regard to caudate and anterior cingulate volumes for either side between groups. The Hamilton Depression Rating Scale (HDRS) scores were not associated with any volumetric parameter studied. Age at onset showed a significant relationship to left OFC, and left thalamus volumes. Duration of illness also exhibited a significant association with left OFC, and left thalamus volumes. In conclusion, this morphometric MRI study showed that patients with hypochondriasis had smaller left and right OFC and significantly greater left thalamus volumes compared to healthy controls. Taken together, our findings suggest that abnormalities in the OFC and thalamus seem to play an important role in the pathophysiology of hypochondriasis. Key words: MRI, Volumetric, hypochondriasis, Anterior cingulate, OFC, Thalamus, Caudate Bulletin of Clinical Psychopharmacology 2010;20:293-299 INTRODUCTION Hypochondriasis is defined as preoccupation with fears of having, or the idea that one has, a serious disease based on one’s misinterpretation of bodily symptoms. The main characteristics of hypochondriasis are seeking repeated physical examinations, diagnostic tests, and reassurance from medical professionals; seeking reassurance from friends and family about physical symptoms and doing extensive research on the disease, my means such as using the Internet or reading medical journals. Hypochondrasis is currently classified as a somatoform disorder in DSMIV; however, it has some important similarities with Professor of Psychiatry, 2Resident of Psychiatry, Firat University School of Medicine Department of Psychiatry, Elazig-Turkey 3 Associate Professor of Radiology, 4Resident of Radiology, Firat University School of Medicine Department of Radiology, Elazig-Turkey 1 Yazışma Adresi / Address reprint requests to: Murad Atmaca, M.D., Firat (Euphrates) Universitesi, Firat Tip Merkezi Psikiyatri Anabilim Dali, 23119 Elazig-Turkey Telefon / Phone: +90-424-233-3555/2965 Faks / Faks: +90-424-238-8096 Elektronik posta adresi / E-mail address: [email protected] Kabul tarihi / Date of acceptance: 12 Ekim 2010 / October 12, 2010 Bağıntı beyanı: M.A., S.S., H.Y., A.K., S.K.: Yazarlar bu makale ile ilgili olarak herhangi bir çıkar çatışması bildirmemişlerdir. Declaration of interest: M.A., S.S., H.Y., A.K., S.K.: The authors reported no conflict of interest related to this article. obsessive–compulsive disorder (OCD), which is classified as an anxiety disorder. OCD and hypochondriasis has some similar features such as intrusive thoughts and checking behaviors. On the other hand, hypochonriacal concerns are thought to foster somatization (1,2). It has been proposed hypochondriasis to belong to the obsessivecompulsive spectrum which consists of possible phenomenpological and neurobiological disorders like Tourette’s disorder, otistic disorder, somatoform disorders such as body dysmorphic disorder and hypochondriasis, and impulse control disorders (3-5). Structural imaging studies of OCD, for example, although not always consistent, have suggested basal Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org 293 A volumetric MRI analysis of hypochondriac patients ganglia and frontal pathology (6,7). The findings from structural imaging studies have been inconsistent, with reports of increases (8), decreases (9,10) or no differences (11-13) in the volumes of these key brain regions. Recently, Pujol et al. (14) found reduced gray matter volume in the medial frontal gyrus, the medial OFC, and the left insulo-opercular region. In a very recent metaanalysis, Whiteside et al. (15) reported results that partially support the conclusions drawn from previous narrative reviews that point to structures in the OFC, caudate nucleus, anterior cingulate, and thalamus as the key brain regions in the pathophysiology of OCD. Functional imaging studies have found altered activity in basal ganglia and prefrontal areas at rest and during behavioral challenge with feared stimuli in OCD patients (16). In a recent study, we found that OCD patients had increased white matter volume, significantly smaller left and right OFC volumes and significantly greater left and right thalamus volumes compared to healthy controls. Likewise, in the same study, the patient group had anterior cingulate exhibited a near-significant difference compared to healthy controls on the left side. Previously, Kang et al. (17) measured the volumes of the orbitofrontal cortex, anterior cingulate gyrus, thalamus, and caudate nucleus, which are the main components of the frontal subcortical circuitry in patients with OCD and in normal subjects. These may be key brain regions in the pathophysiology of OCD. Functional MRI (fMRI) has been used to investigate hypochondriasis. Van den Heuvel et al. (18) performed voxel-wise analyses of cerebral blood flow changes for contrasts of interest (incongruent vs. congruent color words, OCD-related vs. neutral words, and panic-related vs. neutral words) within and between OCD, panic disorder, hypochondriasis, and control groups. Their findings support the hypothesis of increased distractibility by irrelevant information in patients with OCD, PD, and hypochondriasis associated with frontal-striatal and limbic involvement compared with controls. So far, no hypochondriasis study has examined the OFC, anterior cingulate, caudate nucleus, and thalamus concurrently in hypochondriac patients. Accordingly, we decided to perform a volumetric MRI study in hypochondriac patients, visiting our clinic for the first time, focusing on in vivo neuroanatomy of the whole brain, total gray and white matter volume, thalamus, caudate nucleus, anterior cingulate cortex, and the OFC concurrently. 294 MATERIALS AND METHODS Subjects and clinical evaluations The study group was retrospectively composed of patients with hypochondriasis who applied to Firat University School of Medicine Department of Psychiatry directly or by referral to our department. A majority of these patients had brain MRI investigation done for severe headaches (n=8), and the remainder needed the same investigation for a variety of other differential diagnoses (e.g., meningitis, encephalitis, brain mass, etcA total of sixteen patients and the same number of healthy controls were studied. Diagnoses were made according to the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV) and the Structured Clinical Interview for the Diagnostic Schedule for Mental Disorders-Fourth Edition (SCID) (19). Severity of depressive symptoms was assessed with the Hamilton Depression Rating Scale (HDRS) (20). Healthy controls were matched on age, sex, education and handedness. Patients with any current comorbid psychiatric disorder, current or lifetime neurological disorders, current medical problems, history of head trauma, and alcohol/substance abuse within the 6 months preceding the study were excluded. With respect to comorbidity in the patient group, as assessed by the SCID and clinical interviews, none met criteria for any current psychiatric disorder. Additional comorbid lifetime Axis I psychiatric diagnoses were major depressive disorder (n=1), and panic disorder (n=1). Healthy control subjects had no DSM-IV Axis I disorders in themselves or in a firstdegree relatives, as determined by the SCID non-patient version, no current medical problems, neurological or psychiatric histories, and no use of psychoactive medications within 2 weeks of the study. None of the controls had taken any psychotropic agents. In the patient group, the father of one patient had a current diagnosis of panic disorder and the mothers of two patients had histories of OCD and depressive disorder. There were no significant group differences in age, years of education, and sex and handedness ratios. The procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 1983. Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org M. Atmaca, S. Sec, H. Yildirim, A. Kayali, S. Korkmaz MRI Procedure MRI were acquired with a 1.5-Tesla GE signa Excite high speed scanner (Milwakuee, USA). A high-resolution structural image of the entire brain was obtained using sagittally acquired 3D spiral fast spin echo high-resolution images (repetition time [TR]=2000 ms, echo time [TE]=15.6 ms, field of view [FOV]=240 mm, flip angle=200, bandwidth=20.8, slice thickness=2.4 mm, echo spacing=15.6 ms, 8 echoes, matrix size=240, resolution=0.9375×0.9375×2.4 mm). Anatomic measurements were obtained on a computer advanced workstation with the GE Volume Viewer voxtool 4.2 program. Tracing was performed by one researcher (HY) blind to the diagnoses of the subjects, and independently verified by a second (HO) blinded investigator. Measured brain structures consisted of the whole brain, total gray and white matter volumes, thalamus, caudate nucleus, anterior cingulate cortex, and the OFC. The boundaries of structures evaluated were delineated on the coronal MR images according to standard brain atlases (21-23) and were adapted from Noga et al. (24), Portas et al. (25), Lacerda et al. (26), Sassi et al. (27), and Riffkin et al. (13): Caudate. For the tracing of caudate nucleus, posterior border was determined as pontine cistern. The posterior landmark was represented by the pontine cistern. The lateral ventricle and the internal capsule were the medial and lateral boundaries, respectively. The most anterior boundary was identified using the mammillary bodies of the hypothalamus as a landmark. Thalamus. The anterior boundary was defined as the mammillary bodies and interventricular foramen. The posterior boundary was the point merging the thalamus Figure 1: Anatomic landmarks for the tracing of the structures evaluated Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org 295 A volumetric MRI analysis of hypochondriac patients under the crus fornix. The lateral boundary was the internal capsule while the third ventricle was determined as the medial boundary. The inferior and superior boundaries were the hypothalamus and the lateral ventricle, respectively. OFC. The last slice traced was the most anterior coronal slice where brain tissue could be identified. For the tracing procedure for measuring the OFC, the posterior boundary was established where the olfactory sulcus was just visible. The posterior boundary was established where the olfactory sulcus was just visible. While the inferior boundary was accepted by the most inferior aspect of the cortex, the lateral boundary was defined by the most lateral edge of the cortex. The medial boundary was the longitudinal fissure. Anterior cingulate. For the tracing procedure for measuring the anterior cingulate, the cingulate sulcus defined the upper limit and the callosal sulcus the lower limit of the cingulate gyrus. The tracing was continued until the slice where the anterior commissure was most visible. The posterior boundary was the anterior commissure. Examples of the structures of coronal slices are presented in Fig 1. All volumes were reported in cubic centimeters. For ICV, whole brain, total gray and white matter volumes, the interrater reliability (intraclass correlation coefficient [ICC]), established by tracings of two different evaluators, was found to be high, ranging between 0.88 and 0.94. ICC’s were 0.86 and 0.86 for left and right OFC, 0.82 and 0.85 for left and right ACC, 0.88 and 0.96 for left and right thalamus and 0.86 and 0.86 for left and right caudate nucleus, respectively. Statistical Analysis Analysis of covariance (ANCOVA), t test, and partial correlation analyses were conducted using SPSS for Windows software, version 10.0 (SPSS, Chicago, IL). In ANCOVA analyses, age and whole brain volumes were covariates. Correlation analyses were done by using Spearman’s rank test. Statistical significance was defined as P<0.05 by a two-tailed t-test. RESULTS No significant difference was found in demographic variables of age, gender composition, educational level, and intracranial volume (ICV) between hypochondriac patient (1432.3±134.8) and healthy control groups (1456.9±152.1) (t=0.959; P>0.05). In the patient group, HDRS scores were 14.5±4.1 (Table 1). Whole brain volume, white and gray matter volumes did not differ between patients and healthy controls (P>0.05). Hypochondriac patients had significantly smaller mean left (t=6.21; P<0.001) and right (t=3.45; P<0.01) OFC, and greater left (t=4.72; P<0.001) but not right (t=1.35; P>0.05) thalamus volumes compared with healthy controls. There was no difference in regard to caudate and anterior cingulate volumes for both sides between groups (P>0.05). Whole brain volume, white and gray matter volumes did not differ between patients and healthy controls after covarying for age (P>0.05). The OFC volumes remained significantly smaller in the patients after covarying for whole brain volume and age. Specifically, the repeated measures ANCOVA predicting left and right OFC volumes detected a significant main effect of diagnostic group (P=0.034). After covarying for whole brain volume, a statistically significant difference still remained between patients and healthy controls (P=0.039) in regard to left thalamus. The HDRS scores were not associated with any volumetric parameter studied. Age at onset showed a Table 1: Clinical and demographic characteristics Item Patients group (n=16) Control group (n=16) Age (years) 30.4±4.2 26.8±3.1 Gender (Female/Male) 7/9 8/8 Education High school High school 7 7 Elemantary school 3 2 First school 2 3 Handedness (right) 16 16 Length of illness (months) 5.9±3.3 - Hamilton Depression Rating Score 13.8±4.7 - 296 p >0.05 >0.05 >0.05 >0.05 Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org M. Atmaca, S. Sec, H. Yildirim, A. Kayali, S. Korkmaz Table 2: The Volumes of the Structures Evaluated in Patients versus Controls (Mean ± Standard Error) Patients (n=16) Healthy Controls (n=16) t Whole Brain Volume 1331.45±172.62 1294.67±142.9 1.30 Gray Matter Volume 804.53±91.4 779.64±78.3 1.42 White Matter Volume 526.89±68.57 515.03±55.23 1.19 OFC Volumes Left 10.22±2.31 15.76±2.72 6.15 Right 11.12±2.87 14.94±3.34 5.94 Anterior Cingulate Volumes Left 1.79±0.30 1.67±0.28 0.71 Right 1.90±0.22 1.86±0.57 0.26 Caudate Volumes Left 3.52±0.62 3.78±0.44 1.41 Right 3.98±0.68 3.66±0.91 1.10 Thalamus Volumes Left 6.56±0.68 5.33±0.78 4.72 Right 6.12±11.76 5.83±1.23 1.35 p >0.05 >0.05 >0.05 <0.001 <0.01 >0.05 >0.05 >0.05 >0.05 <0.001 >0.05 Volumes presented are in cm3. significant relation with left OFC (r=0.42, P=0.023), and left thalamus volumes (r=-0.36, P=0.038). Duration of illness also exhibited a significant association with left OFC (r=-0.51, P=0.012), and significant relation with left thalamus volumes (r=0.48, P=0.017). DISCUSSION Before embarking on the interpretation of these interesting results, we want to emphasize some important findings. The present study found a significant reduction of left and right OFC and significantly greater left thalamus volumes of hypochondriac patients compared to healthy controls. In addition, while age at onset showed a significant relation with left OFC and left thalamus volumes, duration of illness also exhibited a significant association with left OFC, and significant relation with left thalamus volumes. To our knowledge, this is the first report of volumetric MRI investigation in patients with hypochondriasis. This is a critical demonstration, as it has not been previously known whether any brain volume abnormalities exist in hypochondriasis. Of particular note is the fact that these findings were obtained in a sample of patients with a “pure” hypochondriasis, i.e., without any past or current major psychiatric comorbidity with the exception of major depressive disorder (n=1), and panic disorder (n=1). Another important feature of the study was the close matching between each patient and a healthy comparison subject, which minimized possible confounding factors such as gender composition, educational level, and age. One of the main psychiatric conditions associated with abonormalities of theOFC which is evaluated in the present study is OCD. Szeszko et al. (8) reported that patients with OCD had significantly reduced bilateral OFC volumes as compared with healthy subjects by using MRI. In Pujol et al.’s study (14), the brains of patients with OCD showed reduced gray matter volume in the medial frontal gyrus, the medial orbitofrontal cortex, and the left insulo-opercular region. In addition, there is evidence of activity changes in the OFC in OCD. Functional neuroimaging studies, which have compared OCD patients with controls, reported inconsistent results on anterior cingulate and caudate abnormalities in OCD, while relatively more consistent findings have been reported on abnormalities of the the OFC in OCD patients (28). Several authors (3) have proposed that hypochondriasis may belong to the “obsessive–compulsive spectrum” which is a group of disorders that share several features with OCD, including symptoms, sex ratio, course, comorbidity, and neurobiological and neuroanatomical associations although this spectrum can be defined in various ways. Moreover, in the present study, we found that hypochondriac patients had significantly smaller left and right OFC volumes compared to healthy controls. These results are in accordance with, not only the findings of the mentioned studies, but also the conceptualization that hypochondriasis may be an obsessive–compulsive spectrum disorder. Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org 297 A volumetric MRI analysis of hypochondriac patients There is no systematic investigation evaluating thalamic volumes in hypochondriasis. In only one case report, it has been reported that hypochondriac complaints including long-standing hysterical pain and visceral disturbances were successfully treated by unilateral anterior thalamotomy (29). The fact that partial thalamotomy could reduce symptom severity in treatmentrefractory OCD patients (30) provides further evidence on its role of pathophysiology of OCD. In our previous study, we have found that patients with OCD have significantly greater left and right thalamus volumes compared with healthy controls. Overall, we may say that hypochondriac patients behave as OCD patients in regard to brain abnormalities in pathophysiology. In the present study, we did not find any differences in regard to anterior cingulate and caudate volumes. No study has examined the role of these areas in hpochondriasis until now. The reason why we evaluated these areas in hypochondriac patients was to determine whether hypochondriasis has similar brain morphometric abnormalities to OCD since the OFC and thalamus are also key brain regions in OCD (11,13,31,32). We suggest that hypochondriasis and OCD seem to share some morphometric differences although they have some morphometric similarities. While age at onset showed a significant relation to left OFC and left thalamus volumes, duration of illness also exhibited a significant association with left OFC, and left thalamus volumes. This finding suggests that OFC and thalamus abnormalities may be present at the early stages of the illness, supporting the notion of progressive brain structural changes subsequent to the onset of hypochondriasis. The design of our study does not allow us to establish either the time of onset or the mechanisms of the changes in areas evaluated in hypochondriac patients. In fact, these marked changes may well originate from early developmental processes such as abnormal synaptic arborization or myelination (or may have nothing to do with gray matter at all and be restricted to white matter) or, rather, suggest some kind of neuronal damage that would involve the amygdala, but not the hippocampus. There are several important limitations of this study that should not be overlooked or underestimated. First, the number of subjects is small especially given the condition. To be able to generalize these results, replication of the current findings is essential. Second, as we acknowledged, the statistical threshold applied is somewhat liberal, further underscoring the need for replication. Third, we did not perform a segmentation for anterior cingulate and OFC volumes. Fourth, other limitations including the lack of consideration of the effects of IQ should be mentioned. The fifth limitation is the lack of segmentation of gray versus white matter in OFC and the anterior cingulate. In addition, it is unfortunate that we did not use any rating scale for hypochondriac symptoms. In future studies, rating scales should be used for assessment of hypochondriac symptoms. In conclusion, this morphometric MRI study of hypochondriac patients shows that hypochondriac patients had smaller left and right OFC and significantly greater left thalamus volumes compared to healthy controls. Taken together, our findings suggest that abnormalities in the OFC and thalamus seem to play an important role in the pathophysiology of hypochondriasis. References: 1. Barsky AJ. Hypochondriasis and obsessive compulsive disorder. Psychiatr Clin North Am 1992;15:791-801 2. Sayar K, Ak I. The Predictors of Somatization: A Review. Bull Clin Psychopharmacology 2001;11:266-271. 3. Phillips KA, McElroy SL, Hudson JI, Pope HGJr. Body dysmorphic disorder: an obsessive–compulsive spectrum disorder, a form of affective spectrum disorder, or both?. J Clin Psychiatry 1995;56:4151 4. Phillips KA. The obsessive–compulsive spectrums. Psychiatr Clin North Am 2002;25:791-809 5. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry 1991;148:1138-1149 298 6. Atmaca M, Onalan E, Yildirim H, Yuce H, Koc M, Korkmaz S, et al. Serotonin 5-HT1DB gene’s interaction with key brain regions in obsessive-compulsive disorder. Klinik Psikofarmakoloji BulteniBulletin of Clinical Psychopharmacology 2010;20:23-28 (in Turkish). 7. Insel TR. Toward a neuroanatomy of obsessive-compulsive disorder. Arch Gen Psychiatry 1992;49:739-744 8. Scarone S, Colombo C, Livian S, Abbruzzese M, Ronchi P, Locatelli M, Scotti G, Smeraldi E. Increased right caudate nucleus size in obsessive-compulsive disorder: detection with magnetic resonance imaging. Psychiatry Res 1992;45:115-121 9. Robinson D, Wu H, Munne RA, Ashtari M, Alvir JM, Lerner G, Koreen A, Cole K, Bogerts Bet. Reduced caudate nucleus volume in obsessive-compulsive disorder. Arch Gen Psychiatry 1995;52:393-398 Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org M. Atmaca, S. Sec, H. Yildirim, A. Kayali, S. Korkmaz 10. Szeszko P.R, Robinson D, Alvir J.M, Bilder R.M, Lencz T, Ashtari M. Orbital frontal and amygdala volume reductions in obsessivecompulsive disorder. Arch. Gen. Psychiatry 1999; 56:913-919 21. Yuh W.T.C, Tali E.T, Afifi A.K, Sahinoglu K, Gai F, Bergman R.A. MRI of Head & Neck Anatomy, Churchill Livingstone, New York 1994 11. Jenike MA, Breiter HC, Baer L, Kennedy DN, Savage CR, Olivares MJ, Shera DM, Rauch SL, Keuthen N, Rosen BR, Caviness VS, Filipek PA. Cerebral structural abnormalities in obsessivecompulsive disorder. A quantitative morphometric magnetic resonance imaging study. Arch Gen Psychiatry 1996;53:625-632 22. Jackson GD, Duncan JS. MRI Anatomy: A New Angle on the Brain, Churchill Livingstone, New York, 1996 12.Rosenberg D.R, Benazon N.R, Gilbert A, Sullivan A, Moore G.J. Thalamic volume in pediatric obsessive–compulsive disorder patients before and after cognitive behavioral therapy. Biol. Psychiatry 2000;48:294-300 24.Noga JT, Aylward E, Barta PE, Pearlson GD. Cingulate gyrus in schizophrenic patients and normal volunteers. Psychiatry Res 1995;61:201-208 13. Riffkin J, Yucel M, Maruff P, Wood SJ, Soulsby B, Olver J, et al. A manual and automated MRI study of anterior cingulate and orbito-frontal cortices, and caudate nucleus in obsessive-compulsive disorder: comparison with healthy controls and patients with schizophrenia. Psychiatry Res 2005;138:99-113 14. Pujol J, Soriano-Mas C, Alonso P, Cardoner N, Menchen JM, Deus J, Vallejo J. Mapping structural brain alterations in obsessivecompulsive disorder. Arch Gen Psychiatry 2004;61:720-730 15.Whiteside S.P, Port J.D, Abramowitz J.S. A meta–analysis of functional neuroimaging in obsessive–compulsive disorder. Biol. Psychiatry 2004;20132: 69-79 16. Rauch SL, Savage CR. Neuroimaging and neuropsychology of the striatum. Psychiatr Clin North Am 1997;20:741-768 17. Kang DH, Kim JJ, Choi JS, Kim YI, Kim CW, Youn T, Han MH, Chang KH, Kwon JS. Youn T. Volumetric investigation of the frontal-subcortical circuitry in patients with obsessive-compulsive disorder. J Neuropsychiatr Clin Neurosci 2004;16:342-349 18.Van den Heuvel, O.A, Veltman D.J., Groenewegen H.J, Witter M.P, Merkelbach J, Cath D.C., van Balkom A.J, van Oppen P, van Dyck R. Disorder-specific neuroanatomical correlates of attentional bias in obsessive-compulsive disorder, panic disorder, and hypochondriasis. Arch. Gen. Psychiatry 2005;62:922-933 19. Çorapçıoğlu A, Aydemir Ö, Yıldız M., et al. Structured Clinical Interview for DSM-IV, Clinical Version. Hekimler Yayın Birliği, Ankara, 1999 (in Turkish). 20.Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry 1960;23:56-62 23. Patel VH, Friedman L. MRI of the Brain: Normal Anatomy and Normal Variants, WB Saunders Company, Philadelphia, 1997 25. Portas CM, Goldstein JM, Shenton ME, Hokama HH, Wible CG, Fischer I. Volumetric evaluation of the thalamus in schizophrenic male patients using magnetic resonance imaging. Biol Psychiatry 1998;43:649-659 26. Lacerda AL, Nicoletti MA, Brambilla P, Sassi RB, Mallinger AG, Frank E, Frank E, Kupfer DJ, Keshavan MS, Soares JC. Anatomical MRI study of basal ganglia in major depressive disorder. Psychiatry Res 2003;124:129-140 27.Sassi R.B, Brambilla P, Hatch M.A, Mallinger A.G, Frank E, Kupfer D.J, Keshavan M.S, Soares J.C. Reduced left anterior cingulate volumes in untreated bipolar patients. Biol. Psychiatry 2004;56,:467-475 28. Saxena S, Brody A.L, Schwartz J.M, Baxter L.R. Neuroimaging and frontal-subcortical circuitry in obsessive-compulsive disorder. Br. J. Psychiatry Supplement 1998;26-37 29.Andy OJ. Successful treatment of long-standing hysterical pain and visceral disturbances by unilateral anterior thalamotomy. J Neurosurgery 1973;39:252-254 30.Chiocca EA, Martuza RL. Neurosurgical therapy of obsessive compulsive disorder. In: Jenike MA, Baer L, Minichiello WE, editors. Chicago: Year Book Medical Publishing, 1990 31. Stein D.J, Coetzer R., Lee M, Davids B, Bouwer Cet.. Magnetic resonance brain imaging in women with obsessive-compulsive disorder and trichotillomania. Psychiatry Res. 1997;74:177-182 32.Bartha R, Stein MB, Williamson PC, Drost DJ, Neufeld RW, Carr TJ, Canaran G, Densmore M, Anderson G, Siddiqui AR. A short echo 1H spectroscopy and volumetric MRI study of the corpus striatum in patients with obsessive-compulsive disorder and comparison subjects. Am J Psychiatry 1998;155:1584-1591 Klinik Psikofarmakoloji Bülteni, Cilt: 20, Sayı: 4, 2010 / Bulletin of Clinical Psychopharmacology, Vol: 20, N.: 4, 2010 - www.psikofarmakoloji.org 299