Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug interaction wikipedia , lookup
NMDA receptor wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Toxicodynamics wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Psychopharmacology wikipedia , lookup
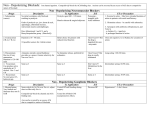
Everyone Relax and Breath: Review of Neuromuscular Relaxants Timothy Finn, CRNA MSN, PhDc Sedation Scale to Lecturing Attentive Interested Good Need Review more Following Coffee When is the next break Will anyone notice if I leave? When will he shut up? Stage 4 of anesthesia ZZZZZZZ! Jaw Thrust! Objectives Review of current and future muscle relaxants Explain the physiology and metabolism Understand the different properties Identify appropriate monitoring techniques Emphasize the pro’s/con’s to reversing Implications for practice History of Muscle Relaxants Earliest known muscle relaxant Curare 16th Century Natives in South America Amazon Basin Poison tipped arrows Ourare Poison tipped arrow History of Muscle Relaxants Curare Active ingredient Tubocurarine chloride Jan 23, 1942 Griffith and Johnson pioneered clinical introduction Tubocurarine chloride Montreal Homeopathic Hospital Present day Luxury and excuse for surgeons I want Relaxation!!!!! 2 Types of Muscle Relaxants NEUROMUSCULAR BLOCKERS (Peripherally) SPASMOLYTICS (Centrally) Spasmolytic Reduce spasticity Enhance the level of inhibition Centrally acting Treatment of neuromuscular conditions Spasmolytic Used to treat spasticity Increased muscle tone Combined with muscle weakness Centrally acting muscle relaxants Inhibit reflexes within the spinal cord or GABA receptors Spasmolytic Dantrolene Mechanism of Action Reduces skeletal muscle strength by interfering with muscle excitation Interferes with calcium release through the sarcoplasmic reticulum Cardiac and smooth muscles are depressed Spasmolytic Dantrolene 1) Used for muscle spasticity 2) Malignant hyperthermia Inability of sarcoplasmic reticulum to sequester calcium Rapid release of calcium with massive muscle contraction, lactic acid production and increased body temp. Neuromuscular Blockade Interfere with motor end plate transmission No CNS activity Relaxes muscles Used for surgical procedures Used for ventilation Primary part of general anesthesia Neuromuscular Junction Neuromuscular Transmission 1. Motor neuron depolarizes causing action potential 2. Depolarization of neuron causes influx of Calcium 3. Calcium influx triggers synaptic vesicles 4. Release of Ach 5. Ach diffuses across synaptic cleft and binds to post synaptic nicotinic receptors. Ach causes influx of sodium and out flux of K leading to depolarization of end plate membrane (muscle contraction) 5. Unbound Ach in synaptic cleft diffuses away and hydrolyzed by AchE (anticholinesterase) Neuromuscular Blockade Presynaptically: Inhibit acetylcholine synthesis or release (practically not used). As they may have whole body unspecific nicotinic as well as muscarinic effects Postsynaptically: Block Receptor activity Block ion channel at the end plate They interfere with the post synaptic action of acetylcholine. Neuromuscular Blockade Drugs that relax skeletal muscle by interacting at the neuromuscular junction 1) Depolarizing Produce excessive depolarization of the motor end plate causing excessive stimulation 2) Nondepolarizing Prevents access of Ach to its receptors Prevents depolarization of the motor end plate Neuromuscular Blockade Chemical breakdown All neuromuscular blockers resemble ACh molecule All are poorly lipid soluble Quaternary nitrogen Depolarizing Neuromuscular Blockade Drug Duration Elimination Succinylcholine 5-10 min -Plasma Cholinesterase -Rapid metabolism Decamethonium (Syncurine) Depolarizing Neuromuscular Blockade Mechanism of action Act like ACh Persist in higher concentration and longer duration of action Opens Na+ channels Leads to muscle contraction/twitching Depolarizing Neuromuscular Blockade Adverse Effects Results Cardiac Arrest Hyperkalemia due to drastic release of K in cases of burns and trauma Muscarinic effects of acetylcholine resulting in bradycardia Increased Intraocular Pressure Contraction of ocular muscles Increased Intragastric Pressure Muscle fasiculations Muscle Pain Muscle contractions resulting in myalgias Malignant Hyperthermia Various symptoms including muscles rigidity Non-Depolarizing Neuromuscular Blockade Mechanism of action Act by blocking ACh receptors Key-in-hole Theory Combine with nicotinic receptors to prevent ACh binding Competitive blockers Prevent depolarization Inhibit muscle contraction Action is overcome by increasing ACh available at receptor site. Non-Depolarizing Neuromuscular Blockade All receptors are not made equally All muscles are not equally sensitive Small rapidly contracting muscles are relaxed first Respiratory muscles Last to be affected First to recover Non-Depolarizing Neuromuscular Blockade Does not cross blood brain barrier (poorly lipid soluble) Limited volume of distribution Highly ionized Low lipophilicity Most metabolized by the liver, kidney, and plasma Organ insufficiency may affect metabolism Degraded spontaneously by ester hydrolysis (Cisatracurium) NonDepolarizing Neuromuscular Relaxants NonDepolarizing Neuromuscular Relaxants Cisatracurium Isoquinoline Dosage 0.05 – 0.1 mg/kg Onset 2.4 - 3.2 min Intermediate duration 25 % recover 15-24 minutes Metabolized by Hoffman elimination and ester hydrolysis Adverse effect Histamine release Bronchospasm Drug Interactions Amikacin Tetracycline Capreomycin Tobramycin Clindamycin Minocycline Doxycycline Kanamycin Neomycin Streptomycin Rocuronium Aminosteroid Dosage 0.6 – 1.2 mg/kg Rapid onset 0.4-6 minutes Avg < 2 minutes Intermediate duration 25% recovery in 12 – 15 minutes Metabolized Hepatic (75-90%) and Renal High allergic risk/Anaphylaxis Particularly asthmatics Drug Interactions Vecuronium Aminosteroid Dosage 0.08 – 0.1 mg/kg Onset 2.5 – 3 minutes 25% recovery 25 – 40 min Metabolized Renal/Hepatic Adverse effects Histamine release Bronchospasm Caution in Hepatobiliary/Renal Issues Drug Interactions Amikacin Tetracycline Capreomycin Tobramycin Clindamycin Minocycline Doxycycline Kanamycin Neomycin Streptomycin Pancuronium Aminosteroid Dosage 0.04 – 0.10 mg/kg Onset Short acting 4.0-6.0 minutes 25% recovery 80–100 minutes Metabolism Enzymatic hydrolysis Renal/Hepatic Adverse effects Tachycardia Hypotension Wheezing Histamine Mivacurium Benzylisoquinolinium Dosage 0.07 – 0.10 mg/kg Onset Short acting 2.0 – 7.6 minutes 25% recovery 8-24 min Metabolism Enzymatic hydrolysis Renal/Hepatic Adverse effects Bronchospasm Wheezing Histamine Drug Interactions Amikacin Lincomycin Aminophylline Phenytoin Azathioprine Piperacillin Carbamazepine Theophylline Clindamycin Tobramycin Fosphenytoin Gentamicin Measuring Muscle Relaxation Train of Four 4/4 0/4 100% receptors blocked 1/4 90% receptors blocked 2/4 80% receptors blocked 3/4 75 % receptors blocked 4/4 0-75% receptors blocked Ulnar Nerve Facial Nerve Posterior Tibial Nerve Train of Four Adductor Pollicis-easily blocked Ulnar nerve monitoring beneficial for two main reasons: 1. Ease of placement and access 2. Ease of monitoring/accessibility Train of Four Redosing Muscles Relaxant 0/4 I 1/4 2/4 I I 90% Blocked Induction Dose 0/4 I 80% blocked 100% 10% of Induction Dose blocked Incidence of Residual Neuromuscular Blockade 25-35%Occurrence Incidence of Residual Neuromuscular Blockade Decreased respiratory muscles Decreased TV and cough reflex Decreased coordination of Laryngeal-Pharyngeal musculature Increased risk of aspiration Increased cost of hospital and intensive care Sensitivity of Muscles Diaphragm Larynx Adductor Muscles Head and Neck Pharynx (Swallowing reflexes) Extraocular Muscles Most Sensitive To Reverse or Not To That is the Question? Neuromuscular Blockade Reversal Mechanism of action Increasing concentration of acetylcholine in synaptic cleft Maximize muscarinic receptors Ex. Neostigmine, Physostigmine, Edrophonium Adverse effect Bradycardia, headache, blurred vision, nausea, vomiting, abdominal cramps Muscarinic anticholinergics Atropine and Glycopyrolate Avoid muscarinic receptor effects Sugammadex Sugammadex Modified gamma-cyclodextrin Reversal of neuromuscular blockade Specific to aminosteroid neuromuscular blocking agents Rocuronium First selective relaxant binding agent Does not rely on inhibition of acetylcholinesterase Immediate reversal < 3 minutes Encapsulates the nondepolarizers Reversal dose = 2 - 4mg/kg Must have 1 – 2/4 twitches Psuedocholinesterase Deficiency Heterozygous atypical (1 abnormal gene) 1 in 50 patients Prolonged blockade 20-30 minutes after succinylcholine Homozygous atypical (2 abnormal gene) 1 in 3000 patient. Prolonged blockade 6-8 hours after succinylcholine Dibucaine number represents the percentage inhibition of pseudocholinesterase activity Inhibits normal pseudocholinesterase by 80%, Heterozygous by 40-60% (atypical) Homozygous by 20% (atypical) Dibucaine Number