Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
NK1 receptor antagonist wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Drug design wikipedia , lookup
Drug discovery wikipedia , lookup
Plateau principle wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Theralizumab wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Norepinephrine wikipedia , lookup
Drug interaction wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
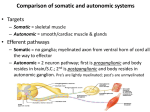
ANS PHARMACOLOGY REVIEW Neurotransmitters & Rcs at various sites of ANS -Memorize various NTs secreted at Pre & post ganglionic level -Figure out the Rcptrs at aforesaid Levels -Why Rcptors at various levels are Different? 15 Somatic N Sympathetic Motor Fiber Smooth Muscle Postganglionic Fiber;N Cardiac Cells Adrenergic E Gland Cells α, β Ganglion Ach Ach Sympathetic EPI/NE Ach Adrenal Gland Parasympathetic Ach Muscle Ganglion Ach Sympathetic N Skeletal Ganglion Ach N Sweat Glands M Smooth Muscle Cardiac Cells Gland Cells Ach Which of the following receptors are responsible for “stress-sweating” in 21-yearold man as he clicks the first question onto the screen for his Step 1 USMLE exam? A. B. C. D. E. Alpha-adrenergic Beta-adrenergic Histaminergic Dopaminergic Muscarinic Answer: A Apocrine sweating Drugs modifying autonomic neurotransmission at various levels ,autonomic Receptors & their 2nd Messenger System -Know the specific moa of -Figure out the Rcptrs at aforesaid Levels -Why Rcptors at various levels are Different? 15 Cholinergic Transmission Acetylcholine (ACh) Synthesized (Step1) by choline acetyltransferase (ChAT) • Acetyl-CoA synthesized in mitochondria • Choline transported into the neuron • Blocked by hemicholinium (blocks uptake of choline) ACh transported (Step2) into small clear vesicles • Transporter can be blocked by vesamicol (depletes neurotransmitter stores) Release (Step3) of transmitter is calcium-dependent • Triggered by action potentials • ACh release blocked by botulinum toxin Acetylcholine binds to receptors (Step4) (cholinoceptor) Catabolized (Step5) by acetylcholinesterase (AChE) • Breaks ACh into choline and acetate • Terminates the action of the transmitter • Half-life of acetylcholine is very short • AChE in other tissues, eg, red blood cells 7 Examples of Drugs Affecting Parasymp. Neurotransmission Mechanism of action Drugs Affecting Acetylcholine Neurotransmission Inhibit synthesis of neurotransmitter Hemicholinium* Prevent vesicular storage of neurotransmitter Vesamicol* Inhibit release of neurotransmitter Botulinum toxin Increase release of neurotransmitter Black widow spider venom (α-latrotoxin)* Inhibit reuptake of neurotransmitter - Inhibit metabolism of neurotransmitter Cholinesterase inhibitors (physostigmine) Activate postsynaptic receptors Acetylcholine, bethanechol, and pilocarpine Block postsynaptic receptors Atropine and tubocurarine (block muscarinic and nicotinic receptors, respectively) *These agents have no current medical use. A pack of girls were expediting their social research in various countryside of Mexico. After few days couple of girls developed various symptomatology mimicking ‘cholinergic stimulation. That place is quite known for black widow spider . What could be the possible mechanism of such toxicity? Cholinergic Receptors: Receptors Activated by Ach Muscarinic Receptors (Activated by muscarine from Amanita muscaria) Nicotinic Receptors (Activated by nicotine from tobacco) M1 (Nerve Cells) M2 NM (Neuromuscular) (Blocked by NN Tubocurarine) Autonomic ganglia, (Heart & SM) M3 (Vas. & other SM) M4 (SM & Glands) (Blocked by Atropine) M5 (?) Adrenal medulla & CNS (Blocked by Trimethaphan or Hexamethonium) Muscarinic Receptors M1 & M3 Gq Activation of PLC Formation of IP3 Release of Intracellular Calcium Formation of DAG Activation of PKC M2 & M4 α subunit Inhibition of Adenylyl Cyclase Gi β subunit Opening of Potassium Channels When acetylcholine is injected into an experimental subject, which of the following cholinergic-mediated mechanisms is responsible for the formation endotheliumderived relaxing factor (EDRF) or nitric oxide (NO) formation, the factor that initiates vasodilatation? A. B. C. D. E. Activation of adenylyl cyclase Activation of guanylyl cyclase Inhibition of adenylyl cyclase Opening of potassium channels Release of intracellular calcium Answer: E Endothelial-nitric oxide synthase (eNOS) is a Ca2+ dependent enzyme NE Sympathetic Nervous System (Thoracolumbar Outflow) ACh Pilomotor Muscles Sweat Glands ACh = thermal sweating NE = nervous sweating Radial Muscle of Iris Ciliary Muscle Sublingual/Submaxillary & Parotid Gland SA & AV Nodes His-Purkinje System Myocardium Bronchi/Bronchial Glands Stomach Kidneys Blood Vessels Intestines Paravertebral Ganglia Bladder//Genitalia Prevertebral Ganglia Receptor distribution On various organs –memorize ; Predicting outcome through various organsyou can figure out by putting yourself in “fight & flight” mode Norepinephrine is typical product in SNS • In adrenal, NE converted to epinephrine • Dopamine stored in some CNS neurons Conversion of tyrosine to dopa is rate-limiting • Tyrosine hydroxylase • Inhibited by tyrosine analog metyrosine Dopa converted to dopamine • Dopa decarboxylase (inhibited by carbidopa) Dopamine converted to NE • Dopamine-beta-hydroxylase Storage inhibited by reserpine Release blocked by guanethidine and bretylium Uptake 1 (NET) transports catecholamines into presynaptic neuron • Inhibited by cocaine (and TCAs) • Increases transmitter activity NE taken up postjunctionally by uptake 2 Release is calcium-dependent Tyramine and amphetamines • Enter via Uptake 1 NEpool Examples of Drugs Affecting Sympathetic Neurotransmission Mechanism of action Drugs Affecting Sympathetic Neurotransmission Inhibit synthesis of neurotransmitter Metyrosine (alpha-methyl-paratyrosine) Prevent vesicular storage of neurotransmitter Reserpine Inhibit release of neurotransmitter Bretylium Increase release of neurotransmitter Amphetamine Inhibit reuptake of neurotransmitter Cocaine Inhibit metabolism of neurotransmitter Monoamine oxidase inhibitors (phenelzine) Activate postsynaptic receptors Albuterol, dobutamine, and epinephrine Block postsynaptic receptors Phentolamine and propranolol (block α- and β-adrenoceptors, respectively) *These agents have no current medical use. 14 A cocaine addict was brought to ER with a state of hypertensive crisis. What is the possible pharmacologic mechanism through which cocaine has raised BP in this patient? Summary of Catecholamine Biosynthesis Tyrosine Rate limiting step DOPA Dopamine Norepinephrine SYMPATHETIC NERVE ADRENAL GLAND Epinephrine Inhibition of which of the following enzymes would be the most appropriate in the treatment of a 56-year-old man with pheochromocytoma? A. B. C. D. E. Catechol-O-methyltransferase Dopa decarboxylase Dopamine-beta-hydroxylase Phenethanolamine-N-methyltransferase Tyrosine hydroxylase Answer: E Rate limiting step Adrenergic Receptors: Receptors Activated by EPI/NE alpha-adrenergic receptors a (Epinephrine>>Isoproterenol) alpha1-adrenergic receptors (Phenylephrine>>Clonidine) alpha2-adrenergic receptors (Clonidine>>Phenylephrine) beta-adrenergic receptors (Isoproterenol>Epinephrine) beta1-adrenergic receptors (EPI >= NE) beta 2-adrenergic receptors (EPI>>NE) beta 3-adrenergic receptors (NE>EPI) Signal Transduction by a1 - Adrenergic Receptors Phenylephrine Norepinephrine Gq q Polyphosphoinositide q Signal Transduction by a2 - and - Adrenergic Receptors Isoproterenol Clonidine ADRENAL MEDULLA Chromaffin Cells Epinephrine (+) Dilates Airways (+) Cardiac Output (+) Muscle Contraction & Efficiency (+) Fatty Acid Release (+) Mental Alertness (+) ACTH & TSH (+) Glycogenolysis (-) Intestinal Motility Broad effects supporting “fight or flight” Which of the following will occur in a 15-yearold boy after stimulation of adrenal catecholamine release during a stress response? A. B. C. D. E. Bradycardia Bronchodilation Decreased fatty acid release Decreased skeletal blood flow Increased intestinal motility Answer: B Beta-2 activation ANS Rcs their organ distribution & response following agonism & antagonism -predict responses on diff.organs By visulaizing urself preparing For ‘fight & flight’&’rest & digest’ Responses through various sub types of adrenergic & cholinergic Receptors respectively -visualize 2nd MS used by various types of SNS & PNS receptors 15 26 Responses elicited in effector organs by sympathetic and parasympathetic activation Effector organ Adrenergic response Cholinergic response Rate of contraction Increase, β 1 Decrease, M2 Force of contraction Increase, β1 Decrease, M2 (atrial contraction) Atrioventricular conduction Increase, β1 Decrease, M2 in myocardium Vasodilatation, β 2 (α 1 constr*) Vasodilatation, M3 in skeletal muscles Vasodilatation, β2, M3 (contraction α1) Heart Arteries and arterioles Endothelium EDRF release ,vasodilatation M3, M5 (cerebral blood vessels) (See Note below) Skin, splanchnic vessels Contracts, α 1 Veins Contracts, α 1 *Periphery as well 27 Bronchodilatation, β 2 Bronchoconstriction, M3 motility Decrease, α 2 (β 2, ) Increase, M3 sphincters Contraction, α1 Relaxation*, M3 secretion ?Decrease, α Increase, M3 Small secretion, α 1 Secretion, M3, M2 Bronchial muscles Gastrointestinal Exocrine glands Salivary Lacrimal Digestive Secretion, M3, M2 ?Decreased secretion, α Airway Sweat Secretion, M3, M2 Secretion, M3 ‘ M2 Secretion, α1 (Apocrine [ stress]) Secretion, M3 Eccrine sweat glands (thermoregulatory) 28 Pancreatic acini Decreased secretion, α Langerhans islets Decreased secretion, α 2 Increased secretion, β 2 Lipid cells Lipolysis, β 1 β 3 Liver glycogenolysis ↑ glycogenolysis & gluconeogenesis, β 2 ,α 1 Secretion, M Eye Ciliary muscle Contraction, M3 (near vision) Dilatator muscle of pupil (iris Contract., α 1 (Mydriasis) radial muscle) Sphincter muscle of pupil (iris circular) Contraction, M3 (Miosis) Kidney ↑Renin secretion, β 1 ↓Renin secretion α 1 Ureter-motility Increase, α 1 29 Urinary bladder detrusor Relaxation, β2 Contraction, M3 Sphincter/Trigone Contraction, α 1 Relaxation, M3 male Ejaculation, α 1 Erection, M3 uterus (pregnant) Contraction, α 1 Relaxes β2 Genital organs Adrenal medulla Platelets Pre junctional adrenergic Neurons in brian Secretion, N ↑ Aggregation ↓ Release of NE thus sympatholysis Ocular Pharmacology & Glucoma -various therapeutic approaches By exploiting physiological flow Of aquas humor -diff.drugs that are used in t/t. 16 Table 10–3. Drugs Used in Open-Angle Glaucoma. Mechanism Methods of Administration Ciliary muscle contraction, opening of trabecular meshwork; increased outflow Topical drops or gel; plastic film slow-release insert Increased outflow Topical drops Cholinomimetics Pilocarpine, carbachol, physostigmine, echothiophate, demecarium Alpha agonists Unselective Epinephrine, dipivefrin Alpha2-selective Decreased aqueous secretion Apraclonidine Topical, postlaser only Brimonidine Topical Beta-blockers Timolol, betaxolol, carteolol, levobunolol, metipranolol Decreased aqueous secretion from the ciliary epithelium Topical drops Decreased secretion due to lack of HCO3- Topical Diuretics Dorzolamide, brinzolamide Acetazolamide, dichlorphenamide, methazolamide Oral Prostaglandins Latanoprost, unoprostone Increased outflow Topical Structures of the anterior chamber of the eye • Tonometric measurements in a 61-year-old patient revealing a consistent increase in intra ocular pressure together with abnormalities in central visual field testing, are diagnostic of open-angle glaucoma. A number of pharmacologic treatments can slow the progression of the disease, which can ultimately lead to complete blindness if left untreated. Which one of the following statements about such drug therapy is accurate? (A)Beta blockers cause ciliary muscle contraction, increasing aqueous humor outflow. (B)Cholinomimetics causes miosis leads to better outflow of aqueous humor. (C)Topical use of nonselective beta blockers will worsen glaucoma. (D)Activation of alpha receptors leads to miosis. (E)Topical use of AChE inhibitors leads to mydriasis. Directly acting cholinomimetics-Pharmacology -classification based on MOA -ADME based on ter/quarter -diff. in organ system effect in -clinical uses & underlying MOA 17 From: McGraw Hill’s AccessMedicine; Katzung; Table 7-2 Note methyl group blocks nicotinic activity Note carbamoyl group blocks hydrolysis Tertiary natural cholinomimetic alkaloids • Pilocarpine • Nicotine • Lobeline is a plant derivative similar to nicotine in action Muscarine - a quaternary amine • Source – Amantia muscaria Mushrooms 43 Clinical uses of choline esteres and alkaloid Choline Ester Clinical uses Acetylcholine chloride. Short t1/2, no clinical use Methacholine chloride Dx-bronchial hyperreactivity Carbachol chloride Bethanechol chloride Rx-ileus (postop/neurogenic) , urinary retention Choline Alkaloid Clinical uses Muscarine no clinical use, toxological importance Nicotine no clinical use, toxological importance Lobeline no clinical use, toxological importance Pilocarpine Rx-glaucoma (topical), xerostomia • A 54-year-old woman recovering from abdominal surgery receives bethanechol pharmacotherapy. Which of the following symptoms could be expected to be observed in this individual? A. Dry mouth, abdominal cramps and tachycardia B. Miosis, bronchospasm and fasciculations C. Miosis, diarrhea and hypotension D. Constipation, increased sweating and salivation E. Hypotension, fasciculations and decreased urination (A) (B) (C) (D) (E) Calcium efflux Increased cyclic adenosine mono phosphate (cAMP) concentration Increased cyclic guanosine monophosphate (cGMP) concentration Increased inositol triphosphate (lP 3) concentration Potassium efflux • For each of the following pharmacologic effects, select the corresponding mechanism of action. • Contraction of the iris sphincter muscle produced by pilocarpine • Vasodilation produced by sildenafil • Slowing of the heart rate by acetylcholine • A new acetylcholine receipt or inhibit or has just been approved by the FDA. You consider the possible therapeutic implications of this agent and want to review the autonomous nervous supply of various organs. Which of the following nervous outputs is noradrenergic? A. Sympathetic output to adrenals B. Sympathetic output to sweat glands C. Sympathetic output to the bladder D. Parasympathetic output to the heart E. Parasympathetic output to the bronchi • A strong, non-specific muscarinic agonist has recently been developed. This new agent would most likely have which of the following actions? A. Bladder wall relaxation B. Kidney renin release C. Gl sphincter contraction D. Increased ventricular contractility E. Release of endothelium-derived relaxation factor • A new drug seems to have partial agonist/antagonist activity against receptor X. When the drug is applied to cells expressing receptor X, there is an immediate change in transmembrane sodium and potassium flow thought secondary to the opening of receptorcoupled transmembrane ion channels. Receptor X is most likely which type of receptor? A. a1adrenoreceptor B. β1 adrenoreceptor C. β2 adrenoreceptor D. Muscarinic cholinergic receptor E. Nicotinic cholinergic receptor Indirectly acting cholinomimeticsPharmacology -classification based on MOA -ADME based on ter/quarter -diff. in organ system effect in Comparision with DADs. -clinical uses & underlying MOA -toxicity & management 17 Indirect-Acting Cholinomimetics: Basic Pharmacology ACh effects terminated by Acetylcholinesterase Indirect-acting cholinomimetics inhibit this enzyme Cholinesterase inhibitors fall into three chemical groups: (1) Simple alcohols bearing a quaternary ammonium group (doesn’t enter CNS); compete for ACh at the enzyme Edrophonium (2) Carbamic acid esters of alcohols bearing quaternary (doesn’t enter CNS); or tertiary ammonium (enter CNS); groups (carbamates); carbamoylate the active site Neostigmine – quaternary Physostigmine – tertiary (crosses BBB) Carbaryl – high lipid solubility (rapid CNS effects); insecticide (3) Organic derivatives of phosphoric acid (organophosphates); phosporylate the active site Echothiophate; used for glaucoma Soman; nerve agent Sarin; nerve agent Malathion, parathion Bioactivated to give active phosphorylating agent used as insecticides. Cholinesterase Inhibitors: Absorption, Distribution, and Metabolism Absorption of quaternary carbamates is predictably poor • Permanent charge renders them relatively insoluble in lipids The tertiary amine carbamates (physostigmine; carbaryl) are well absorbed • Distribute into the CNS (crossess BBB) • Duration of their effect is determined by stability of inhibitorenzyme complex Organophosphates (except for echothiophate) • Are well absorbed both topically and orally • Are distributed to all parts of the body, including the CNS Cholinesterase Inhibitors: Pharmacodynamics Acetylcholinesterase is primary target Butyrylcholinesterase is also inhibited Quaternary alcohols (edrophonium) reversibly bind to the active site • Inhibition is short-lived (on the order of 2–10 minutes) Carbamate esters undergo a two-step hydrolysis • Covalent bond of the carbamoylated enzyme is slowly hydrolyzed (reactivated) • Inhibition is longer (on the order of 30 minutes to 6 hours) Organophosphates • Results in a phosphorylated AChE active site • Covalent phosphorus-enzyme bond is extremely stable • Inhibition lasts hundreds of hours • Lifetime of enzyme protein • “Aging” strengthens phosphorus-enzyme bond • Before aging, pralidoxime (2-PAM) can restore enzyme function (Reactivation) Cholinesterase Inhibitors: Organ System Effects Most prominent effects are on: • Cardiovascular and gastrointestinal systems • Eye and skeletal muscle Actions amplify the actions of endogenous acetylcholine Effects are similar to direct-acting cholinomimetics Little effect on vascular smooth muscle and on blood pressure • Remember PNS does not innervate peripheral vasculature!) • At NMJ: • Low (therapeutic) concentrations increase force of contraction • Higher doses produce depolarizing neuromuscular blockade Cholinesterase Inhibitors: Clinical Uses Eye • Glaucoma (closed & open angle)-(Physiostigmine,Ecothiophate) • Reduce intraocular pressure • Contraction of the ciliary body • Facilitates outflow of aqueous humor Gastrointestinal and Urinary Tracts (Neostigmine,pyridostigmine) • Clinical disorders related to inactivity of smooth muscle activity • Postoperative ileus • Congenital megacolon • Urinary retention • Neurogenic bladder • Reflux esophagitis • Insufficient salivary secretion Reversal of Non-depolarizing Neuromuscilar blockers (Neostigmine ,pyridostigmine) Cholinesterase Inhibitors: Clinical Uses (cont’d) Neuromuscular Junction (Dx-Edrophonium ); T/t: Neostigmine, pyridostigmine) • Myasthenia gravis • Autoimmune disease affecting NMJ • Cholinesterase inhibitors are valuable therapy • Edrophonium (Tensilon test) – i.diagnostic test for MG (improvement in muscle strength after inj.) ii.differential diagnosis bet. MG & Cholinergic crisis. Atropine intoxication (physostigmine) • Reversal of competitive blockade by cholinomimetics • Physostigmine has tertiary structure so reverses both CNS and peripheral effects Central Nervous System (Tacrine & donepezil ) • Alzheimer’s disease • Tacrine & donepezil have anticholinesterase and cholinomimetic actions • Used in therapy for mild to moderate Alzheimer's disease Cholinesterase Inhibitors: Acute Toxicity “SLUDGE” • Salivation • Lacrimation • Urinary incontinence • Diarrhea • Gastrointestinal cramps • Emesis DUMBBELSS Diarrhea Urination Miosis Bronchoconstriction Bradycardia Excitation; Emesis Lacrimation Salivation Sweating • Can be reversed by atropine (muscarinic antagonist) • Cholinesterase inhibitor poisoning also treated by: • Maintenance of vital signs (respiration) • Decontamination to prevent further absorption • Atropine parenterally in large doses • Therapy may also include treatment with pralidoxime to “rescue” un-aged inhibited enzyme; but pralidoxime contraindicated for carbamate intoxication Irreversibly acting Cholinomimetics These compounds phosphrylate the esteric site of AchE,at serine hydroxyl groups. 1.Phosphorylation-reversible by pralidoxime (2PAM) 2.Removal of part of organophosphate molecule (aging). Complex no longer reversible by 2PAM. R-leaving group P-organophosphate A. B. C. D. E. F. G. • Bethanechol Donepezil Echothiophate Malathion Physostigmine Pilocarpine Pyridostigmine For each patient described below, select the most appropriate drug for treatment. • A 22-year-old woman presents with eyelid and facial ptosis, loss of hand-grip strength, and diplopia, which she says gradually developed over several months. These clinical manifestations are rapidly reversed when intravenous edrophonium is given for diagnostic purposes. • A 60-year-old woman exhibits progressive dementia and complains of the loss of short-term memory over the past year. Her clinical manifestations cannot be attributed to a specific cause. • A 45-year-old man has Sjogren's syndrome and suffers from chronic dry mouth. • A 44-year-old woman returns to her physician for a follow-up examination complaining of fatigue. On her last visit 1-month ago she was diagnosed with myasthenia gravis and placed on neostigmine pharmacotherapy. On questioning she states that 1 week ago she felt weak and increased her dosage of neostigmine. Today, on challenge with edrophonium, a decrease in muscle strength (3/4) is observed. Which of the following is the recommended next step in the treatment of this patient? A. Maintain the current dosage of neostigmine B. Reduce the current dosage of neostigmine C. Increase the current dosage of neostigmine D. Replace neostigmine treatment with physostigmine E. Replace neostigmine treatment with isoflurophate (DFP) • The administration of pralidoxime would be most useful in treating a 29-year-old man 2 hours after an excessive exposure to which to the following cholinergic drugs/poisions ? (A)Soman (B)Donepezil (C)Pilocarpine (D)Physostigmine (E)Echothiophate • A 24-year-old migrant farm worker is rushed to a nearby emergency room after an accidental exposure to an organophosphate insecticide. He is in respiratory distress and is bradycardic. Which of the following drugs can be given to increase the activity of his acetylcholinesterase? A. Atropine B. Deferoxamine C. Dimercaprol D. N-acetylcysteine E. Physostigmine F. Pralidoxime Cholinoreceptor blocking drugs-Uses & a/e -clinical uses & underlying MOA -a/e & contraindications 18 Cholinoceptor-Blocking Drugs: Therapeutic Applications Parkinson's Disease (benztropine, trihexphenidyl) Motion Sickness (scopolamine) Patch behind the ear Preoperative medication – prevents laryngospasm (glycopyrrolate); some are also amnestic (scopalamine) Relieves bronchodilation – asthma and COPD (ipratropium, tiotropium) Relief of vagal syncope Traveler's diarrhea, mild GI hypermotility • Combined with an opioid antidiarrheal (abuse deterrent) Cholinoceptor-Blocking Drugs: Therapeutic Applications Urinary urgency, frequency, incontinence (Oxybutynin; Tolterodine – M3 selective) Oxybutynin available as a patch Reversal of cholinergic poisoning • Requires a tertiary (not quaternary) drug • Large doses of atropine may be needed • Drug may have to be repeated Ophthalmology (homatropine, cyclopentolate, tropcainamide, scoplolamine, atropine) • Retinal examination • Prevention of synechiae after surgery Hyperhidrosis • Relief is incomplete at best • Understand ecccrine (cholinergic) vs. apocrine (adrenergic) glands Cholinoceptor-Blocking Drugs: Adverse Effects Atropine poisoning • Dry mouth, mydriasis, tachycardia, flushed skin, delirium • “Dry as a bone, blind as a bat, red as a beet, mad as a hatter." • Can be treated with physostigmine or symptom management Contraindications are relative: • Glaucoma (especially narrow angle-closure glaucoma) • Prostatic hyperplasia • May increase gastric ulcer symptoms • A 38-year-old traveler presents to your office for a routine check-up. He will be leaving for a cruise next week, and asks for a drug that would prevent the severe nausea and vomiting he experiences on ships. What is the site of action of the most appropriate drug for this patient? • You have successfully prescribed neostigmine to a young patient with myasthenia gravis, and her muscle strength has improved markedly. However, she also exhibits cardiovascular and gastrointestinal signs of excessive vagal tone, which you would like to block with atropine. Which of the following risk factors in prescribing atropine is MOST important to you? A. Dry mouth B. Ocular disturbances C. Paralysis of the respiratory muscles D. Tachycardia E. Urinary incontinence. • Atropine and other muscarinic receptor antagonists are used to treat all of the following conditions EXCEPT • • • • • atrioventricular block bradycardia emphysema gastroesophageal reflux urinary incontinence • Ocular effects that include mydriasis and fixed far vision are characteristic of A. mecamylamine B. neostigmine C. phentolamine D. phenylephrine E. timolol • An 11-year-old boy was brought to the ER by some of his friends because he "started going crazy" after eating seeds from a plant while "trying to get high." The boy was incoherent; his skin was hot and dry. His pupils were dilated and unresponsive to light. Blood pressure was 180/105, pulse 150, and rectal temp 400C. The presumptive diagnosis was drug toxicity due to the ingestion of a compound similar to • cannabis • digoxin • mescaline • phencyclidine • scopolamine • Toxic doses of atropine typically cause all of the following effects EXCEPT (A) bronchospasm (B) hallucinations (C) hyperthermia (D) palpitations (E) urinary retention Ganglionic blockers-predicting responses -how to predict response on different Organs following administration of Ganglionic blockers? -reflex control of HR & mechanism 19 Algorithm: Reflex control of Heart Rate • The effects of a ganglion blocking agent may be predicted by knowledge of ANS innervation of effector systems and which branch of the ANS exercises dominance in terms of organ and tissue responsivity. With this principle in mind, one can anticipate that hexamethonium will cause • • • • • abolition of the circulatory reflex cycloplegia reduction of bladder tone xerostomia all of the above Sympathomimetics & their specific adrenergic Rc innervation 20 -required to read the autonomic tracings Adrenoceptor Agonists Sympathomimetics Anxiety, nervousness Fear, fight, flight Pupil dilated Alpha = excitatory Beta-1 = excitatory Beta-2 = inhibitory (relaxation) Direct acting Catecholamines Indirect acting Releasers tachyphylaxis Tyramine Ephedrine Amphetamine Direct adrenoceptor agonists Epinephrine α1, α2, β1, β2 Norepinephrine α1, α2, β1 Isoproterenol β1, β2 Dobutamine β1 (α1) Dopamine D1 (α1 and β1 at high doses) Methoxamine α1 Phenylephrine α1 Methyldopa α2 prodrug Clonidine α2 Ritodrine β2 Terbutaline β2 Albuterol β2 Metaproterenol β2 MAO Inhibitors Tranylcypromine (A) Selegiline (B) Reuptake inhibitors Cocaine Imipramine (TCA) COMT inhibitors Tolcapone Entacapone • A medical student is conducting a pharmacology experiment. He infuses Drug X intravenously over different dose ranges and measures several important hemodynamic parameters. Graphs plotting the recorded measurements of renal blood flow and cardiac output change with increasing doses of Drug X are shown below. Which of the following is most likely to be the drug used in the experiment? A. Epinephrine B. Phenylephrine C. Dopamine D. Edrophonium E. Esmolol Sympathomimetics & uses 21 -clinical uses & underlying MOA Sympathomimetics: Clinical Applications Conditions in which Blood Pressure is to be enhanced: – Hypotension (2o to cardiac arrhythmias, neurologic disease, etc.) – Hypovolemic or cardiogenic shock – Cardiac insufficiency Conditions in which Blood Flow is to be reduced: – – – Hemostasis in surgery (cocaine) Reducing diffusion of local anesthetics (Epi) Reducing mucous membrane congestion (alpha1 agents) Heart failure - may respond to positive inotropic effects of dobutamine • Tolerance/ desensitization limits use in heart failure Sympathomimetics: Clinical Applications Bronchial asthma (bronchodilation by beta2) Anaphylaxis (bronchospasm, hypotension) Fundoscopic examination of the retina (alpha1 – mydriasis) Premature labor – uterus relaxed by beta2 agonists (ritodrine, terbutaline) Narcolepsy - amphetamines produce alertness and defer sleep Attention-deficit hyperactivity disorder (ADHD); methylphenidate Sympatholytics & uses 21 -clinical uses & underlying MOA Alpha-Receptor Antagonists: Clinical Uses Pheochromocytoma • Tumor of the adrenal medulla • Releases a mixture of epinephrine and norepinephrine • Symptoms and signs of catecholamine excess • Hypertension, headaches, palpitations, sweating • Very severe cases treated with metyrosine • Competitive inhibitor of tyrosine hydroxylase Hypertensive Emergencies • Direct vasodilators (nitrates) are preferred Chronic Hypertension • Effective, but may not prevent eventual heart failure • Adverse effect - postural hypotension Urinary Obstruction due to benign prostatic hyperplasia (BPH) • Poorly defined mechanism Some B-Blockers & isolated characteristics 22 Some Beta Blockers Beta blocker -Uses & a/e -clinical uses & underlying MOA -a/e & contraindications 23 Beta-blockers: Clinical Uses Hypertension (Any BB) • Effective and well tolerated • Often used in combination with diuretic or vasodilator drugs Ischemic Heart Disease (Any BB) • Reduce the frequency of anginal episodes • Improve exercise tolerance • Decrease cardiac work • Reduce myocardial oxygen demand • Good evidence that long-term use prolongs survival after MI Cardiac Arrhythmias (only Class II Antiarrhythmics) • Effective in supraventricular and sympathomimetic-driven arrhythmias • Post-MI survival may be due to suppression of arrhythmias • Increase AV node refractory period • Slows ventricular response rates in atrial fibrillation • Reduce ventricular ectopic beats Beta-blockers: Clinical Uses Glaucoma (Timolol,Betoxolol) • Topical administration reduces intraocular pressure • Reduced production of aqueous humor by the ciliary epithelium • Better tolerated than epinephrine-related drugs or pilocarpine in open-angle glaucoma Hyperthyroidism (only Propranolol) • Beneficial effects in limiting excessive catecholamine activity Migraine,performance anxiety & essential tremor (only Propranolol) Combined use *CHF (Labetolol & Carvedilol ;Reversible alpha1 blocker + nonselective beta blocker) *Arrhythmia (Sotalol, Class III antiarrhythmics;K+channel blocker+beta blocker) Toxicity of the Beta-Receptor Antagonist Drugs Drugs are relatively well-tolerated Minor toxic effects include: • Rash, Fever ,Sedation & Depression Major adverse effects: • Related to predictable consequences of beta blockade: • Worsening of preexisting asthma and other airway obstruction (B2) • Vasospasm in patients with peripheral vascular disease (PID) (B2) • Depression of myocardial contractility and excitability • May result in cardiac decompensation(B1) Toxicity of the Beta-Receptor Antagonist Drugs Supersensitivity with abrupt discontinuation after chronic use – Gradual tapering of dosage can prevent hypertensive crisis (B1) – Can exacerbate hypoglycemic episodes in diabetics (B2) & masks the symptoms of hypoglycemia (B1& B2) – BB overdose should be treated with Glucagon rather than beta agonist to prevent development of receptor supersensitivity • A 43-year-old, insulin-dependent diabetic patient is diagnosed with hypertension and begins therapy with an antihypertensive agent. Three days later, he measures his blood glucose at home and finds that it is 53 mg/dL. He recalibrates his glucose testing apparatus and repeats the test, only to find that the first reading was accurate. He is concerned that his hypoglycemia did not produce the normal premonitory signs and symptoms. Which of the following medications was most likely prescribed to treat his hypertension? A. Acebutalol B. Methoxamine C. Methyldopa D. Prazosin E. Propranolol ANS Trachings 24 Effect of an unknown drug on Heart rate and blood pressure Control drug effect Increased diastolic Decreased diastolic Increased Heart rate Decreased Heart rate Increased pulse pressure Increased TPR (Increased α1) decreased TPR (increased β2, decreased α1, directly acting vasodilators and cholinomimetics. increased β1 (May be reflex *) Increased Cholinergic (May be a reflex) increased β1 (increased inotropic activity) Effect of α1 activators on Heart rate and blood pressure •Systemically , increase mean blood pressure via vasoconstriction. •Increased BP may elicit a reflex bradycardia. •Cardiac output may be decreased but also offset by increased venous return. •No change in pulse pressure. Effect of β activators on Heart rate and blood pressure •Systemically, decrease mean BP via vasodilation (β2) and increased HR (β1) •Increased Pulse pressure. Effect of Norepinephrine on Heart rate and blood pressure Exercise: Effect of norepinephrine after pre-tretment with atropine. Effect of Epinephrine on Heart rate and blood pressure • Dose dependent effects – Low dose: β1 ,β2 stimulation. – High dose: α1, β1 (β2). • Β2 specific effects: – Smooth muscle relaxation. – Metabolic effects: • Increased glycogenolysis • Increased gluconeogenesis • Increased mobilization and use of fat. • Exercise: Effect of epinephrine after pre-treatment with α1 blocker. Predicting Responses β1 & β2 Epi reversal β 1, β 2, & α 1 β 1, & α1 Use of α 1blocker to reverse hypertension to hypotension (unmasking β2 action) in pt. receiving too much Epinephrine (Vasomotor reversal of Dale) Effect of an unknown drug (R) on Heart rate and blood pressure 3 logical questions to yourself • R is 1.What does the drug do in control tracing? 2.Does the blocker changes drug response? (compare with control) 3.In +ce of blocker can the drug still do some changes? (compare baseline vs after effect in the same tracing A. epinephrine B. norepinephrine . C. phenylephrine D. isoproterenol E. terbutaline Effect of an unknown drug (U) on Heart rate and blood pressure Effect of an unknown drug (S) on Heart rate and blood pressure Effect of an unknown drug (H) on Heart rate and blood pressure Effect of an unknown drug (R) on Heart rate and blood pressure Effect of an unknown drug (R) on Heart rate and blood pressure • • • • • • Drug H is Isoprotenol Epinephrine. Norepinephrine Phenylephrine Tyramine Effect of an unknown drug (R) on multiple body parameters • • • • • Drug X and Y are, respectively Isoproterenol and propranolol Epinephrine and phenoxybenzamine Norepinephrine and phentolamine Terbutaline and phenylephrine. Acetylcholine and Effect Effectofofananunknown unknowndrug drug(R) (R)ononHeart multiple rate body and blood parameters pressure Effect of unknown drugs on Heart rate and blood pressure in vitro • • • Horner's syndrome is a clinical syndrome caused by damage to the sympathetic nervous system. PAMELa" for Ptosis, Anhidrosis, Miosis, Enophthalmos and Loss of ciliospinal reflex. Lesions First-order neuron disorder: Central lesions that involve the hypothalamospinal pathway (e.g. transection of the cervical spinal cord). Second-order neuron disorder: Preganglionic lesions (e.g. compression of the sympathetic chain by a lung tumor). Third-order neuron disorder: Postganglionic lesions at the level of the internal carotid artery (e.g. a tumor in the cavernous sinus). lesion of the post-ganglionic sympathetic innervation of the right eye. 1. Alpha 1 agonist 2. Releaser / indirectly acting drug 3. Muscarinic receptor blocker 4. Alpha receptor blocker Heart Rate Blood Pressure Look at BP 1st Low dose ACH (2 mg) ACH (50 mg) Intermediate dose (Atropine: Muscarinic Receptor Antagonist) ACH (50 mg) ACH (5 mg) High dose (Hexamethonium: Neuronal Nicotinic Receptor Antagonist) ACH (5 mg) • A medical student is observing a pharmacology experiment where drug A is being intravenously administered to a pregnant dog. Some parameters that are being recorded during the experiment include heart rate, pupil size and uterine contractions .The following diagrams illustrate the measured parameters and observed changes after infusing drug A. Characterize drug A? HR Cardiovascular effects of a new drug (X) that activates autonomic receptors are shown in the table below: Parameter Systolic BP Diastolic BP Heart rate Control 118 mm Hg 85 mm Hg 62/min Drug X 114 mm Hg 54 mm Hg 122/min The most probable receptor affinities of drug X are A. α1, α2 B. α1, α2, β1 C. β1, β2 D. M2 E. NM • A pharmacologist is investigating the cardiovascular actions of Drug X. Alone Drug X causes an increase in blood pressure and a decrease in heart rate when administered iv. If an antagonist at ganglionic nicotinic receptors is administered first, drug X causes an increase in blood pressure and no change in heart rate. Drug X most likely is? A. Epinephrine B. Isoproterenol C.Norepinephrine D.Phenylephrine E. Propranolol • Three days after a 60-year-old man undergoes a bowel resection, he begins hyperventilating and is found to have respiratory alkalosis. The following day, his condition has worsened. Findings include temperature that exceeds 40°C (>104°F), profound hypotension, tachycardia, elevated blood urea nitrogen (BUN) and serum creatinine levels, low urinary output, and a white blood cell count of 18,000/mm3 with a shift to the left. The patient’s sputum is purulent, and a Gram stain shows the presence of gram-negative rods. What agent is the most appropriate drug to give to this patient for hemodynamic support? A.Aspirin B.Dopamine C. Furosemide D.Isoproterenol E.Nitroprusside