Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Serotonin syndrome wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Toxicodynamics wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
5-HT3 antagonist wikipedia , lookup
Polysubstance dependence wikipedia , lookup
Pharmacogenomics wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
Atypical antipsychotic wikipedia , lookup
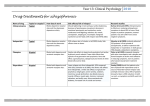
PSYC 342: Psychopharmacology ANTIPSYCHOTIC MEDICATIONS Primary Indication for Use: Schizophrenia Positive symptoms * Delusions Hallucinations Functional Impairments Work/school Interpersonal relationships Self-care Cognitive deficits * Attention Memory Verbal fluency Executive function (eg, abstraction) Disorganization Speech Behavior Negative symptoms * Anhedonia Affective flattening Avolition Social withdrawal Alogia Mood symptoms Depression/Anxiety Aggression/Hostility Suicidality DSM IV-TR Diagnostic Criteria 2 or more of the following for most of 1 month: – – – – – Delusions Hallucinations Disorganized speech Grossly disorganized or catatonic behavior Negative symptoms • Social/occupational dysfunction • Duration of at least 6 months • Not schizoaffective disorder or a mood disorder with psychotic features • Not due to substance abuse or a general medical disorder What, then, is PSYCHOSIS? • Generally equated with positive symptoms and disorganized or bizarre speech/behavior • Impaired “reality testing” • A syndrome present in many illnesses – remove known cause or treat underlying illness – treat symptomatically with antipsychotic medications Other Uses for Antipsychotics • Schizoaffective disorder, bipolar disorder, delusional disorder • Off-label use for Tourette’s, autism spectrum disorders, to augment treatment in depression and OCD, dementia, aggression in children • Medical treatment of nausea, hiccups A bit more terminology….. ….before we blast off. Many names…. Not all the same thing….. Antipsychotics - neuroleptic - typical and atypical - first gen, second gen, third gen - phenothiazine, thioxanthene, butyrophenone - low, med, and hi potency (1st gens) - chemical and trade names - chlorpromazine/thorazine; olanzapine/zyprexa An Historical Timeline • The state of affairs prior to the 1950s - available treatments very ineffective • Early 1950s experimental use of chlorpromazine (thorazine) • Once broadly introduced, institutions emptied out (* but a couple of caveats) • First generation (typical) antipsychotics developed. • Second generation begins with clozapine (1989) A “Typical” (1st Gen) Timeline FDA approval 1953 1958 1958 1959 1959 1967 1967 1970 1975 1977 1984 Generic Name chlorpromazine trifluoperazine perphenazine fluphenazine thioridazine haloperidol thiothixene mesoridazine loxapine molidone pimozide Brand Name (Thorazine) (Stelazine) (Trilafon) (Prolixin) (Mellaril) (Haldol) (Navane) (Serentil) (Loxitane) (Moban) (Orap) Efficacy of Typical Antipsychotics Mechanism of Action: Dopamine D2 receptor antagonist Regions affected by D2 blockade • Mesolimbic (midbrain – limbic) and mesocortical (midbrain – forebrain) pathways – Emotional, cognitive regulation and integration • Nigrostriatal Pathway – Basal ganglia – movement • Hypothalamus-pituitary – Hormones, motivation, regulatory processes • Brain stem – Chemoreceptor trigger zone (compazine) – Descending RAS (reticular activating system) Dopamine related side effects profile • Extrapyramidal side effects (EPS) – Extrapyramidal movement system/basal ganglia – – – – Drug induced Parkinson’s (aka “Thorazine shuffle”) Acute dystonias Akathesia Tardive dyskinesia (sensitization, upregulation?) – Hypothalamic pituitary – Neuroleptic malignant syndrome (high fever, sweating, unstable blood pressure, stupor, muscular rigidity, and autonomic dysfunction). Aggressive medical care needed. – Heat regulation and susceptibility to heat stroke – Increased prolactin – Sexual side effects Other Mechanism of Action Table 4: Clinical Potency and Receptor Affinity for Typical Antipsychotic Agents Receptor type Dopamine D1 Dopamine D2 Norephinephrine Acetylcholine Serotonin Histamine From Baldesarrini, 1985 r with Potency .41 .94 .24 (hypotension, sedation) - .74 (anticholinergic effects) .32 -.44 (sedation) Anticholinergic effects • • • • • Memory deficits, clouded cognition Urinary retention, constipation Dry mouth Blurred vision Tachycardia Limitations of D2 Blockers • • • • “The Law of Thirds” Treatment resistant cases Lack of improvement of negative symptoms EPS side effects Next Gen #1 - Clozapine • Introduction and withdrawal in 1970s Europe – Agranulocytosis • Reintroduction in US – Works in some (30-60%) of treatment resistant patients – Does not produce EPS – Improve affect, reduce suicidality – Agranulocyctosis reversible if detected and drug discontinued (testing protocol – weekly, monthly) What’s Atypical about Clozapine? • • • • NOT a strong D2 blocker (relatively speaking) Antagonizes other dopamine receptors Antagonizes 5-HT receptors Antagonizes histimine, muscarinic Ach, adrenergic NE The Atypical Boom FDA approval 1990 1994 1996 1997 2001 2002 2009 2009 Generic Name clozapine risperidone olanzapine quetiapine ziprasidone aripiprazole iloperidone asenapine Brand Name (Clozaril) (Risperdal) (Zyprexa) (Seroquel) (Geodon) (Abilify) (Fanapt) (Saphris) A small sample of Next Gens • Search to produce clozapine-like drug without agranulocytosis • Prototype: Risperidone (Risperdal) – Dual action – block D2 and 5-HT2 receptors – Other 5-HT/D2 combos • • • • Olanzapine (Zyprexa) Sertindole (Serlect) Quetiapine (Seroquel) Ziprasidone (Geodon) Strengths and Weaknesses of 2nd Gens • Able to dissociate clinical effects from EPS side effects – But for some, this is dose dependent • Able to dissociate clinical effects from agranylocytosis – No need for WBC monitoring • Have become wildly popular. Off label use, especially in young and old, has expanded. – Raises serious concerns Strengths and Weaknesses of 2nd Gens • Expansion to vulnerable populations REAL concern. • Initial promise not entirely fulfilled – Note CATIE and Cutlass studies reported in text • Claims for superior efficacy over 1st gens (for increased tolerability, superior performance with negative symptoms and in treatment refractory) not entirely supported. • Tolerability - similarly lousy compliance rates • Trade-off in side effects profiles 2nd Gen Side Effects • Metabolic syndrome – Weight gain – Blood sugar dysregulation • Increase risk of developing type 2 diabetes • Rapid and independent of weight gain • Increased risk of cardiac problems – Stroke risk in dementia patients – Electrical activity of the heart (sudden cardiac death) 3rd Gens • Aripiprazole (Abilify) – 5-HT2 antagonist – Partial agonist at D2 and 5-HT1a • D2 effects at low and high intrinsic dopamine levels • Antidepressant effects, especially when combined with true antidepressants • Amisulpride (Solian) – D2 and D3 blocker, but selectively in limbic regions (not basal ganglia) – Blocks dopamine autoreceptors (increase DA release) Next: Theories of Schizophrenia • Neurochemical Models – Dopamine Hypothesis – Glutamate Hypothesis • Etiology – Structural anomalies – Heredity – Development • Experimental Research Models