Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Compounding wikipedia , lookup
Discovery and development of beta-blockers wikipedia , lookup
Toxicodynamics wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
Nicotinic agonist wikipedia , lookup
Epinephrine autoinjector wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Drug design wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Prescription costs wikipedia , lookup
Drug interaction wikipedia , lookup
Dydrogesterone wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Psychopharmacology wikipedia , lookup
Neuropharmacology wikipedia , lookup
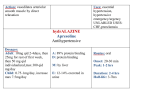
RT 210 Pharmacology Terminology Drug Exerts biological effect used for Treatment Diagnosis Prevention Chemical name Chemical structure of the drug Terminology Generic name Name given by US Pharmacopoeia Trade name Brand or patented name Side effect: Other than desired effects Half life: Length of time when 1/2 dosage is still active in the body Terminology Tolerance: A condition in which the dose of a drug must be increased (over time) to obtain the desired effect -or- a decreasing intensity of responsiveness to a drug over time Tachyphylaxis: Rapidly developing tolerance to a drug -or- a rapid decrease in responsiveness to a drug. Additive effects: The effect of two chemicals acting simultaneously on the same receptors & is the simple sum of the effects that they would have if acting alone Terminology Synergism: The presence of one chemical that enhances the effects of the second. Also, when 2 drugs act on a target organ by different mechanisms of action & the effect of the pair is greater than the sum of the separate effects of the drugs. Terminology POTENTIATION: Special case of synergism in which one drug has no effect, but can increase the activity of the other drug. Also, the action of these two drugs result in the total effect being greater than the sum of the independent effects. Terminology Pharmaceutical phase: Method by which a drug is delivered Inhalation (Benefits) Immediate onset of action at desired site Reduced systemic side effects Smaller doses required Ability of patient to self administer Pharmacokinetic phase: Time required for drug absorption, distribution, metabolization, and excretion Terminology Pharmacodynamic phase: Mechanism of action by which a drug causes its therapeutic effect Agonist: A substance that binds to a receptor and triggers a response in the cell Antagonist: A substance that binds to a receptor but fails to activate the receptor and actually blocks it from activation by agonists Prescription requirements Patient name Drug name Dose Frequency Route of administration Check before administering drug Chart for information Patient's name band Medication label Dates of expiration or opening of the drug Dosage Response to previous administration of drug Normal routes of administration (fastest to slowest) IV (intravenous) Inhaled (aerosol to lung) IM (intramuscular) Sub Q (subcutaneous injection) Sublingual or rectal absorption Oral Topical Concentration The concentration is the percent solution of the active ingredient in the drug It is the weight (in grams or mg) of solute dissolved in a volume (in ml) of solvent expressed as a percentage 1% solution means that 1 gram (1000mg) of solute is dissolved in 100 ml of solvent 1000 mg/100 ml = 10 mg/ml It is possible to determine the amount of solute or solvent needed in a solution of a known percentage Before you can determine the amount of solute or solvent that is needed you must first express the concentration as mg/ml Multiply the percentage by 10 i.e. 1% * 10 = 10 mg/ml 0.5% * 10 = 5 mg/ml Determine what you are trying to find Solute (mg) = solvent (ml) * concentration (mg/ml) You have 1 ml of a 1% solution. How much solute do you need? 1% * 10 = 10 mg/ml Y mg = 1 ml * 10 mg/ml Y mg = 10 mg Solvent (ml) = solute (mg) ÷ concentration (mg/ml) You have 5 mg of a 1% solution. How much solvent do you need? 1% * 10 = 10 mg/ml Y ml = 5 mg ÷ 10 mg/ml Y ml = 0.5 ml Ratios Drug solutions may be expressed as a ratio instead of a percentage A 1:100 solution is a 1% solution and a 1:200 solution is a 0.5 % solution This is derived by the following equation for a 1:100 solution 1/100 = 0.01 then multiply by 100 to give a percentage Thus 0.01 * 100 = 1% For a 1:200 solution we do the same thing 1/200 = 0.005 then we multiply that by 100 Thus 0.005 * 100 = 0.5% Ratios We can determine the desired solute or solvent with a simple equation Solution 10 ml of a 1:100 solution. How much solute do we need? Convert the 1:100 ratio into grams per ml Take 1 and multiply it by 1000 to give us 1000 mg Add ml to 100 so now we have 1000 mg/100 ml Ratios 1000mg Y mg 100ml 10ml 1000mg * 10ml Y mg 100ml 100mg Y mg Solvent 10 mg of a 1:200 solution. How much solution do we need? Set up the equation as before 1000mg 10 mg 200ml Y ml 200ml *10mg Y ml 1000mg 2ml Y ml Nervous system Sympathetic nervous system Adrenergic Uses epinephrine as a neurotransmitter Fight or flight Dilates pupils Dilates bronchioles Speeds up heart rate Secretes adrenaline Nervous system Parasympathetic nervous system Cholinergic Uses acetylcholine as a neurotransmitter Feed or breed Constricts pupils Constricts bronchioles Slows down heart rate Nervous system Adrenergic stimulation Three adrenergic receptors Alpha: Vasoconstriction Beta 1: Increased cardiac rate and strength of contraction Beta 2: Bronchodilation Nervous system Adrenergic stimulation (cont) Stimulation of receptors with sympathomimetic drugs causes Activation of adenylate cyclase Increase conversion of atp into cyclic 3'5'amp Results in bronchodilation Nervous system Adrenergic stimulation (cont) Post stimulation Phosphodiesterase converts cyclic 3'5'amp into 5'amp Break down of cyclic 3'5'amp ends bronchodilation Cholinergic stimulation Nicotinic receptors Stimulation affects all of the PNS and also affects the sympathetic nervous system and skeletal muscles Causes paralysis of skeletal muscles Increases production of dopamine (pleasure response) Muscarinic receptors :Stimulation of receptors stimulates only the PNS Specific sympathomimetics Isoproterenol HCl Trade name – Isuprel Generic - Isoproterenol HCl Concentration - 1:200 (0.5%) solution Receptor effects Alpha 0 Beta1 4+ Beta 2 4+ Short duration Dosage: 0.25-0.5 ml QID or q 4 hours Specific sympathomimetics Isoetharine Trade name: Bronkosol Generic – Isoetharine Concentration – 1:100 (1%) solution Effects Alpha 0 Beta1 1+ Beta2 3+ Duration – medium Specific sympathomimetics Isoetharine (cont) Dosage 0.25-0.5ml QID 1cc maximum Specific sympathomimetics Metaproterenol sulfate Trade Generic - Metaproterenol sulfate Concentration – 5% solution Effects Alupent Metaprel Alpha – 0 Beta1 - 2+ Beta2 - 2+ Medium duration (2 – 4 hrs) Dosage 0.2 - 0.3 ml tid, qid Maximum dose is 0.3 ml Specific sympathomimetics Racemic epinephrine Trade name Generic - Racemic epinephrine Concentration - 2.25% Receptor effects Vaponephrine Micronephrine Asthmanephrine Alpha 2+ Beta1 3+ Beta2 2+ Duration of 0.5 - 2 hours Dosage: 0.25 - 0.5 ml q1-2 hours Specific sympathomimetics Epinephrine HCl Trade – Adrenalin Generic Receptor effects Epinephrine HCl Alpha - 3+ Beta1 - 4+ Beta2 - 3+ Concentration - 1:100 (1%) solution Short duration Dosage: 0.2 – 0.5 ml q2-4 hours Specific sympathomimetics Salbutamol, Albuterol Trade name Ventolin Proventil Generic name International – salbutamol US – albuterol Receptor effects Alpha – 0 Beta1 - 1+ Beta2 - 4+ Concentration - 1:200 (0.5%) solution Long duration Dosage MDI 2 puffs TID, QID 0.5 ml TID, QID Specific sympathomimetics Terbutaline sulfate Trade name Generic name - terbutaline sulfate Receptor effect Bricanyl Brethine Alpha – 0 Beta1 - 1+ Beta2 - 3+ Concentration - 200 µg/puff Long duration Dosage: 2 puffs q4-6 hours Specific sympathomimetics Levalbuterol Trade name: Xopenex (R)-Isomer of Albuterol Very specific Beta2 agonist Same Beta2 as Albuterol No Alpha effects and almost no Beta1 effects Dosage 0.63 mg every 6 to 8 hours 1.25 mg TID Long duration Specific sympathomimetics Side effects of adrenergic bronchodilators Palpitations Tachycardia Hypertension Restlessness Fear Anxiety Tremor Weakness Dizziness Pallor Xanthines Inhibits phosphodiesterase thus maintaining levels of cyclic 3'5'amp This results in better bronchodilation Types Theophylline: Available in tablet and elixir form Aminophylline Administered IV or in tablet form After a loading dose, serum levels are monitored Therapeutic serum level of 10-20 mg/dl Xanthines Side effects Dizziness Headache Restlessness Palpitations, tachycardia Nausea, vomiting Anorexia Xanthines Many physicians now disregard this agent as a choice to treat asthma routinely Has found favor in treating acute asthma attacks with hospital admittance Subcutaneous Epinephrine is often favored as the first agent to try in Status Asthmaticus Parasympatholytics/anticholinergic Enhance sympathetic effects Atrovent Ipratropium bromide Contraindications Allergy to soybeans and peanuts Blocks production of cGMP Side effect: occasional dry mouth Often used in conjunction with albuterol to enhance bronchodilation Parasympatholytics/anticholinergic Atropine Atropine sulfate Frequently used in surgery Blocks production of cGMP Contraindications Sensitivity Glaucoma Tachycardia Parasympatholytics/anticholinergic Atropine (cont) Side effects Dilated pupils Thick drying of secretions Dry mouth Palpitations Tachycardia Corticosteroids Used in the management of the inflammatory process associated with asthma, reactive airway disease, and other pulmonary disorders Administered orally or aerosolized Corticosteroids Side effects Inhaled Oral candidiasis Throat irritation Dry mouth Systemic Cushing’s syndrome Immunosuppression Diabetes Corticosteroids Aerosolized steroids Dexamethasone Decadron MDI provides 84 µg per inhalation Dosage 3 to 4 puffs 3 to 4 times a day Not to exceed 12 puffs per day Corticosteroids Aerosolized steroids (cont) Beclomethasone diproprionate Vanceril, beclovent MDI provides 42 µg per inhalation Dosage 2 puffs 3 to 4 times a day Not to exceed 12 puffs per day Corticosteroids Aerosolized steroids (cont) Flunisolide Aerobid MDI provides 250µg per inhalation Dosage 2 puffs 2 times a day Not to exceed 4 puffs per day Corticosteroids Aerosolized steroids (cont) Triamcinolone acetonide Azmacort, MDI provides 100 µg per inhalation Dosage 2 puffs 3 to 4 times a day Not to exceed 12 puffs per day Budesonide - Pulmicort Respules - 0.25 mg/2 ml , 0.5 mg/2 ml Turbuhaler – (DPI) 1-2 inhalations twice daily Corticosteroids Aerosolized steroids (cont) Fluticasone propionate Flovent MDI provides 44, 110, or 220 µg per inhalation Dosage 2 puffs of 44 µg 2 times a day for mild asthma 4 puffs of 220 µg 2 times a day for severe asthma Corticosteroids Oral steroids Prednisone Action Dosage Reduce inflammation Potentiation of sympathomimetics Loading dose of 4 mg per kg of body weight Maintenance dose of 1 mg per kg Therapeutic serum levels: 100 to 150 mcg/100ml May be given for a 2-3 week period or long term To manage the patient’s condition more adequately Long acting bronchodilators Salmeterol xinafoate Serevent DPI provides 50 µg per blister 1 blister BID MDI provides 25 µg per puff 2 puffs BID 12 hour duration 20-60 minute onset Maintenance therapy only – not for emergency Long acting bronchodilators Formoterol Foradil Dpi provides 12 µg per puff 1 puff bid 12 hour duration 15 minute onset Even though rapid onset and peak effect, better maintenance drug than rescue agent Prophylactic Fluticasone propionate/salmeterol Advair DPI – discus 100 µg Flovent/50 µg serevent BID 250 µg Flovent/50 µg serevent BID 500 µg Flovent/50 µg serevent BID Maintenance only – not for emergency Prophylactic Cromolyn sodium Intal Stabilizes mast cell thus preventing histamine release (degranulation) Indicated for management of chronic extrinsic asthma and is also effective as a prophylactic in patients who have intrinsic asthma Prophylactic effects require 2 to 4 weeks to reach maximal levels Not to be used during acute attack MDI provides 800 µg per puff 2 puffs QID SVN with one 20 mg ampule 1 ampule QID Prophylactic Nedocromil sodium Tilade Stabilizes mast cells and has some anti-inflammatory properties Indicated as part of treatment regimen for management of chronic allergic bronchitis and asthma Blocks early and late asthmatic responses to a variety of allergic and nonallergic triggers Prophylactic effects require 2 to 4 weeks to reach maximal levels MDI provides 1.75 mg per puff 2 puffs QID Leukotriene inhibitors Leukotrienes are mediators of inflammation, edema, and bronchoconstriction Leukotriene activity can be inhibited by synthesis inhibition or by receptor blocking Types Zafirlukast Accolate 20 mg tablets BID Montelukast Singulair 10 mg tablets once a day Zileuton Zyflo 600 mg tablets QID Antimicrobial agents Antibiotics Tobramycin - TOBI Gentamicin Treats most gram-negative organisms Pseudomonas aeruginosa: Often seen in CF patients Acinetobacter Klebsiella Enterobacter Treats some gram-positive organisms: Usually preceded by a bronchodilator Staphylococcus aureus Antimicrobial agents Antiviral Ribavirin Treatment of respiratory syncytial virus (RSV) Causes bronchiolitis in infants Indicated only in carefully selected infants and young children with severe lower respiratory tract infection Delivered with a small particle aerosol generator (SPAG) Antimicrobial agents Antiprotozoal Pentamidine isethionate (Nebu Pent) Treat opportunistic pneumonia caused by pneumocystis carinii Seen in immunocompromised patients such as AIDS Must be given via a nebulizer with several one-way valves and a scavenging expiratory filter – in a negative pressure room or via portable filter system 300mg (powder form) w/6ml Sterile Water Treatment lasts about 15-20minutes Antimicrobial agents Surfactant Replacement Therapy Premature or low birth weight infants often develop IRDS Primary cause is lack of surfactant at birth Survanta and Exosurf Neonatal Instilled via an ETT followed by manual ventilation and positional changes Restores WNL Lung Compliance in RDS of the newborn Equipment for administering bronchodilator treatments Small volume nebulizers Metered dose inhalers (MDI) Dry powder inhalers (DPI) Spacers Mucokinetics (to move mucus) Diluents – wetting agents Thins the mucus making it easier to move Distilled water Used in humidifiers Osmolarity – hypotonic Will be absorbed into interstitial space of tissue May cause edema Mucokinetics (to move mucus) Diluents – wetting agents (cont) Isotonic saline 0.9% saline Normal saline Used as diluent for medication Osmolarity - same as lung Mucokinetics (to move mucus) Diluents – wetting agents (cont) Hypotonic saline Less than 0.9% saline ½ normal saline, 0.45% saline Osmolarity - hypotonic will be absorbed into the interstitial space Used in USN due to evaporation of water from small particles thus becoming isotonic by the time it reaches the patient Can increase airway resistance Mucokinetics (to move mucus) Diluents – wetting agents (cont) Hypertonic saline Greater than 0.9% saline Usually 5% saline Used to induce sputum Osmolarity - hypertonic Draws fluid out of interstitial space to enhance production Can cause bronchospasms Mucokinetics (to move mucus) Mucolytics Acetylcysteine Mucomyst Works by breaking down disulfide bonds of mucus Dose: 10% or 20% Indicated for thick mucoid secretions Should be used with bronchodilator May cause bronchospasm and/or nausea Discard 96 hours after being opened Mucokinetics (to move mucus) Mucolytics (cont) Sodium bicarbonate Raises ph of sputum Viscosity breaks down 2-5 ml of 2% solution, 3-4 times a day Mucokinetics (to move mucus) Mucolytics (cont) Deoxyribonuclease Dornavac Proteolytic enzyme breaks down DNA bonds in sputum Reduces viscosity of sputum 50,000 – 100,000 units aerosolized up to 4 times a day Mucokinetics (to move mucus) Mucolytics (cont) Dornase alfa Pulmozyme Genetically engineered peptide proteolytic enzyme Breaks down extracellular dna in purulent secretions Used to manage purulent mucoid secretions in patients with cystic fibrosis 2.5 mg (1 ampule) aerosolized daily Surface active Ethanol Ethyl alcohol (ETOH) Dose: 5-15 ml of 30% - 50% every 30 minutes for two to four treatments Delivered by SVN or IPPB Indicated for pulmonary edema Alters surface tension thus popping bubbles May cause Bronchospasm Irritation Dehydration Alcohol intoxication Contraindicated in patients taking Antabuse Equipment for administering mucokinetics & mucolytic agents Small volume nebulizers Large volume nebulizers USN