Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Sexually dimorphic nucleus wikipedia , lookup
Triclocarban wikipedia , lookup
Endocrine disruptor wikipedia , lookup
Hormonal contraception wikipedia , lookup
Neuroendocrine tumor wikipedia , lookup
Xenoestrogen wikipedia , lookup
Bioidentical hormone replacement therapy wikipedia , lookup
Vasopressin wikipedia , lookup
Hormone replacement therapy (male-to-female) wikipedia , lookup
Mammary gland wikipedia , lookup
Menstrual cycle wikipedia , lookup
Hyperandrogenism wikipedia , lookup
Hyperthyroidism wikipedia , lookup
Adrenal gland wikipedia , lookup
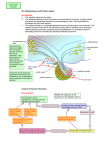
❖ CASE 33 A 44-year-old woman presents to her gynecologist with complaints of not having had a period for the last 8 months. She reports a negative pregnancy test at home. Upon further questioning, she reports a daily headache, changes in vision, and a milky discharge from the breast. She has no medical problems and is not taking any medications. On physical examination, she is noted to have galactorrhea and diminished peripheral vision bilaterally. The remainder of her examination is normal. A pregnancy test is repeated and is negative. A thyroid-stimulating hormone (TSH) level is drawn and is normal. Her serum prolactin level is elevated significantly. After a thorough workup is completed, she is found to have a prolactin-secreting pituitary adenoma. ◆ ◆ ◆ How does hyperprolactinemia cause amenorrhea? Why would a physician need to check thyroid studies in patients with hyperprolactinemia? Where are the posterior pituitary hormones synthesized? 272 CASE FILES: PHYSIOLOGY ANSWERS TO CASE 33: PITUITARY ADENOMA Summary: A 44-year-old woman has secondary amenorrhea, galactorrhea, headache and visual changes, and hyperprolactinemia. She is diagnosed as having a pituitary prolactinoma. ◆ Elevated prolactin and amenorrhea: Elevated prolactin levels inhibit pulsatile gonadotropin-releasing hormone (GnRH) secretion. ◆ Thyroid disease and elevated prolactin: Hypothyroidism is associated with an elevated thyrotropin-releasing hormone (TRH) level that increases the secretion of prolactin. ◆ Synthesis of the posterior pituitary hormones: Hypothalamic nuclei—hormones are synthesized in nerve cell bodies, packaged in secretory granules, and transported down the nerve axon to the posterior pituitary. CLINICAL CORRELATION An elevated prolactin level can be seen in numerous conditions. Patients should be screened initially with a pregnancy test and thyroid studies. Many different medications can cause an elevated prolactin level, including birth control pills, metoclopramide, and many antipsychotic medications. Patients present with amenorrhea secondary to inhibition of GnRH and/or galactorrhea. When adenomas are present, a patient may present with symptoms of headache or even changes in vision. The visual changes (bitemporal hemianopia) and headache usually are related to the prolactinoma compressing the optic chiasm. Normally, prolactin inhibits its own secretion by stimulating the release of dopamine from the hypothalamus. However, when pituitary adenomas are present, prolactin is secreted without inhibition from normal feedback mechanisms. Treatment of microadenomas that are not symptomatic is usually medical with bromocriptine (a dopamine agonist). However, when microadenomas are symptomatic or do not respond to medical management, surgical intervention is often necessary. Macroadenomas usually are treated surgically. APPROACH TO THE PITUITARY GLAND Objectives 1. 2. 3. Discuss the synthesis and secretion of the hormones of the anterior and posterior pituitary. Describe the role of the hypothalamus in the synthesis and secretion of the hormones of the anterior and posterior pituitary. Know the factors that increase and decrease prolactin secretion. CLINICAL CASES 273 Definitions Hypothalamohypophysial portal system: The vasculature that allows for peptides secreted by hypothalamic cells to travel to, and act on, cells in the pituitary. Arcuate nucleus: The region of the hypothalamus whose cells secrete growth hormone-releasing hormone and gonadotropin-releasing hormone, Paraventricular nucleus: The region of the hypothalamus whose cells secrete thyrotropin-releasing hormone and corticotropin-releasing hormone. DISCUSSION The pituitary gland is composed of two lobes that are derived embryonically from the primitive gut (anterior lobe) and the brainstem (posterior lobe). The pituitary secretes a large number of peptide hormones into the blood that affect the growth and secretions of other endocrine glands and/or the function of many end organs directly. Although it plays a major role in regulating many body functions, the pituitary itself is regulated in large part by the hypothalamus and/or by secretory products of other endocrine glands. Concerning the posterior pituitary, nerves extend from the supraoptic and paraventricular nuclei of the hypothalamus to end in the posterior pituitary. Cell bodies in the hypothalamus, not in the posterior pituitary, synthesize and package peptide hormones in secretory granules that then undergo axonal transport to be stored in nerve endings in the posterior pituitary until they are released. The major hormones released from the posterior pituitary are antidiuretic hormone (ADH), also known as vasopressin, and oxytocin. These hormones are released from nerve endings in the pituitary when their nerve cells bodies in the hypothalamus receive stimulatory input. Input for the secretion of ADH comes from hypothalamic osmoreceptors responding to the osmotic pressure of the blood and from receptors located within the cardiovascular system (eg, the right atrium) responding to blood volume (pressure). Input for secretion of oxytocin comes from receptors in the cervix and in mammary glands. Stretching of the cervix during labor and delivery stimulates secretion of oxytocin, which stimulates uterine contractions that result in further stretching of the cervix. This is an example of a positive feedback loop. In nursing females, oxytocin also is released in response to suckling and often as a conditioned reflex in response to the thought of nursing. In this case, oxytocin stimulates milk ejection from the mammary gland. The release of ADH and oxytocin does not appear to be under direct negative feedback from circulating levels of the hormones. The situation for the anterior pituitary differs. Peptide hormones of the anterior pituitary are synthesized and stored in secretory cells in the pituitary itself. Communication with the hypothalamus is via the hypothalamohypophysial 274 CASE FILES: PHYSIOLOGY portal system, one of only two portal systems in the body. Capillaries in the median eminence of the hypothalamus and in the infundibular stem converge to form portal vessels that travel to the anterior lobe, where they branch into a second set of capillaries that supply the anterior pituitary. Thus, mediators released by cells in the hypothalamus can circulate to and affect pituitary secretory cells. The major peptide hormones released from the anterior pituitary are growth hormone (GH); thyroid-stimulating hormone (TSH), also known as thyrotropin; follicle-stimulating hormone (FSH); luteinizing hormone (LH); adrenocorticotropic hormone (ACTH); and prolactin (PRL). The secretion of all these hormones is regulated in large part by mediators secreted into the hypothalamohypophysial portal system by cells in the hypothalamus. In addition, secretion of most of the anterior pituitary hormones is modulated by feedback inhibition from hormones released from the endocrine glands they influence. Secretion of GH is stimulated by growth hormone-releasing hormone (GHRH), and perhaps by ghrelin, which is secreted by cells in the arcuate nucleus. GH secretion is modulated in a complex fashion. In peripheral tissues, GH stimulates the production of insulin-like growth factor-1 (IGF-1). IGF-1 in turn inhibits GH release at the level of the pituitary and the level of the hypothalamus by inhibiting the release of GHRH and stimulating the release of somatostatin, which in turn inhibits the release of GH from pituitary cells. Secretion of TSH is stimulated by the tripeptide TRH secreted by hypothalamic cells in the paraventricular nucleus. At the level of the thyroid gland, TSH stimulates growth of the thyroid and the synthesis and secretion of the thyroid hormones T3 and T4. As part of their actions, circulating T3 and T4 exert feedback inhibition primarily at the level of the pituitary and perhaps also at the hypothalamus. Secretion of FSH and LH is stimulated by the secretion of gonadotropin-releasing hormone (GnRH) from cells in the arcuate nucleus. Unlike the other hypothalamic hormones, to be effective, GnRH must be secreted in a pulsatile manner at a frequency of around 1 pulse per hour. Frequencies much higher or lower than that are not effective at stimulating FSH and LH secretion. Also, GnRH, and hence FSH and LH, secretion is very low during childhood. Starting at puberty and continuing during reproductive life, pulsatile GnRH secretion occurs and FSH and LH are secreted from the pituitary to influence the maturation and function of the reproductive organs. In addition to the control exerted by GnRH, FSH and LH secretion are influenced by both positive and negative feedback. In females, estrogen secreted by the developing graafian follicle suppresses FSH and LH secretion at the level of the pituitary. However, before ovulation, estrogen levels are reached that trigger a surge in secretion of FSH and LH. After ovulation, rising levels of progesterone suppress FSH and LH secretion through actions on both the pituitary and the hypothalamus. In males, testosterone secreted from the testes suppresses LH secretion CLINICAL CASES 275 through actions on both the pituitary and the hypothalamus. FSH secretion is suppressed by inhibin, which also is secreted by the testes and acts at the level of the pituitary. Secretion of ACTH is stimulated by the peptide corticotropin-releasing hormone (CRH), which is secreted by cells in the paraventricular nucleus. At the level of the adrenal gland, ACTH stimulates growth of the adrenal cortex and the synthesis and secretion of cortisol, corticosterone, and small amounts of adrenal androgens and estrogens. ACTH secretion exhibits a diurnal rhythm that peaks early in the morning. The mechanisms controlling this rhythm are not understood completely. As part of their actions, circulating cortisol (mainly) and corticosterone exert feedback inhibition at the level of both the pituitary and the hypothalamus. The regulation of prolactin secretion differs from that of the other pituitary hormones in that PRL secretion is under tonic inhibition from the hypothalamus. If the hypothalamohypophysial portal system is disrupted, PRL secretion increases rather than decreases as is the case for the other pituitary hormones. Most evidence points to dopamine rather than a peptide as being the prolactin inhibitory hormone. In addition to this inhibitory pathway, PRL secretion can be stimulated by TRH. The main target of PRL is the mammary gland, where it promotes the secretion of colostrum and milk. PRL levels rise during pregnancy. After parturition, basal levels fall, but there are spikes in PRL levels during and after periods of nursing. The spikes in PRL secretion are because of neural signals from the breast acting at the level of the hypothalamus to decrease dopamine release into the hypothalamohypophysial portal system. This reflex and the high levels of PRL suppress the hypothalamic secretion of GnRH, thus inhibiting the menstrual cycle. COMPREHENSION QUESTIONS [33.1] A 45-year-old woman is noted to have fatigue and cold intolerance and is diagnosed with hypothyroidism. Her physician suspects a pituitary etiology. Which of the following laboratory findings is most consistent with this condition? A. B. C. D. Low TSH, low free thyroxine Elevated TSH, low thyroxine Elevated TSH, elevated thyroxine Low TRH 276 [33.2] CASE FILES: PHYSIOLOGY A 35-year-old woman experiences anterior pituitary hemorrhagic necrosis (Sheehan syndrome) after a postpartum hemorrhage. She feels light-headed, dizzy, and weak. Which of the following hormones most likely is responsible for her symptoms? A. B. C. D. E. [33.3] ACTH GnRH Prolactin TSH GH A 25-year-old woman is undergoing ovulation induction for infertility. She is given an injection of GnRH on Monday. Serum estradiol is low, and ovarian ultrasound reveals small follicles on Wednesday and Friday. What is the most likely explanation? A. B. C. D. Ovarian failure Pituitary failure Need for pulsatile hormone More time needed to see an effect Answers [33.1] A. Usually, hypothyroidism is diagnosed by an elevated TSH, because the vast majority of cases of hypothyroidism involve a primary gland (thyroid) failure. A much less common etiology is a pituitary etiology, which would be reflected by a low TSH. This would lead to a low free thyroxine but elevated hypothalamic secretion of TRH. [33.2] A. This female with anterior pituitary failure after postpartum hemorrhage has symptoms of dizziness and light-headedness. This probably is because of lack of ACTH and thus lack of mineralocorticoids such as aldosterone. The inability to retain sodium leads to hypovolemia and the symptoms of hypotension. [33.3] C. Unlike the other pituitary hormones, GnRH needs to be secreted in a pulsatile fashion to effect gonadotropin (FSH and LH) secretion from the pituitary. CLINICAL CASES 277 PHYSIOLOGY PEARLS ❖ ❖ ❖ ❖ ❖ ❖ ❖ The posterior pituitary secretes two hormones: antidiuretic hormone (also known as vasopressin) and oxytocin. The anterior pituitary secretes six hormones: GH, TSH, ACTH, FSH, LH, and PRL. Posterior pituitary hormones are released from endings of nerves that originate in the hypothalamus. The secretion of hormones by cells of the anterior hypothalamus is regulated by factors released from the hypothalamus into a portal venous system that runs from the hypothalamus to the anterior pituitary. The secretion of all the anterior pituitary hormones except prolactin requires stimulatory peptide factors to be released from the hypothalamus. Prolactin secretion is tonically inhibited by dopamine secreted by the hypothalamus. Peripheral neural and humoral inputs that regulate posterior pituitary hormone secretion act at the level of the hypothalamus. Peripheral neural and humoral inputs that regulate anterior pituitary hormone secretion act at the level of the hypothalamus and the pituitary. REFERENCES Genuth SM. Hypothalamus and pituitary gland. In: Levy MN, Koeppen BM, and Stanton BA, eds. Berne & Levy, Principles of Physiology. 4th ed. Philadelphia, PA: Mosby; 2006:647-662. Goodman HM. Pituitary gland. In: Johnson LR, ed. Essential Medical Physiology. 3rd ed. San Diego, CA: Elsevier Academic Press; 2003:573-585. This page intentionally left blank