Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
DNA vaccination wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Immune system wikipedia , lookup
Adaptive immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Innate immune system wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Immunosuppressive drug wikipedia , lookup
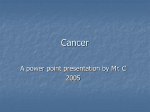
Published OnlineFirst January 20, 2012; DOI: 10.1158/1078-0432.CCR-11-3322 Clinical Cancer Research CCR Translations Commentary on Wilmott et al., p. 1386 Rehabilitation for Oncogene Addiction: Role of Immunity in Cellular Sobriety David L. Bajor and Robert H. Vonderheide Clinical responses to oncogene inhibitors result from direct effects on cell-intrinsic growth signals and disruption of downstream messages that produce a protumor immunosuppressive microenvironment. Combining oncogene-targeted and immunomodulatory therapies may result in synergistic effects, producing increased response rates and longer periods of tumor control than can be achieved with either class alone. Clin Cancer Res; 18(5); 1–3. 2012 AACR. In this issue of Clinical Cancer Research, Wilmott and colleagues (1) report that the administration of selective BRAF inhibitors in patients with metastatic melanoma results in early infiltration of CD4þ and CD8þ T lymphocytes. The magnitude of CD8þ lymphocyte infiltration correlates with tumor shrinkage, but at the time of tumor progression the immune infiltrate is most often lost. These data are important because they support the hypothesis that immune activation plays a role in the antitumor activity of targeting the BRAF oncogene in patients. Metastatic melanoma is a notoriously deadly malignancy, and until recently there were no therapies capable of extending patient survival. In 2011, 2 agents with different mechanisms of action were approved in the United States for use in melanoma, based on evidence that they each prolong overall survival in selected populations. Ipilimumab, a fully human monoclonal antibody, antagonizes cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) on T lymphocytes, thereby silencing a negative regulator of Tcell response. CTLA-4 blockade allows T-cell activation and leads to immune-mediated destruction of melanoma cells. When used as a single agent, the objective response rate for ipilimumab is <15%, but for a minority of patients, clinical response can be sustained long-term (2). The selective BRAF inhibitor vemurafenib was also approved last year, and the drug has emerged as a highly active and well-tolerated treatment that improves survival for patients whose tumors harbor a BRAF mutation. Although cancer cells possess multiple genetic abnormalities, single mutations, such as the constitutively active BRAFV600E in melanoma, can be so crucial to growth and survival that their blockade results in Authors' Affiliation: Abramson Family Cancer Research Institute, Hematology-Oncology Division, Department of Medicine, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania Corresponding Author: Robert H. Vonderheide, 551 BRB ii/iii, 421 Curie Boulevard, Philadelphia, PA 19104. Phone: 215-573-4265; Fax: 215-5732652; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-11-3322 2012 American Association for Cancer Research. tumor cell death, a phenomenon termed "oncogene addiction" (3). Responses to selective BRAF inhibition are often dramatic in terms of reduction of overall tumor burden; unfortunately, however, these transient responses do not typically lead to long-term disease control (4). The fundamental principles of clinical oncology suggest the utility of testing combinations of treatments that exhibit single-agent activity but have different mechanisms of action and nonoverlapping toxicities. By showing that BRAF inhibition is associated with an influx of T lymphocytes, Wilmott and colleagues (1) further fuel the notion that combining targeted therapy and immunotherapy may be able to yield synergistic responses in melanoma (5). The presence of intratumoral T cells is a positive prognostic biomarker in primary melanoma. This may also be the case in metastatic melanoma. Wilmott and colleagues (1) now report that selective BRAF inhibition in patients with metastatic melanoma results in a marked increase in tumor-infiltrating T cells. Although they are not addressed specifically in this study, at least 2 mechanisms could explain this immunological effect. First, tumor cell death in the wake of a therapy that is not itself overtly immunotoxic or immunosuppressive may produce a "vaccine effect" insofar as tumor antigens that are shed after therapy may be processed and presented by host antigen-presenting cells (APC) to drive tumor-specific adaptive immune responses. Second, the influx of T cells during treatment may also occur as a direct response to changes in the tumor microenvironment caused by BRAF inhibition. For example, the production of the immunomodulatory cytokines interleukin 10 (IL-10), VEGF, and IL-6 by melanoma cell lines is controlled by the mitogen-activated protein kinase (MAPK) pathway and decreased in vitro by treatment with mitogen-activated protein–extracellular signal-regulated kinase (MEK) inhibition or BRAFV600E RNA interference (6). Thus, treatment with selective BRAF inhibitors in vivo may alter this immunosuppressive cytokine milieu and permit enhanced infiltration of T cells. In addition, dying tumor cells may also release ATP (7) and other cellular contents that act as strong chemoattractants for T cells that are not otherwise present in www.aacrjournals.org Downloaded from clincancerres.aacrjournals.org on April 29, 2017. © 2012 American Association for Cancer Research. OF1 Published OnlineFirst January 20, 2012; DOI: 10.1158/1078-0432.CCR-11-3322 Bajor and Vonderheide the tumor microenvironment. In this case, T cells may be actively recruited to regressing melanoma, as clearly shown in this study, although it remains to be shown that tumorinfiltrating T cells following BRAF inhibition are tumor specific. The key point, however, is that vemurafenib does not appear to be immunosuppressive, and in fact may promote T-cell responses by enhancing antigen presentation by tumor cells (8, 9). Other immunological effects of BRAF inhibition on the tumor microenvironment may be highly nuanced and intertwined. For example, macrophages are generally considered to be tumor-promoting leukocytes through their roles in angiogenesis, metastasis, and production of a T-cell–suppressive microenvironment. Melanoma cell line growth in the mouse is enhanced by tumor-associated macrophages (10), and the production of macrophage chemoattractant protein 1, the major chemokine for macrophages, is upregulated in part by the MAPK pathway (11), which suggests that its production may be decreased by selective BRAF inhibition. Understanding the role of tumorassociated macrophages in patients receiving selective BRAF inhibitors would be a valuable next step in elucidating the interplay between oncogene inhibition and the innate immune system. The findings from Wilmott and colleagues fit nicely with the increasing body of data regarding the importance of the immune system in eradicating tumors following oncogene inactivation. Using a mouse model of T-cell acute lympho- blastic lymphoma (T-ALL) driven by the c-MYC oncogene, Rakhra and colleagues (12) showed the necessity of the immune system for eliminating tumors completely. In their study, T-ALL tumors driven by the tetracycline-sensitive c-MYC oncogene were implanted into wild-type mice or mice with various forms of lymphocyte deficiency. Tumor growth was monitored following oncogene inactivation, which was accomplished experimentally by doxycycline administration. Partial regression was seen upon c-MYC inactivation in all of the animals; however, in the absence of CD4þ T cells, tumors failed to regress completely and began to grow despite continued oncogene inactivation. The host immune system was shown to produce antitumor cytokines in the presence of c-MYC inactivation, which were necessary mediators of tumor elimination. Similar immune-mediated responses were also seen in a BCR-ABL oncogene–induced model of pro-B-cell acute lymphoblastic leukemia. To the extent that such murine models show that an immune response is important or even required for optimal tumor regression following oncogene inactivation, strategies to add potent immunomodulatory drugs (e.g., antiCTLA-4 mAb) to oncogene-targeted cancer therapies have merit. This is particularly true in melanoma, for which ipilimumab is clinically approved. Indeed, a phase I/II trial combining ipilimumab and vemurafenib recently began accrual. In one proposed mechanism of action (Fig. 1), selective BRAF inhibition blocks the activated MAPK pathway, resulting in tumor cell death by targeting Tumor antigen release T lymphocyte Tumor antigen presentation APC Tumor “Vaccine effect” Tumor death/clinical response Melanoma • BRAF inhibitor resistance • Immune escape • Clinical relapse Immune effector response BRAF inhibition Tumor infiltrating lymphocyte (TIL) No further treatment Associated with increased T lymphocyte infiltrate Addition of immunotherapy • Anti CTLA-4 • Anti CD40 • Anti PD-1 • Others • Combinations • Immunological memory • Sustained clinical response © 2012 American Association for Cancer Research Figure 1. The prospect of immunotherapy cooperating with oncogene inhibition for optimal clinical outcome in metastatic melanoma. BRAF inhibition causes tumor cell death, which is associated with increased lymphocyte infiltration. Tumor antigen released by dying tumor cells is presented to lymphocytes by APCs. Without further treatment, tumors develop BRAF inhibitor resistance, leading to immune escape and relapse. The addition of immunotherapy such as anti CTLA-4, anti CD40, or anti PD-1 (programmed death 1) monoclonal antibodies, or other types of immunotherapy alone or in combination may lead to a more pronounced immune infiltrate, immunological memory, and sustained clinical response. TIL, tumor-infiltrating lymphocyte. OF2 Clin Cancer Res; 18(5) March 1, 2012 Clinical Cancer Research Downloaded from clincancerres.aacrjournals.org on April 29, 2017. © 2012 American Association for Cancer Research. Published OnlineFirst January 20, 2012; DOI: 10.1158/1078-0432.CCR-11-3322 Combining Targeted and Immune Therapy oncogene-addicted cells. The concomitant release of tumorspecific antigens can then be picked up by APCs, which present tumor antigen to T cells and produce cytokines and chemokines that are capable of accelerating the antitumor immune response. BRAF inactivation may also decrease production of immunosuppressive cytokines that regulate the tumor microenvironment, further driving intratumoral infiltration of CD4þ and CD8þ T cells. Ultimately, and unfortunately commonly, treatment resistance emerges, leading to recapitulation of an immunosuppressive microenvironment, immunological escape, and clinical relapse. Treatments such as ipilimumab may be able to fuel a more robust immunological response and potentially clinical responses as well, even perhaps preserving clinical activity in the setting of resistance to BRAF inactivation. Several immunomodulatory agents with different mechanisms of action and more-muted toxicity profiles than ipilimumab are currently showing promise in clinical investigations of melanoma and other malignant diseases (Fig. 1), and many of these can be seen as potential partners with oncogenetargeted therapy. With the increasing development of targeted therapies for multiple types of tumors, the combination of these agents with immune therapy represents an exciting clinical frontier with a sound scientific rationale. Disclosure of Potential Conflicts of Interest Dr. Vonderheide received research funding from Pfizer Corporation. No other potential conflicts of interest were disclosed. Grant Support National Institutes of Health grants (T32 HL007775 to D.L. Bajor and R01 CA158186 to R.H. Vonderheide). Received December 23, 2011; accepted January 11, 2012; published OnlineFirst January 20, 2012. References 1. 2. 3. 4. 5. 6. 7. Wilmott JS, Long GV, Howle JR, Haydu LE, Sharma RN, Thompson JF, et al. Selective BRAF Inhibitors induce marked T cell infiltration into human metastatic melanoma. Clin Cancer Res 2012;18:1386–94. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363:711–23. Weinstein IB, Joe A. Oncogene addiction. Cancer Res 2008;68:3077– 80, discussion 3080. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al.BRIM-3 Study Group. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med 2011;364: 2507–16. Ribas A, Flaherty KT. BRAF targeted therapy changes the treatment paradigm in melanoma. Nat Rev Clin Oncol 2011;8:426–33. Sumimoto H, Imabayashi F, Iwata T, Kawakami Y. The BRAF-MAPK signaling pathway is essential for cancer-immune evasion in human melanoma cells. J Exp Med 2006;203:1651–6. Ghiringhelli F, Apetoh L, Tesniere A, Aymeric L, Ma Y, Ortiz C, et al. Activation of the NLRP3 inflammasome in dendritic cells induces IL1beta-dependent adaptive immunity against tumors. Nat Med 2009;15:1170–8. www.aacrjournals.org 8. Comin-Anduix B, Chodon T, Sazegar H, Matsunaga D, Mock S, Jalil J, et al. The oncogenic BRAF kinase inhibitor PLX4032/RG7204 does not affect the viability or function of human lymphocytes across a wide range of concentrations. Clin Cancer Res 2010;16: 6040–8. 9. Boni A, Cogdill AP, Dang P, Udayakumar D, Njauw CN, Sloss CM, et al. Selective BRAFV600E inhibition enhances T-cell recognition of melanoma without affecting lymphocyte function. Cancer Res 2010;70: 5213–9. 10. Chen P, Huang Y, Bong R, Ding Y, Song N, Wang X, et al. Tumorassociated macrophages promote angiogenesis and melanoma growth via adrenomedullin in a paracrine and autocrine manner. Clin Cancer Res 2011;17:7230–9. s N, Basagoiti M, Dotor J, Aranda F, Monreal I, Riezu-Boj JI, 11. Díaz-Valde et al. Induction of monocyte chemoattractant protein-1 and interleukin-10 by TGFbeta1 in melanoma enhances tumor infiltration and immunosuppression. Cancer Res 2011;71:812–21. 12. Rakhra K, Bachireddy P, Zabuawala T, Zeiser R, Xu L, Kopelman A, et al. CD4(þ) T cells contribute to the remodeling of the microenvironment required for sustained tumor regression upon oncogene inactivation. Cancer Cell 2010;18:485–98. Clin Cancer Res; 18(5) March 1, 2012 Downloaded from clincancerres.aacrjournals.org on April 29, 2017. © 2012 American Association for Cancer Research. OF3 Published OnlineFirst January 20, 2012; DOI: 10.1158/1078-0432.CCR-11-3322 Rehabilitation for Oncogene Addiction: Role of Immunity in Cellular Sobriety David L. Bajor and Robert H. Vonderheide Clin Cancer Res Published OnlineFirst January 20, 2012. Updated version Supplementary Material E-mail alerts Reprints and Subscriptions Permissions Access the most recent version of this article at: doi:10.1158/1078-0432.CCR-11-3322 Access the most recent supplemental material at: http://clincancerres.aacrjournals.org/content/suppl/2012/02/27/1078-0432.CCR-11-3322.DC1 Sign up to receive free email-alerts related to this article or journal. To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at [email protected]. To request permission to re-use all or part of this article, contact the AACR Publications Department at [email protected]. Downloaded from clincancerres.aacrjournals.org on April 29, 2017. © 2012 American Association for Cancer Research.