Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Molecular mimicry wikipedia , lookup
Adaptive immune system wikipedia , lookup
Lymphopoiesis wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
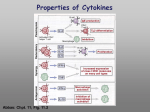
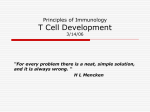
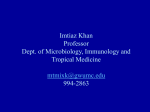
Bulletin 9338 Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function Pat Roth, Ph.D., Ronald Paul, Ph.D. Enrique Rabellino, M.D. INTRODUCTION T CELL BIOLOGY Transplantation of hematopoietic stem cells (HSC) has been applied successfully to restore bone marrow function and provide curative therapy for a number of previously untreatable diseases. The original HSC transplant programs were aimed at reconstituting hemato-lymphopoiesis in patients with immunodeficiency syndromes, aplastic anemia and acute leukemia.1 Encouraged by advances in myeloablative chemotherapy and immunosuppressive regimens, HSC transplant protocols were subsequently developed for many other hematological malignancies, solid tumors (breast, ovarian, neuroblastomas etc.) and more recently, for a host of metabolic, congenital and autoimmune disorders.2-4 Helper CD4 and suppressor CD8 lymphocytes were the first human T cell subsets characterized by immunophenotyping. These findings gained clinical relevance with the recognition of the effect of HIV infection on T cells and the importance of CD4 monitoring in the management of HIV/AIDS patients. CD4 phenotyping provides critical clinical information concerning diagnosis, prognosis, monitoring and evaluating the efficacy of developing therapies. HSC transplantation has the capacity to reconstitute erythroid, myeloid and lymphoid functions.The pluripotent nature of HSC give rise to all blood cell types including immune cells. Patient pre-conditioning for stem cell transplantation includes a myeloablation that eliminates most of the lymphoid cells as well as the lymphopoietic tissues. Thus, the reconstitution of the immune system and in particular the recovery of T cell function, is one of the most important goals of stem cell transplantation. T cells are regarded as the key regulatory and effector cells for multiple cellular and humoral immune functions. The availability of monoclonal antibodies to lymphoid antigens has played a key role in the identification and characterization of functional T cell populations. Therefore the dissection of T cell responses has led to our current understanding of the functional heterogeneity among T cells and their associated phenotypes. Thus, the enumeration of T cells has evolved from T cell counting to subset profiling. The purpose of this communication is to review the current understanding of reconstitution of immunocompetent cells and the methods used to assess their recovery. Eastern Europe, Middle East, North Africa: Switzerland, Nyon (41) 22 994 0707. Australia, Gladesville (61) 2 9844 6000. Canada, Mississauga (1) 905 819 1234. China, Beijing (86) 10 6515 6028. France, Villepinte (33) 1 49 90 90 00. Germany, Krefeld (49) 2151 33 35. Hong Kong (852) 2814 7431, 2814 0481. Italy, Milan (39) 02 953921. Japan, Tokyo (81) 3 5404 8424. Latin America (1) (305) 380 4709. Mexico, Mexico City (525) 575 6805. Netherlands, Mijdrecht (31) 297 230630. Singapore (65) 6339 3633. South Africa/Sub-Saharan Africa, Johannesburg (27) 11 805 2014. Sweden, Bromma (46) 8 564 85 900. Switzerland, Nyon 0800 850 810. Taiwan, Taipei (886) 2 2378 3456. Turkey, Istanbul (90) 216 309 1900. UK, High Wycombe (44) 01494 441181. USA, Miami, FL (1) 800 526 3821, Option 7. www.beckmancoulter.com/cytomics © Copyright 2003 Beckman Coulter, Inc. PRINTED IN U.S.A. The significance of these findings in conjunction with the availability of monoclonal reagents and technological advances in flow cytometry led to an explosion in the research of T lymphocyte differentiation and functional development. This research has led to the current understanding of T cell ontogeny including the recognition of naïve, memory and effector T cells. Due to this new understanding of T cell heterogeneity, the laboratory evaluation of T cells must be more comprehensive than the simple enumeration of CD4 and CD8 subsets. IMMUNE RECONSTITUTION Immune reconstitution following stem cell transplantation encompasses the recovery of the adaptive cells and functions of the immune system. Sustained and complete immune reconstitution is achieved in stages, many of which have been defined by the appearance of distinct cell populations. LYMPHOCYTE SUBSETS In order to evaluate T cell recovery, the first level of posttransplant monitoring consists of immunophenotyping the total T cell population and the helper (CD4) and suppressor (CD8) subsets (Figure 1). Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function Figure 1 A study of the kinetics of CD4+ T cell recovery demonstrated that the first wave of cells is exclusively in the CD4+CD45RA-CD45R0+ memory subset. These memory cells resulted from the expansion of donor-derived naïve/memory T cells present in the inoculum. However, repopulation of naïve CD4 T cells (CD4+CD45RA+CD45R0-) followed different kinetics. Naïve cells develop from T lineage committed stem cells which undergo differentiation in the thymus and which repopulate a broad T cell repertoire. The effect of age on the naïve cell repopulation is consistent with the decrease in thymic function with age.15 The fact that early expansion of CD4 cells was not dependent on patient age supports the notion that this expansion included mostly memory cells. This explains why young recipients recovered normal levels of naïve cells after the first year while for many older patients with low thymic function, it required years to detect any naïve cells. 900 CD4 Absolute cell number/ul 800 CD8 700 B 600 NK 500 400 300 200 100 0 0 3 6 9 12 18 24 Months after transplantation Figure 1 Recovery of lymphocyte subsets over a two year post transplant period. This data, compiled from various studies, demonstrates the recovery profiles of T cell subsets. B and NK cell recovery which are also included for comparison are beyond the scope of this discussion. In the T cell compartment, CD8+ cells are reconstituted earlier than CD4+ cells. For a variety of transplant conditions, CD8+ T cells approach normal levels within the first 6 months after stem cell infusion.5-11 However, in each of these studies, CD4+T cell levels in adults remained abnormally low up to a year after transplant. One study demonstrated low CD4 levels at the 5-year follow-up.7 CD8+ T cell counts in children rebounded somewhat faster than for adults, and CD4+T cells were up to normal levels by the end of the first year after transplant.6;9;12 Several studies demonstrated greater efficiency in T lymphocyte recovery when donor HSC were derived from peripheral blood as compared to bone marrow.13 Presumably, this was due to the higher content of committed T cells available in the transplanted peripheral blood (PB) sample. In addition, transplantation of peripheral blood stem cells significantly lowered the incidence of infection13, suggesting some association between this parameter and efficient T cell recovery.10 These data indicate that this first level of phenotypic screening has provided useful preliminary information on T lymphocyte recovery following HSC transplantation. ANALYSIS OF FUNCTIONAL LYMPHOCYTE SUBSETS While quantitation of the major lymphocyte subsets indicates the initial commitment of stem cells to the lymphoid lineage, enumeration of these broad cell populations does not always correlate with the incidence of post transplant complications. The next level of analysis further dissects these major populations into subsets that are associated with specific immune functions. Following migration of lymphoid-committed stem cells, T cells maturation occurs in the thymus (Figure 2). Mature T cells are released from the thymus as naïve CD4 or CD8 cells. Acquisition of effector and memory functions occur upon antigen stimulation. Effector T cells are generally short -lived. The memory population comprises a pool of long-lived immune cells that are primed for specific responses. Figure 2 Other studies showed below normal levels of naïve cells in adults 1-5 years after transplantation.7;6 Age dependence of naïve cell recovery has been shown for different transplant variables, such as source of stem cells,9;12;16 and incidence of Graft Versus Host Disease (GVHD).16 It is important to note that these variables are all inter-related and it is often difficult to determine which variable is independent. Overall, the integrity of the thymic environment is likely to be most important factor associated with the age-dependence of naïve T cell reconstitution. Monitoring the recovery of naïve CD4+ T cell levels has become one of the standard methods for evaluating the efficacy of transplant protocols. Various studies have shown that the levels of naïve CD4 cells are higher when either cord blood or mobilized peripheral blood is the source of transplanted HSC as compared to bone marrow.10, 13, 14, 17 It is also believed that transplantation of relatively immature and naïve cord blood stem cells reduces the incidence of GVHD, thus the use of cord blood (CB) stem cells is being carefully evaluated. Naïve cell monitoring is a large component of this evaluation. The expression of CD45RA and CD45R0 was initially used as the basic phenotypic profile to distinguish naïve and memory T cell subsets, respectively. More recently, CD45RA and CD45R0 were found to overlap in different functional subsets.17; 18 Thus the combination of CD8 or CD4 and CD45RA with a variety of other markers is necessary to further discriminate functional T cells. Table 1 describes both the basic and expanded profiles that have been used to define naïve, memory and effector T cell populations. As an example, expression of CD27 on CD8 CD45RA+ cells correlated with a functionally naïve population and loss of CD27 was seen when these cells became highly differentiated19. Figure 3 illustrates an example of this expanded phenotypic analysis. Similar results were found with other marker combinations.19-20;21 22Thus, phenotypic analysis of naïve/memory cells should include CD45RA as well as other markers that refine the definition of these functional subsets.23 Table 1 Functional T Cell Subset Basic Phenotypic Profile Expanded Phenotype Profile Naïve CD4 T cells CD4+CD45RA+ or CD4+CD45R0- CD11a low CD27+ CD62L hi CCR7+ Memory CD4 T cells CD4+CD45RAor CD4+CD45R0+ CD27CD62L CCR7- Effector CD4 T cells CD4+CD45RA+ or CD4+CD45R0+ Cytokines (post-stimulation) Naïve CD8 T cells CD8+CD45RA+ or CD8+CD45R0- CD11a low CD31+ (TREC hi) CD27+ CD62L hi CCR7+ CD244/2B4- Memory CD8 T cells CD8+CD45RAor CD8+CD45R0+ CD27CD62L CCR7- Effector CD8 T cells CD8+CD45RA+ or CD8+CD45R0+ CD27CD62L low CCR7CD244/2B4+ Perforin, Granzyme B + Cytokines (post-stimulation) Activated T cells CD4+CD25+, CD69+, CD71,HLA-DR+ Effector cells (T helper and T cytotoxic) Pluripotent (HSC) stem cells →T lineage stem cells → Thymus → Naïve T cells (CD4 and CD8) Memory (CD4 and CD8) The reconstitution of functional T cell subsets has been extensively examined. Studies suggest these cells affect the incidence of post-transplant infection.10;14 The focus of many studies has been on naïve and memory T cell subsets, since the reappearance of a broad naïve T cell repertoire is thought to be necessary to respond to a lifetime of antigenic stimulation. CD8+CD25+, CD69+, CD71, HLA-DR+, CD38+ 3 low low Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function Figure 3 T CELL RECEPTOR DIVERSITY Another parameter that is increasingly useful in monitoring T cell reconstitution is T cell receptor (TCR) diversity. The ability of the immune system to protect an individual from a great variety of pathogens is dependent on a diverse TCR repertoire. Diversity is generated during T cell maturation in the thymus, by recombining TCR genes in the variable (V) regions. CDR3 Spectratyping Further phenotypic analysis CDR3 spectratyping analyzes the complexity of the complementarity-determining regions (CDR3) of the TCR Vβ. These regions are generated during gene rearrangement in the thymus and play a major role in conferring TCR diversity. The greater the size heterogeneity of CDR3 sequences demonstrated for each Vβ family, the more complex and diverse is the TCR repertoire. During the course of T cell reconstitution the number of peaks in a CDR3 spectragraph would be expected to increase as has been described in Roux et al.15 This study also demonstrated a strong correlation between the number of CDR3-complete Vβ families and the number of CD4+CD45RA+ CD45R0- T cells. Of clinical importance, an increase in naïve cells and in their diversity was necessary for patients to respond to tetanus toxoid immunization. This finding may help define more effective revaccination protocols. These data also suggests that the degree of diversity is indicative of the level of immune protection. T Cell Receptor Excision Circles (TREC) Figure 3 Functional subpopulations of T cell subsets. The definitions of naïve, memory and effector T cell populations are based upon the expression of CD45RA and CD27. During thymic TCR gene rearrangement, DNA fragments are excised in the form of circular DNA or TRECs. TRECs are stable within the cell but do not replicate and are diluted during T cell proliferation. Quantitative detection of TRECs using PCR appears to be a sensitive measurement of thymic T cell output. T cells have the largest number of circles right after rearrangement, then get diluted out by cell division as cells get further in time from thymic emigration. This measurement has been used to monitor the emergence of naïve T cells after stem cell transplantation. TREC levels have been shown to correlate with the frequency of naïve CD4 T cells and with the recovery of proliferative responses.12 5 Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function Figure 4 Tube A L Vβ5.3 Vβ9 K K Vβ17 Vβ7.1 M Vβ3 M Tube C L NonActivated CD4 Vβ13.1 Vβ5.1 K SS Vβ13.6 Vβ20 M Vβ8 PE M Vβ16 Tube D Vβ18 L K Cytometric analysis has previously limited antibody based T cell repertoire monitoring, because of the large number of cells needed to test more than 20 Vβ families. However a recent advance, which combined most of the available Vβ antibodies into 8 tubes24 has greatly improved this methodology and made it feasible to include it in the routine monitoring of immune reconstitution. Tube B CD69 L CD3 It is now possible to measure the diversity of the T cell repertoire by detection of the distinct Vβ families of the TCR β chain using multiparametric flow cytometric analysis. This approach can determine whether representation in the TCR repertoire is broad or skewed/biased. The broadest Vβ usage is indicative of the most intact immune system. The imbalance in naïve/memory T cells seen following stem cell transplantation undoubtedly contributes to a bias in Vβ usage. Figure 5 CD3 Phenotypic Analysis Of The Vβ Repertoire IFN ϒ CD8 Tube E Tube F L L Vβ5.2 Vβ23 K K Vβ2 Vβ1 M Vβ12 Vβ21.3 Tube H Vβ11 Flow cytometry offers a standardized method for the evaluation of TCR Vβ diversity that is easier, less expensive and faster than comparable molecular methods. In addition, multiparametric analysis permits the evaluation of TCR Vβ diversity within functional T cell subsets. This capability may contribute to better patient management in the evaluation of HSC transplantation and immune reconstitution. IMMUNE FUNCTION/RESPONSE The measurement of T cell responses after in vitro stimulation is often used to assess effector functions during immune reconstitution. Measurement of proliferative responses has traditionally been performed by measuring thymidine incorporation following polyclonal stimulation with mitogens (PHA, PWM or anti-CD3)7;8;9;12 or specific anti-viral and bacterial antigens.7;9;12;15 In general, it has been shown that proliferative responses correlate with the generation of naïve T cells and a high degree of diversity as found using phenotyping or molecular methods. More recently, single cell analysis of proliferation using reagents such as BrdU, PCNA, Ki67 and CFSE has become popular in an effort to eliminate radioisotope-based protocols.25 L K Vβ13.2 Activated K Vβ4 Vβ22 M Vβ14 M CD69 Tube G L CD3 Figure 4 illustrates the use of Betamark™ flow cytometry to quantitate the expression of 24 distinct TCR Vβ families in functional T cell populations. CD3 M CD4 Vβ7.2 FITC Figure 4 Analysis of TCR Vβ diversity in functional T cell subsets. Twenty four Vβ families were characterized within the naïve CD4+ T cell population as defined by expression of CD45RA and CD27. See Figure 2 This analytical approach provides a comprehensive assessment of T cell diversity within the CD4 and CD8 subsets. SS CD8 IFN ϒ Figure 5 Analysis of Intracellular IFNγ in Peripheral Blood Mononuclear Cells (PBMC). PBMC were analyzed for CD69 and IFNγ co-expression following stimulation with Staphylococcal enterotoxin B (SEB) and anti-CD28. Sample preparation and staining was identical for the non-activated control. Samples were permeabilized with IntraPrep and stained with a 5-color antibody cocktail consisting of CD8/IFNγ/CD4/CD69/CD3. 7 Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function Multiparametric flow cytometry is the method of choice in assessing the activation responses of lymphocytes, as many post stimulation events consist of up regulation of surface antigens and intracellular antigens that can be detected with monoclonal antibodies.25 Thus, measurement of CD69 and cytokine production hours after stimulation, or CD25, CD71, HLA-DR, etc. days after stimulation provides an activation profile which may reflect T cell functional status during immune reconstitution. An example of intracellular cytokine analysis is shown in Figure 5. SUMMARY Transplantation of Hematopoietic stem cells (HSC) has become a common procedure for the treatment of a number of hematological, neoplastic, metabolic and genetic disorders Following transplantation, reconstitution of immune function is achieved in stages as revealed by the enumeration of distinct lymphocyte populations. Immunophenotyping studies have shown that CD8+ lymphocytes are recovered faster than CD4+ cells. Acquisition of different immunological functions is slow and depends on many variables including source of stem cells, HSC quantity, quality of the inoculum, clinical conditions, patient age, and graft complications (GVHD, infections). Immunophenotyping by multiparametric flow cytometric analysis has been very effective in defining functional subsets of lymphocytes and has allowed the phenotypic characterization of naïve/memory and effector cells. In addition, T cell diversity can be assessed by TCR Vβ analysis using flow cytometry. This capability has led to more comprehensive immunological monitoring of grafted patients. As a result, it is now apparent that one of the most critical parameters is the re-appearance of newly generated and fully diverse naïve T cells, reflecting the availability of T lineage stem cells and the level of thymic function. Once an intact T cell compartment is phenotypically identified, functional integrity of the immune cells can be confirmed by measuring post-stimulation parameters which are indicative of responsiveness. The improved ability to monitor the course of immune reconstitution will aid in devising therapeutic strategies for HSC transplantion and post-transplant management. References (1) Cao,T.M., C.Kusnierz-Glaz, F.Valone, K.E.Stockerl-Goldstein, W.W.Hu, L.Johnston, K.G.Blume, S.Strober, and R.S.Negrin. 2001. Rapid engraftment after allogeneic transplantation of density-enriched peripheral blood CD34+ cells in patients with advanced hematologic malignancies. Cancer 91:2205-2213. (2) Atkinson K. 2000. Clinical Bone Marrow and Blood Stem Cell Transplantation. Cambridge University Press, Boston. (3) Little,M.T. and R.Storb. 2002. History of haematopoietic stem-cell transplantation. Nature Reviews Cancer 2:231-238. (4) Burt,R.K., A.Fassas, J.Snowden, J.M.van Laar, T.Kozak, N.M.Wulffraat, R.A.Nash, C.E.Dunbar, R.Arnold, G.Prentice, S.Bingham, A.M.Marmont, and P.A.McSweeney. 2001. Collection of hematopoietic stem cells from patients with autoimmune diseases. Bone Marrow Transplant. 28:1-12. (5) Douek,D.C., R.A.Vescio, M.R.Betts, J.M.Brenchley, B.J.Hill, L.Zhang, J.R.Berenson, R.H.Collins, and R.A.Koup. 2000. Assessment of thymic output in adults after haematopoietic stem-cell transplantation and prediction of T-cell reconstitution. Lancet 355:1875-1881. (6) Savage,W.J., J.J.Bleesing, D.Douek, M.R.Brown, G.M.Linton, H.L.Malech, and M.E.Horwitz. 2001. Lymphocyte reconstitution following non-myeloablative hematopoietic stem cell transplantation follows two patterns depending on age and donor/recipient chimerism. Bone Marrow Transplant. 28:463-471. (7) Fujimaki,K., A.Maruta, M.Yoshida, F.Kodama, M.Matsuzaki, S.Fujisawa, H.Kanamori, and Y.Ishigatsubo. 2001. Immune reconstitution assessed during five years after allogeneic bone marrow transplantation. Bone Marrow Transplant. 27:1275-1281. (8) Morecki,S., Y.Gelfand, A.Nagler, R.Or, E.Naparstek, G.Varadi, D.Engelhard, A.Akerstein, and S.Slavin. 2001. Immune reconstitution following allogeneic stem cell transplantation in recipients conditioned by low intensity vs myeloablative regimen. Bone Marrow Transplant. 28:243-249. (9) Small,T.N., E.B.Papadopoulos, F.Boulad, P.Black, H.Castro-Malaspina, B.H.Childs, N.Collins, A.Gillio, D.George, A.Jakubowski, G.Heller, M.Fazzari, N.Kernan, S.MacKinnon, P.Szabolcs, J.W.Young, and R.J.O'Reilly. 1999. Comparison of Immune Reconstitution After Unrelated and Related T-Cell-Depleted Bone Marrow Transplantation: Effect of Patient Age and Donor Leukocyte Infusions. Blood 93:467480. (10) Storek,J., M.A.Dawson, B.Storer, T.Stevens-Ayers, D.G.Maloney, K.A.Marr, R.P.Witherspoon, W.Bensinger, M.E.Flowers, P.Martin, R.Storb, F.R.Appelbaum, and M.Boeckh. 2001. Immune reconstitution after allogeneic marrow transplantation compared with blood stem cell transplantation. Blood 97:3380-3389. (11) Wu,C.J., A.Chillemi, E.P.Alyea, E.Orsini, D.Neuberg, R.J.Soiffer, and J.Ritz. 2000. Reconstitution of T-cell receptor repertoire diversity following T-cell depleted allogeneic bone marrow transplantation is related to hematopoietic chimerism. Blood 95:352-359. (12) Klein,A.K., D.D.Patel, M.E.Gooding, G.D.Sempowski, B.J.Chen, C.Liu, J.Kurtzberg, B.F.Haynes, and N.J.Chao. 2001. T-Cell recovery in adults and children following umbilical cord blood transplantation. Biol.Blood Marrow Transplant. 7:454-466. (13) Ottinger,H.D., D.W.Beelen, B.Scheulen, U.W.Schaefer, and H.GrosseWilde. 1996. Improved immune reconstitution after allotransplantation of peripheral blood stem cells instead of bone marrow. Blood 88:2775-2779. (14) Elmaagacli,A.H., S.Basoglu, R.Peceny, R.Trenschel, H.Ottinger, A.Lollert, V.Runde, H.Grosse-Wilde, D.W.Beelen, and U.W.Schaefer. 2002. Improved disease-free-survival after transplantation of peripheral blood stem cells as compared with bone marrow from HLA-identical unrelated donors in patients with first chronic phase chronic myeloid leukemia. Blood 99:1130-1135. (15) Roux,E., F.Dumont-Girard, M.Starobinski, C.A.Siegrist, C.Helg, B.Chapuis, and E.Roosnek. 2000. Recovery of immune reactivity after T-cell-depleted bone marrow transplantation depends on thymic activity. Blood 96:2299-2303. (16) Dumont-Girard,F., E.Roux, R.A.van Lier, G.Hale, C.Helg, B.Chapuis, M.Starobinski, and E.Roosnek. 1998. Reconstitution of the T-Cell Compartment After Bone Marrow Transplantation: Restoration of the Repertoire by Thymic Emigrants. Blood 92:4464-4471. (17) Talvensaari,K., E.Clave, C.Douay, C.Rabian, L.Garderet, M.Busson, F.Garnier, D.Douek, E.Gluckman, D.Charron, and A.Toubert. 2002. A broad T-cell repertoire diversity and an efficient thymic function indicate a favorable long-term immune reconstitution after cord blood stem cell transplantation. Blood 99:1458-1464. (18) Faint,J.M., N.E.Annels, S.J.Curnow, P.Shields, D.Pilling, A.D.Hislop, L.Wu, A.N.Akbar, C.D.Buckley, P.A.Moss, D.H.Adams, A.B.Rickinson, and M.Salmon. 2001. Memory T cells constitute a subset of the human CD8+CD45RA+ pool with distinct phenotypic and migratory characteristics. J Immunol 167:212-220. (19) Baars,P.A., L.M.Ribeiro Do Couto, J.H.Leusen, B.Hooibrink, T.W.Kuijpers, S.M.Lens, and R.A.van Lier. 2000. Cytolytic mechanisms and expression of activation-regulating receptors on effector-type CD8+CD45RA+. J Immunol 165:1910-1917. (20) Champagne,P., G.S.Ogg, A.S.King, C.Knabenhans, K.Ellefsen, M.Nobile, V.Appay, G.P.Rizzardi, S.Fleury, M.Lipp, R.Forster, S.Rowland-Jones, R.P.Sekaly, A.J.McMichael, and G.Pantaleo. 2001. Skewed maturation of memory HIV-specific CD8 T lymphocytes. Nature 410:106-111. (21) Chen,G., P.Shankar, C.Lange, H.Valdez, P.R.Skolnik, L.Wu, N.Manjunath, and J.Lieberman. 2001. CD8 T cells specific for human immunodeficiency virus, Epstein-Barr virus, and cytomegalovirus lack molecules for homing to lymphoid sites of infection. Blood 98:156-164. (22) Kimmig,S., G.K.Przybylski, C.A.Schmidt, K.Laurisch, B.Mowes, A.Radbruch, and A.Thiel. 2002. Two subsets of naive T helper cells with distinct T cell receptor excision circle content in human adult peripheral blood. J.Exp.Med. 195:789-794. (23) Speiser,D.E., M.Colonna, M.Ayyoub, M.Cella, M.J.Pittet, P.Batard, D.Valmori, P.Guillaume, D.Lienard, J.C.Cerottini, and P.Romero. 2001. The activatory receptor 2B4 is expressed in vivo by human CD8+ effector alpha beta T cells. J Immunol 167:6165-6170. (24) De Rosa,S.C., L.A.Herzenberg, L.A.Herzenberg, and M.Roederer. 2001. 11-color, 13-parameter flow cytometry: identification of human naive T cells by phenotype, function, and T-cell receptor diversity. Nat.Med. 7:245-248. (25) van den,B.R., P.P.Boor, E.G.van Lochem, W.C.Hop, A.W.Langerak, I.L.Wolvers-Tettero, H.Hooijkaas, and J.J.van Dongen. 2000. Flow cytometric analysis of the Vbeta repertoire in healthy controls. Cytometry 40:336-345. (26) Darzynkiewicz,Z.C.H.a.&.R.J.P. 2001. Cytometry - Methods in Cell Biology. Academic Press, San Diego, CA. 9 Hematopoietic Stem Cell Transplantation Reconstitution of T Cell Immune Function PRODUCT LISTING FOR IMMUNE RECONSTITUTION STUDIES MULTI-COLOR PRODUCTS FOR FLOW CYTOMETRY SINGLE COLOR PRODUCTS FOR FLOW CYTOMETRY Specificity FREEZE DRIED Application CD3 LS CD4 CD8 CD11a LS LS NME COULTER CLONE/IOTest Clone Purified UCHT1 6604629 Biotin A BL4 13B8.2 IM0115 IM0263 IM0398 IM0704 SFCI12T4D11 6602138 6602393 SFCI21Thy2D3 6602139 B9.11 IM0102 25.3 IM0157 B1.49.9 IM0119 33b3.1 IM0317 1A4CD27 IM2034 CD28 NME CD28.2 IM1376 NME 1F11 IM2052 IM0447 T16 A 6602385 NME CD45R0 NME CD62L NME CD69 CD71 IM0266 IM2635 APC PC7 IM2467 6607100 FITC RD1 ECD 6604623 6604621 IM0448 IM0451 IM0452 IM0860 IM1433 IM0477 IM0478 IM1235 IM1236 37L (T9) 6603117 A C1.7 IM1607 2B1 IM1517 B8.12.2 IM0108 A Immu-357 IL-2 EF N7.48A IL-4 EF 4D9 Ki-67 P Ki67 INF-Gamma P 45.15 PCNA P 5A10 TNF-Alpha EF 188 IM2646 6607107 IM2071 6607111 6607108 IM1832 IM2651 6604928 IM0584 IM1834 IM1247 IM1307 IM1230 IM1231 6603904 6603866 IM2712 IM2214 IM2713 Part Number FITC PE/RD1 ECD PC5 LS 6607013 X X X X PC5 CD45/56/19/3 LS 6607073 X X X X 6607010 CD8/4/3 LS 6607053 X X X CD45//4/3 LS 6607015 X X X CD45/8/3 LS 6607017 X X X CD8/4/3 LS 6607103 X X X CD62L/45RA/4 NME 6607104 X X X CD62L/45RA/8 NME 6607105 X X X CD62L/45R0/8 NME 6607106 X X CD8/4/3 LS IM3485 X X X CD16/56/3 LS IM3487 X X X CD25/4/3 LS IM3486 X X X CD3/4/45v LS IM1651 X X X CD3/8/45 LS IM1670 X X X CD4/8/3 LS IM1650 X X X CD4/8/45 LS IM1653 X X X CD3/4 LS 6604929/IM1382/IM1287 X X CD3/8 LS 6604930/IM1310/IM1383 X X CD4/8 LS 6604614/IM0747/IM1385 X X CD4/CD45RA NME 6603800 X X CD8/CD4 LS 6603802/IM1379 X X IM1943 6607110 IM0482 IM0483 IM0462 IM0463 IM1638 6602924 IM2667 X X A IM1295/IM2053/IM1390 X X CD8/38 A IM2695 X X CD38/8 A IM2673 X X IM2656 HLA-DR/3 A IM1300 X X HLA-DR/8 A IM1199 X X IM2658 IM0464 IM1639 IM3636 IM2659 MULTI-COLOR PRODUCTS FOR FLOW CYTOMETRY IM3635 6602920 IM0109 6603140 6603424 A 6603450 Specificities Application Part Number IOTest Beta MarkTCR Vβ Repertoire Kit D M3497 6604366 IM2718 IM1316 IM2719 MISCELLANEOUS PRODUCTS IM2716 IM2717 IM1510 IntraPrep Permeabilization Reagent IM2388/IM2389 Flow-Count Fluorospheres 7547053 IM3279 Activation Naive, Memory Effector Proliferation LS Lymphocyte Subsets EF Effector Function D Diversity 11 PC7 X IM2001 IM1608 IM0261 CD3/25 CD3/HLA-DR IM2655 6604077 P BL2 IM0479 6607112 IM1246 IM0780 BrdU 9-49 (I3) IM2469 6602944 IM2117 A 6603862 6603850 6604727 6607102 6603181 IM2711 IM0537 YDJ1.2.2 “HLA-DR,DP,DQ” IM2638 IM2371 DREG56 A 6607101 IM1431 IM0775 SFCI28T17G6 (TQ1) TP1.55.3 IM2468 IM2409 UCHL1 A IM2636 IM2578 LS198-4-3 ALB11 IM0449 IM0481 H279 (I2) P PC5 IM2705 6604422 IM0366 CD244 HLA-DR ECD IM1282 6603861 6603848 6604728 6607011 IM0450 2H4LDH11LDB9 (2H4) CD45RA PE/RD1 6602864 5.6E CD38 FITC 6603200 NME CD31 Purified IM0178 CD27 A Application CD45/4/8/3 CYTOSTAT 6604701 1HT44H3(IL2R1) CD25 FITC IM1301 6604625 6604629 IM1281 HIT3a X35 NME Specificities LIQUID