Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Extracellular matrix wikipedia , lookup
Cell growth wikipedia , lookup
Tissue engineering wikipedia , lookup
Cell culture wikipedia , lookup
Cellular differentiation wikipedia , lookup
Organ-on-a-chip wikipedia , lookup
Cell encapsulation wikipedia , lookup
Morphology of Single Ganglion Cells in the
Glaucomatous Primate Retina
Arthur J. Weber,1 Paul L Kaufman,2 and William C. Hubbard2
examine the degenerative effects that prolonged elevation of intraocular pressure
GOP), a risk factor commonly associated with glaucoma, has on the morphology of single ganglion
cells in the primate retina.
PURPOSE. TO
The monkey model of glaucoma was combined with intracellular staining techniques
using an isolated retina preparation. Midget and parasol cells from normal and glaucomatous eyes
were labeled intracellularly, and their axons, somas, and dendritic fields were compared using
confocal microscopy.
METHODS.
In midget and parasol cells, the earliest signs of pressure-induced degeneration involved
structural abnormalities associated with the dendritic arbor. Reductions in axon thickness appeared
later, with changes in soma size occurring concomitantly or slightly later. Chronic elevation of IOP
resulted in a significant decrease in the mean soma sizes of midget and parasol cells, but only
parasol cells showed a significant reduction in dendritic field size and axon diameter. Comparisons
of eyes with different levels of optic nerve damage, based on cup- disc ratio, showed that the axons
and dendritic fields of parasol cells were significantly smaller at lower cup- disc ratios than were
those of midget cells, suggesting a possible differential effect.
RESULTS.
CONCLUSIONS. In glaucoma, retinal ganglion cells undergo a pattern of degeneration that originates
with the dendritic arbor and ends with shrinkage of the cell soma. Although this pattern of
degeneration implies early functional deficits and retinal ganglion cell atrophy that occurs earlier
than previously thought, based on ganglion cell loss alone, it also suggests a window of opportunity
for effective neuroprotection. (Invest Ophthalmol Vis Sci. 1998;39:2304-2320)
laucoma is a disease of the visual system that, in many
cases, is characterized by an elevation of intraocular
pressure (IOP), progressive changes in the appearance
of the optic disc and retinal nerve fiber layer, and visual field
defects. Although several investigators have described the degenerative effects that chronic elevation of IOP and glaucoma
have on fibers in the optic nerve1"6 and the concomitant loss
of ganglion cells that occurs within the retina itself,2'7"12 the
morphologic changes that characterize the atrophy of single
ganglion cells in the glaucomatous eye remain unknown.
These data are important, because the spatial and temporal
processing of visual information by retinal ganglion cells depends on their structural integrity.1314 In addition, an understanding of the pattern of glaucomatous neuropathy that occurs at the single-cell level will benefit ongoing studies
conducted to develop neuroprotectant-based treatment strategies.
From the 'Department of Anatomy, Neuroscience Program, Center for Clinical Neuroscience and Ophthalmology, Michigan State University, East Lansing; and the 2 Department of Ophthalmology and
Visual Sciences, University of Wisconsin, Madison.
Supported in part by Alcon Laboratories, Fort Worth, Texas
(AJW); American Health Assistance Foundation (AJW); and Grants
EY11159 (AJW), EY02698 (PLK), and RR00167 to the Wisconsin Regional Primate Research Center, Madison, Wisconsin.
Submitted for publication March 21, 1998; revised June 18, 1998;
accepted July 17, 1998.
Proprietary interest category: N.
Reprint requests: Arthur J. Weber, Department of Anatomy, B512
W. Fee Hall, Michigan State University, East Lansing, MI 48824.
Although it is possible to identify, based on soma size and
dendritic field architecture, several different types of ganglion
cells in the primate retina, the midget and parasol cells have
been described most completely.13"29 In brief, midget cells
represent approximately 80% of the ganglion cells in the primate retina, they have medium-sized somas, and their small- to
medium-sized dendritic trees often originate from a single
dendrite that then gives rise to a compact, bushy dendritic
arbor. The axons of midget ganglion cells project to the dorsal,
parvocellular, layers of the lateral geniculate nucleus (LGN),
and they represent the P-pathway of the primate visual system.
Functionally, these neurons have small receptive fields and
more slowly conducting axons than parasol cells, and they
respond best to chromatic stimuli of high spatial and low
temporal frequency. Parasol cells represent approximately 10%
of the total population of ganglion cells in the primate retina.
At all retinal eccentricities, the somas and dendritic fields of
these neurons are among the largest in the ganglion cell layer,
and their dendritic trees often originate from three to four
thick primary dendrites that branch regularly and form a radially symmetrical arbor. The axons of parasol cells typically are
larger than the axons of midget ganglion cells. Parasol cells
project to the ventral magnocellular layers of the LGN, and
they represent the M-pathway of the primate visual system.
Functionally, parasol cells have large receptive fields with rapidly conducting axons, and they respond best to achromatic
stimuli of high temporal and low spatial frequency.
To examine the morphology of midget and parasol cells in
the glaucomatous eye, we combined the monkey model of
experimental glaucoma31"34 with intracellular staining tech-
2304
Investigative Ophthalmology & Visual Science, November 1998, Vol. 39, No. 12
Copyright © Association for Research in Vision and Ophthalmology
G
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
Retinal Ganglion Cell Degeneration in Glaucoma
IOVS, November 1998, Vol. 39, No. 12
2305
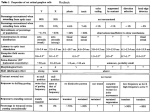
TABLE 1. Summary of Animals Studied
Animal No.
Sex
M81102
AE96
AA02
M86005
W84
M80085
M79047
AM92
M1903
AE05
M88081
M80142
M1799t
M1755*
M
F
F
M
M
M
M
Age (yr)
M
F
F
M
M
F
F
11
15
Mean IOP
(mmHg)*
Peak IOP
(mmHg)
46 ± 17
44 ± 21
62
58
72
52
78
6
62 ± 9
46 ± 9
63 ± 19
54 ± 12
27 ± 12
40 ± 12
25 ± 8
26 ± 7
37 ± 10
14
36 ± 9
9
32 ± 15
24 ± 11
25 ± 12
18
8
19
13
13
8
8
17
10
76
45
66
55
42
52
61
66
53
54
Duration
(wk)
2.5
2.5
4
4
4
8
9
12
12
16
16
16
32
49
Cup/Disc Ratio
(initial/final)
0.2/0.9
0.3/0.9
0.3/0.9
0.3/0.8
0.2/1.0
0.2/0.8
0.2/1.0
0.2/0.4
0.3/0.4
0.3/0.5
0.3/0.8
0.3/0.6
0.3/0.9
0.2/0.4
0.3/0.5
IOP, intraocular pressure.
* Values are means ± SD.
t Laser and microsphere treatment.
t Bilateral microsphere treatment.
niques. A major advantage to this approach compared with
more conventional staining techniques is that it permits visualizing not only the cell body, but also the intraretinal axon and
entire dendritic arbor of each labeled neuron. These data are
important not only for accurate classification of ganglion cells
in the primate retina, but also because they provide a broader
range of anatomic features for use in the identification of
glaucoma-related changes in ganglion cell morphology.
MATERIALS AND METHODS
Subjects and Procedures
Fourteen rhesus monkeys (Macaca mulatto) of both sexes,
aged 6 to 19 years, were used in this study (Table 1). All had
clinically normal-appearing eyes, determined by slit lamp
biomicroscopy, gonioscopy (using a lens by Carl Zeiss,
Oberkochen, Germany) and stereoscopic funduscopy (fundus
camera by Zeiss or Topcon, Tokyo, Japan) and all had baseline
intraocular pressure, measured under ketamine HC1 anesthesia
with either a tonometer (minified Goldman30) or (Tono-pen
XL; Mentor O&O, Norwell, MA), below 21 mm Hg (normal IOP
for ketamine-anesthetized rhesus monkeys, 10-20 mm Hg).31
Topical 0.5% proparacaine HC1 (Alcaine; Alcon Laboratories;
Fort Worth, TX) was used for all procedures involving contact
with the cornea, and dilation of the pupils for fundus photography was achieved with 2.5% phenylephrine HC1 (Mydfrin,
Alcon) and 1% tropicamide HC1 (Mydriacil, Alcon). All procedures were approved by the Animal Care Committees of the
University of Wisconsin, Madison, and Michigan State University, East Lansing, and all adhered to the ARVO Statement for
the Use of Animals in Ophthalmic and Vision Research. Although animal M1755 had a bilateral elevation of IOP, optic
disc evaluation and close behavioral observation indicated that
the well-being of the animal was not affected adversely. At the
time of death, the cup- disc (C-D) ratios of the left and right
eyes had increased only slightly (from 0.2 and 0.3 to 0.4 and
0.5, respectively), the optic discs showed normal color, and
the isolated retinas contained a large complement of retinal
ganglion cells.
In 12 animals, chronic elevation of IOP and experimental
glaucoma were induced by argon laser scarification of the
trabecular meshwork.31"33 Each animal first was anesthetized
with 10 mg/kg ketamine HC1 intramuscularly, supplemented
with 5 mg/kg as needed, and sedated with 1 mg/kg diazepam
intramuscularly. A standard clinical argon laser (model 900;
Coherent, Palo Alto, CA) and slit lamp delivery system then was
used to produce a series of focal lesions to the trabecular
meshwork in one eye (50-250 spots, 50-jiim spot diameter,
1-1.5 W, 0.5 seconds' duration). Intraocular pressure was
monitored for 2 to 3 weeks after treatment, and if not consistently 25 mm Hg or more, additional laser treatments were
performed until stable ocular hypertension was achieved. The
opposite eye served as a normal control (additional normal
eyes obtained through the Wisconsin Regional Primate Research Center Tissue Distribution Program, Madison, WI).
In the remaining two animals, IOP was elevated by injecting 100 jul sterile aqueous solution containing approximately
3-99 X 105 latex microspheres (10-/i,m diameter; Molecular
Probes, Eugene, OR) into the anterior chamber of each eye. 34
Injections were made using a 30-gauge needle and a transcorneal approach that resulted in little, if any, backflow. Generally,
8 to 10 injections were needed to produce an initial sustained
elevation of IOP. The frequency of additional injections, and
determination of the volume of beads to be injected, was made
based on biweekly measurements of intraocular pressure.
Approximately once a week after laser treatment and
twice a week after the initial injection of latex microspheres,
the normal and treated eyes were examined with a slit lamp
(Zeiss), noting corneal clarity and cells and flare in the anterior
chamber. After measurement of IOP, the anterior chamber
angle and optic nerve head were examined with a goniolens
(Zeiss, or OG3M-13; Ocular Instruments, Bellevue, WA). Fundus photographs were obtained approximately every 3 to 4
weeks, depending on the clinical appearance of the optic disc
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2306
Weber et al.
compared with its appearance in the previous eye examination.
After periods of elevated IOP that ranged from 2.5 weeks
to 49 weeks, the animals were anesthetized deeply with 15
mg/kg ketamine HC1 intramuscularly, followed by an intravenous injection of 35 mg/kg pentobarbital sodium. The eyes
then were removed quickly, and the animal received an overdose of pentobarbital sodium and was perfused transcardially
with 0.5 1 of 0.9% saline followed by 1 1 of 10% formol-saline
solution. The brains were removed and postfixed for future
histologic examination of the LGN.35
In Vitro Procedures and Tissue Processing
Immediately on enucleation, the anterior segment of each eye
(from the ora serrata forward) was removed with a pair of fine
scissors and the posterior eyecup placed in a solution of artificial cerebrospinal fluid (pH 7.4)36 saturated with a mixture of
95% O2 and 5% CO2 at room temperature. The vitreous body
was removed and the retina isolated. Care was taken to avoid
mechanical stress, especially near the fovea where the retina is
very thin. The retina then was flattened and placed ganglion
cell layer up in a plexiglass chamber also perfused with 6
ml/min to 8 ml/min oxygenated artificial cerebrospinal fluid.
The tissue was held submersed in the chamber by a small nylon
net, and the chamber was mounted on the stage of an upright
microscope equipped with epifluorescence. A neutral density
filter (ND4; Nikon, Tokyo, Japan) was used to reduce the
intensity of the mercury vapor light reaching the tissue. Single
ganglion cells were viewed using a 40 X water immersion
objective (numerical aperature 0.55; Nikon) with a working
distance of 1.6 mm. Periodically, a few drops of a 1 mM
solution of the vital dye acridine orange (catalog no. A-4921;
Sigma, St. Louis, MO) was added to the tissue chamber to aid in
visualizing single ganglion cells. 18 ' 20
Intracellular injections of single retinal ganglion cells were
made using glass microelectrodes and a four-axis hydraulic
micromanipulator attached to the microscope stage. Glass micropipettes were pulled on a micropipette puller (Flaming/
Brown, model P-87; Sutter Instruments, Novato, CA) and filled
with a solution of 3% Lucifer yellow CH (catalog no. L-0259;
Sigma) in 0.1 M LiCl (pH 7.6). For injection, single retinal
ganglion cells were first positioned in the center of the microscope field and the dye-filled electrode was lowered into position adjacent to the cell body. Each cell then was impaled by
slowly advancing the electrode along its axis until the tip of the
electrode was seen to penetrate the cell's membrane. Complete filling of the sorna, dendritic tree, and from 1 mm to 2
mm of the cell's intraretinal axon segment was achieved by
passing a negative current (1-5 nA) through the electrode.
Typically, 1 to 2 minutes was sufficient to label completely the
dendritic trees of midget and parasol cells. The progress of
each intracellular injection was monitored visually, with care
taken to minimize the amount of time that individual cells were
exposed to the mercury vapor light. After the last cell was
injected, the retina was removed from the injection chamber
and immersion-fixed in 4.0% paraformaldehyde in 0.1 M sodium phosphate buffer (pH 7.4). Each retina then was rinsed
with 0.1 M sodium phosphate buffer, wholemounted on a
gelatinized glass slide, dehydrated, defatted, and protected
with a coverslip.
IOVS, November 1998, Vol. 39, No. 12
Sampling, Classification, Mapping, and
Morphologic Analysis of Retinal Ganglion Cells
Because the intracellular approach does not permit the injection of a large number of neurons at every location in each
retina studied, we focused our morphologic examination on
ganglion cells located in the superior and inferior regions of the
midperipheral temporal retina (—2-7 mm, ~10°-35°, from the
fovea), the area considered clinically to be most vulnerable to
glaucoma-related neuronal damage.337"39 In addition, we restricted our analysis to only those labeled cells that, based on
anatomic comparisons with other intracellular studies in the
primate retina,18"20'24'40'41 we considered to be midget and
parasol cells.
Because retinal ganglion cell size varies with retinal eccentricity,15"24 the position of each labeled ganglion cell relative
to the location of the optic disc and fovea was recorded using
a microscope-based digitizing system (Minnesota Datametrics,
St. Paul, MN). This retinal map also served as a guide for the
reconstruction of each labeled ganglion cell using a confocal
microscope (MRC 600 Lasersharp; Bio-Rad, Richmond, CA).
Measurements of cell soma, dendritic field area, and axon
diameter at a point approximately 5 jam to 10 /xm from the cell
body, were made directly from the confocal images (projected
z-series; resolution, 0.1-0.5 /xm/optical section) using the morphometric software of the confocal system. Somal area was
determined by tracing the maximum cell body outline of each
optically reconstructed neuron, and dendritic field size was
obtained by measuring the enclosed area formed by connecting the distal tips of each neuron's dendritic processes.20
Measurements for each experimental group, normal versus
glaucoma, were pooled, and all mean data comparisons are
presented as means ± 1 SE. Soma and dendritic field size
distributions were compared using the Mann-Whitney test,
and differences in mean soma, axon, and dendritic field sizes
were evaluated with a two-tailed Student's f-test. All statistical
analyses were performed using commercially available statistical software (SPSS, Chicago, IL), with P = 0.05 used as the level
of significance.
RESULTS
A total of 1298 intracellularly labeled retinal ganglion cells,
judged by visual inspection to be filled completely, were analyzed in this study. Of these, 518 cells (111 midget and 407
parasol) were injected in normal retinas, and 780 ganglion cells
(236 midget and 544 parasol), were labeled in glaucomatous
eyes.
Qualitative Observations
Parasol Cells. Confocal images of parasol cells that were
labeled intracellularly in the normal primate eye are shown in
Figure 1. In agreement with previous studies,13"18'20"24 these
neurons have large cell bodies; large, radially oriented dendritic trees that originate from three to four primary dendrites;
and thick proximal axon segments. In addition, their dendritic
processes branch regularly, and they show a progressive decrease in size with increased branching and distance from the
cell soma. Although the main dendrites of most normal parasol
cells had a relatively smooth appearance, it was not uncommon to see numerous fine dendritic appendages associated
with the arbors of these cells.20
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
Retinal Ganglion Cell Degeneration in Glaucoma
IOVS, November 1998, Vol. 39, No. 12
A
1
<-•
ri
'-.
•"/
2307
B
FIGURE 1.
(A through F) Confocal images of intracellularly labeled neurons showing the range
of morphologic features that characterize the somas, dendritic fields, and intraretinal axon
segments {arrowheads) of parasol cells from the normal eye. Scale bars, 25 /xm.
The photomicrographs in Figure 2 outline the range of
morphologic features characteristic of parasol cells from glaucomatous eyes. The cells shown are from six animals, and they
are arranged based on increasing C-D ratios for the eyes from
which they were obtained. The cell in Figure 2A was injected
in the superior-temporal retina (—6.6 mm from the fovea) of an
eye that had had a mean IOP of 36 mm Hg for 16 weeks. At the
time of death, the nasal and temporal regions of the disc
showed normal color, the C-D ratio had increased from 0.3 to
0.6, and the disc was slightly more cupped superiorly than
inferiorly. Despite these changes, however, the soma, dendritic
field, and axon (arrowhead) of this cell are normal in size and
appearance for parasol cells at this retinal location. The cell in
Figure 2B also was injected in the superior-temporal retina of
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2308
Weber et al.
A
IOVS, November 1998, Vol. 39, No. 12
B
FIGURE 2. Confocal images showing the range of morphologic features that characterize
parasol cells from eyes with increasing degrees of optic disc cupping. (A, B) Mild; (C, D)
moderate; (E, F) severe. The earliest changes occurred at the level of the dendritic tree.
Arrowheads indicate intraretinal axon segments, arrows indicate dendritic abnormalities (see
the Results section). Scale bars, 25 M-m-
an eye that had had the pressure elevated for 16 weeks, but in
this eye the mean IOP was only 26 mm Hg. Although the disc
was pink at death, the C-D ratio had nearly doubled (0.5 versus
0.3)- Although the soma, axon, and dendritic arbor of this
neuron also were normal in size, its dendritic processes
showed more variability in thickness (arrows) than in the
normal cells (Fig. 1) or in the neuron shown in Figure 2A. The
parasol cell in Figure 2C was injected in the superior-temporal
retina (~3.4 mm from the fovea) of an eye that had had a mean
IOP of 46 mm Hg for 1 month. At the time of death the disc had
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
Retinal Ganglion Cell Degeneration in Glaucoma
2309
good color but was deeply cupped, having progressed from a
C-D ratio of 0.3 to 0.8. In addition, there was a small hemorrhage in the superior-temporal region of the disc. Although the
cell body, axon, and dendritic tree of this neuron are normal in
size for its retinal location, the proximal portion of one primary
dendrite (arrow) is abnormally thin compared with its distal
segment. In addition the cell body does not have the smooth,
round shape exhibited by the other parasol cells. The cell in
Figure 2D, similar to that in Figure 2A, was injected in the
superior-temporal region of an eye that had had a mean IOP of
37 mm Hg for 16 weeks. Unlike the cell in Figure 2A, however,
the C-D ratio of the eye from which this cell was recovered
had increased from a baseline value of 0.3 to 0.8 at the time of
death, and the temporal region of the disc was paler than the
nasal region. Although the cell's overall appearance was not
abnormal, some of its higher order dendrites were thinner than
their parent processes (arrows). The axon of this neuron also
could be seen to undergo an abrupt decrease in thickness
(arrowheads).
The parasol cells shown in Figures 2E and 2F are from eyes
with C-D ratios of 0.9. The cell in Figure 2E was injected in the
superior-temporal retina (~4.5mm from the fovea) of an eye
with an IOP averaging 46 mm Hg for only 2.5 weeks. At the
time of death, the nerve head was deeply cupped, and the
temporal region of the disc was pale. Although the size and
general organization of the cell's dendritic field are similar to
those of normal parasol cells at this retinal location, several
structural abnormalities can be seen. In particular, unlike normal parasol cells (Fig. 1), the dendrites of this neuron did not
show a progressive decrease in size with increased branching
and distance from the cell soma. Instead, most of this neuron's
primary dendrites were uniformly large and clublike, undergoing abrupt changes in diameter at distal branch points and
giving rise to thin, wispy terminal dendritic processes. In addition, although the cell displayed a normal, spherical-shaped
soma, the cell body was smaller than that of most normal
parasol cells found at this retinal location and smaller than that
of cells containing a dendritic arbor of comparable size. Further, the cell's proximal axon (arrowhead) was abnormally
thin, measuring only half the mean thickness of axons of
normal parasol cells with comparable-sized somas (0.75 jam
versus 1.5 (xm). The parasol cell in Figure 2F is from the
superior-temporal retina of a glaucomatous eye that had had a
mean IOP of 42 mm Hg for 8 weeks. At time of death, the eye
had a cup/disc ratio of 0.9, the disc was deeply cupped, and
the temporal region of the disc was paler than the nasal region.
Although the somas, dendritic arbor, and proximal axon (arrowhead) of this neuron were normal in size for its retinal
location (—5.5 mm from the fovea), the primary dendrites of
this neuron were abnormally thin, and the distal dendritic
processes showed considerable variability in thickness.
Midget Cells. Examples of normal midget ganglion cells
are shown in the confocal images in Figure 3- In contrast with
normal parasol cells (Fig. 1), these neurons were characterized
by their small cell bodies, smaller and more compact dendritic
arbors, and relatively thin proximal axon segments. In addition,
the dendritic trees of most midget cells originate from a single
primary dendrite, and they typically are not radially symmetrical around the cell body. Further, the dendritic arbors of
midget ganglion cells contain finer processes that are more
variable in size and length than are the dendritic processes of
parasol cells.13"24
The confocal images in Figure 4 show the range of morphology associated with midget ganglion cells injected in the
temporal retinas of eyes with glaucoma. The cells shown were
from four different eyes and again were arranged based on
increasing C-D ratios for their respective eyes. The midget
cells in Figures 4A and 4B were injected in the inferior-temporal retina of the same eye as the parasol cell shown in Figure 2A
(mean IOP, 36 mm Hg for 16 weeks; C-D, 0.6). Similar to the
parasol cell, the somas, dendritic arbors, and axons (arrowheads) of these neurons were normal in size and appearance
for midget cells at this retinal location (~6.8 mm from the
fovea). The midget cells in Figures 4C and 4D were injected in
the inferior-temporal retina of an eye that had had a mean IOP
of 54 mm Hg for 8 weeks. At time of death, the disc was deeply
cupped (C-D, 0.8), but showed good color. Although both
neurons displayed considerable variability in the thickness of
their dendritic appendages, their somas, dendritic fields, and
axons were normal in size and appearance.
The midget cell in Figure 4E is from the inferior-temporal
retina of an eye that had a mean IOP of 27 mm Hg for
approximately 9 weeks. Despite the relatively modest IOP
elevation, at time of death the C-D ratio had increased from 0.2
to 1.0, there was undermining of the rim superiorly, and the
temporal region of the disc was very pale. Although the soma
of this neuron was comparable in size with that of the normal
midget cell shown in Figure 3A, its dendritic arbor was highly
abnormal, being reduced to only a few thin, sparsely branched
processes. In addition, the axon was very thin compared with
that of other midget cells of comparable soma size. Similar to
the cell in Figure 4E, the midget ganglion cell shown in Figure
4F was from a glaucomatous eye that had a final C-D ratio of
0.9. This cell, however, was injected in the superior-temporal
retina of an eye that had a mean IOP of 44 mm Hg for only 2.5
weeks. Although the cell's general morphology was similar to
that of the normal midget cell shown in Figure 3A, the primary
dendrite was abnormally thin and gave rise to numerous irregular swellings that were connected by extremely fine processes. Although the soma and dendritic field of this neuron
were within the normal size range, they were smaller than
most midget ganglion cells at this retinal location, as was the
diameter of its axon.
Quantitative Observations
Ganglion Cell Soma Sizes in Normal and Glaucomatous Eyes. Parasol Cells. The histograms in Figure 5A illustrate
the distributions of parasol cell soma cross-sectional areas sampled in the midtemporal retinas of the normal (upper histogram) and glaucomatous (lower histogram) eyes studied. Although the normal parasol cells had somas that ranged from 75
jam2 to 500 jam2, approximately 90% of these neurons had
somas that were within the narrower range of 100 jam2 to 350
jam2 consistent with findings in previous studies of normal
parasol cells in this area of the retina.20 Similarly, parasol cells
injected in glaucomatous eyes had somas that ranged from 50
/am2 to 550 jam2, with 86% having cross-sectional areas between 75 /am2 and 300 jam2. However, in proportion to the
total number of ganglion cells, relatively more parasol cells
with somas 200 jam2 or less were found in the retinas of
glaucomatous eyes than in normal eyes. This resulted in a
skewed distribution of glaucoma-related parasol cell soma
sizes, and a statistical difference (P < 0.001) from the distribution of normal parasol cell soma sizes. The mean soma sizes
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2310
Weber et al.
A
IOVS, November 1998, Vol. 39, No. 12
B
>:>**
3. (A through F) Confocal images showing the range of morphologic features characteristic of normal midget ganglion cells. Arrowheads indicate intraretinal axon segments.
Scale bars, 10 /am.
FIGURE
of parasol cells in normal and glaucomatous eyes (Fig. 5B) also
were significantly different (JP < 0.001), with parasol cells in
the glaucomatous eyes being approximately 13% smaller than
normal. When compared at different retinal eccentricities (Fig.
5C), the mean soma sizes of parasol cells in glaucomatous eyes
were consistently smaller than those of normal cells. This
reduction in cell body size was significant for parasol cells
located 4 mm to 5 mm (23.3%) and 5 mm to 6 mm (15-7%)
from the fovea (4-5 mm: P < 0.001; 5-6 mm: P < 0.01). The
histograms in Figure 5D compare the mean soma sizes of
parasol cells from normal eyes with cells from glaucomatous
eyes that have different C-D ratios. In all cases, the glaucomatous eyes had baseline C-D ratios of 0.3 or less (Table 1).
Although parasol cells from eyes considered to be in the early
stage of the disease process (C-D, 0.4-0.6) had somas that
were actually slightly larger (7.5%) than normal (P < 0.01),
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
Retinal Ganglion Cell Degeneration in Glaucoma
2311
B
•
•
•
*
•
'
:
r'
Jro
FIGURE 4. Confocal images showing the morphologic changes that characterize midget
ganglion cells from eyes with different levels of optic nerve damage. (A, B) Mild; (C, D)
moderate; (E, F) severe. Arrowheads indicate intraretinal axon segments. Scale bars, 10 ju-m.
cells from eyes with C-D ratios of 0.6-0.8 were not different
from normal cells, and cells in eyes with C-D ratios more than
0.8 were significantly smaller (43.2%) than normal (P < 0.001).
Midget Cells. Most of the midget ganglion cell somas in
normal eyes (Fig. 6A, upper) had the same size range as that of
midget cells injected in glaucomatous eyes (Fig. 6A, lower),
with approximately 80% to 85% of the cells in each group
having cross-sectional areas that ranged from 75 /nm2 to 200
fxm2, again consistent with findings in studies of midget ganglion cells in this area of the retina.20 Although the distribution
of soma sizes for midget cells in the glaucomatous eye was
slightly broader than that for normal midget cells, the two
distributions were not significantly different (P = 0.09). Nevertheless, the mean soma sizes of midget ganglion cells in the
glaucomatous eye were significantly smaller (12.5%; P < 0.01)
than those of midget cells in the normal eye (Fig. 6B). This
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
250 -i
Normal: N=407
p<0.001
200 -
<
2 150
<
<
| 100
Z
<
w
S
50 H
20
10
15 20 25 30 35 40 45
50 55 60
NORMAL GLAUCOMA
2
CROSS-SECTIONAL AREA (xlOum )
B
350 -.
300
n
p<0.01
300 -
250 -
113
250 200 -
pO.001
127
200 -
p<0.001
150 -
150 -
O
C/D
100 -
100 -
<
w
S
Normal
Glaucoma
50 -
50 N=
407
201
155
NORMAL
0.4-0.6
0.6-0.8
0
2-3
3-4
4-5
5-6
6-7
ECCENTRICITY (mm)
D
0.8-1.0
CUP-DISC RATIO
FIGURE 5- Soma size comparisons for parasol cells from normal (open) and glaucomatous (batched) eyes. In general, the somas
of parasol cells from glaucomatous eyes were significantly smaller than normal (A, B). This difference was most pronounced in cells
in the midperipheral temporal retina (C) and in those from eyes with severely cupped (cup-disc, 0.8-1.0) optic discs (D).
difference existed primarily in midget ganglion cells located 2
mm to 4 mm from the fovea (Fig. 6C). As with parasol cells, the
mean cross-sectional areas of midget cells from glaucomatous
eyes with C-D ratios less than 0.8 were not significantly different from that of normal cells (P > 0.2), but midget ganglion
cells from eyes with C-D ratios more than 0.8 had somas that
were significantly smaller than normal (P < 0.001), with the
magnitude of difference being comparable in the two classes of
cells (parasol, 43.2%; midget, 45.8%).
Ganglion Cell Dendritic Field Sizes in Normal and
Glaucomatous Eyes. Parasol Cells. A comparison of the size
distributions of the dendritic fields of parasol cells from normal
and glaucomatous eyes is shown in Figure 7A. Similar to parasol cell somas (Fig. 5A), the mode of the distribution representing the dendritic field sizes of parasol cells from glaucomatous
eyes was shifted toward sizes smaller than those of normal
parasol cells, and the distributions were statistically different
(P < 0.001). Similarly, the mean dendritic field sizes of parasol
cells from glaucomatous eyes were significantly smaller (14.7%;
P < 0.001) than those of neurons sampled from comparable
regions of normal retinas (Fig. 7B).20 This difference was most
consistent and significant in cells located farther than 4 mm
from the fovea (Fig- 7C). Compared across eyes with different
C-D ratios (Fig. 7D), the dendritic fields of parasol cells in
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
Retinal Ganglion Cell Degeneration in Glaucoma
IOVS, November 1998, Vol. 39, No. 12
2313
Normal: N=l 11
200 -\
I 150 <
p<0.01
a
< 100 -
o
2
W
10
15
20
25
30
35
40
50 -I
45
NORMAL
GLAUCOMA
B
CROSS-SECTIONAL AREA (xlOum )
200 -i
200 -
43
25
18
31
.5
49
16
150 -
150 -
100 -
V
p<0.01
40
50 -
p<0.001
100 -
48
50 -
—» — Normal
p=0.05
- O — Glaucoma
N=
111
92
80
NORMAL
0.4-0.6
0.6-0.8
0 2-3
3-4
4-5
5-6
6-7
0.8-1.0
CUP-DISC RATIO
ECCENTRICITY (mm)
FIGURE 6. Comparisons of the soma sizes of midget ganglion cells from normal (open) and glaucomatous (hatched) eyes. On
average, the somas of midget cells from glaucomatous eyes were smaller than normal (A, B). This difference was greatest in the
central retina (C) and in eyes with deeply cupped (cup-disc, 0.8-1.0) optic discs (D).
glaucomatous eyes were 24.9% smaller than normal in eyes
with C-D ratios of 0.6 to 0.8 and 42.4% smaller than normal in
eyes with C-D ratios more than 0.8 (both: P < 0.001).
Midget Cells. The size distributions of the dendritic arbors
of midget ganglion cells in normal and glaucomatous monkeys
are shown in Figure 8A. As noted by others, and shown in the
photomicrographs of Figures 1 to 4, the dendritic arbors of
midget ganglion cells in the primate retina were much more
compact than those of parasol cells. This morphologic difference was reflected in the nearly 10-fold difference in the size
distributions for these two classes of neurons (Fig. 8A versus
Fig. 7A; note scales). Although more than 75% of the midget
cells sampled in normal and glaucomatous eyes had dendritic
fields less than 200 jam2 in area, cells with arbors as large as
4000 jam2 were measured in both groups of eyes. 20 No significant differences were found between die dendritic field size
distributions or the mean dendritic field sizes (Fig. 8B), of
midget ganglion cells injected in normal and glaucomatous
eyes (P > 0.5 for both). Unlike parasol cells, no consistent or
significant difference was found in the dendritic field sizes of
midget cells within the range of retinal eccentricities studied
(Fig. 8C). As with soma size, the dendritic fields of midget
ganglion cells from eyes with C-D ratios less than 0.8 were not
different from normal, whereas those from eyes with severe
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
15000
Normal: N=407
•IELD A REA
1
12000
pO.OOl
9000
y
•END]
6000
Q
3000
w
20
10
15
20
25
30
35
40
45
50
NORMAL
GLAUCOMA
B
CROSS-SECTIONAL AREA (xlOOOum )
25000 -|
15000 -i
< 20000 -
12000 -
3 15000 \
E
9000 -
E IOOOO -
6000 -
a
p<0.001
p<0.001
y
Q
W
Q
<
Q
5000 H
Normal
Glaucoma
2-3
3-4
4-5
5-6
ECCENTRICITY (mm)
3000 -
<
w
N=
6-7
407
NORMAL
D
201
0.4-0.6
155
0.6-0.8
188
0.8-1.0
CUP-DISC RATIO
FIGURE 7. Dendritic field size comparisons for intracellularly labeled parasol cells from normal (open) and glaucomatous (hatched)
eyes. In agreement with their smaller soma sizes, the dendritic fields of neurons from glaucomatous eyes were smaller than normal
(A, B). This difference was most pronounced in the peripheral retina (C). Unlike soma size, the dendritic fields of parasol cells from
glaucomatous eyes were significantly smaller than normal in eyes with moderate (cup-disc, 0.6-0.8) and severe (cup-disc,
0.8-1.0) levels of optic disc cupping (D).
glaucomatous cupping averaged 41.3% smaller in mean crosssectional area (P < 0.001; Fig. 8D).
Axon Thickness of Midget and Parasol Cells in Normal and Glaucomatous Eyes. Proximal axon thickness in all
midget cells ranged from 0.2 /xm to 2.5 /xm, with a mean size
of 1.0 /Ltm ± 0.04 (±SE; TV = 227; Fig. 9A). In agreement with
their larger cell body sizes, parasol cells from normal and
glaucomatous eyes showed the largest axon segments (Fig.
9B). In normal eyes, parasol cell axon diameters ranged from
0.8 jam to 4.2 p,m, with a mean diameter of 1.6 ± 0.03 jwm
(N = 390). In glaucomatous eyes, the initial segments of parasol cell axons tended to be smaller (0.5-3.2 jam), with a mean
diameter of 1.4 ± 0.03 M-m (iV = 509). Only the difference in
the mean axon diameters of parasol cells was significant (P <
0.001). Comparisons of axon diameter in ganglion cells with
different C-D ratios (Figs. 9C, 9D) produced results similar to
those seen in comparisons of soma and dendritic field sizes.
Although the size of axons of parasol cells from eyes with C-D
ratios of 0.4 to 0.6 were not different from normal, the axons
of parasol cells from eyes with C-D ratios of 0.6 to 0.8 were
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
Retinal Ganglion Cell Degeneration in Glaucoma
IOVS, November 1998, Vol. 39, No. 12
2315
20 -i
15 10 -
^1500 n
T
E
j
w
o
o
T
3
<
Q 1000
_J
w
O
H
W
CL,
Q 500
Q
2
u
10
15
20
25
30
35
40
45
50
NORMAL
B
CROSS-SECTIONAL AREA (xlOOum )
3000 i
2000
2500 -
50
GLAUCOMA
n
2 1500 -
Q 2000 -
T
Q
j
J 1500 -
^ 1000 -
2
p
2
Q 1000 -
a
Normal
Glaucoma
500
1
Q
|
500 Z
2
2-3
3-4
4-5
5-6
in
92
NORMAL
0.4-0.6
80
o
6-7
ECCENTRICITY (mm)
N=
D
0.6-0.8
0.8-1.0
CUP-DISC RATIO
FIGURE 8. Comparisons of the dendritic field sizes of midget ganglion cells labeled in normal (open) and glaucomatous (hatched)
eyes (A). Unlike parasol cells, the dendritic fields of midget cells were not significantly different from normal (B, C), except in eyes
with severe (cup-disc, 0.8-1.0) glaucomatous cupping of the optic nerve head (D).
12.5% smaller than normal (P < 0.001), and those from eyes
with C-D ratios more than 0.8 were 43.8% smaller than normal
(P < 0.001). Similar to the pattern seen in dendritic field
measurements, only the axons of midget ganglion cells from
eyes with C-D ratios more than 0.8 were significantly smaller
(40%) than normal (P < 0.001).
DISCUSSION
In this study we used intracellular staining techniques to examine
the degenerative effects that chronic elevation of intraocular pressure, ariskfactor commonly associated with glaucoma, has on the
morphology of single ganglion cells in the primate retina. The
data show that in midget and parasol cells, the earliest structural
signs of glaucomatous neuropathy involved changes at the level of
the dendritic arbor. These changes included a thinning of the
proximal and distal dendrites, abrupt reductions in dendritic process diameter at branch points, and a general decrease in the
complexity of the cell's dendritic tree. Decreases in axon diameter seemed to occur later than changes at the level of the dendritic
arbor, whereas a reduction in soma size occurred concurrently or
slightly later.
Comparisons of ganglion cells from eyes with different
levels of optic nerve damage, based on C-D ratios, suggested
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2316
Weber et al.
IOVS, November 1998, Vol. 39, No. 12
2.0 n
2.0 -i
s
1
3
04
W
\XON DIA
2
Q
1.0 -
§
X
Z
w
p<0.001
~oi 1.5
1.5
2
0.5
1.0
0.5
w
N=
89
N=
0.0
390
509
0.0
NORMAL
NORMAL
GLAUCOMA
GLAUCOMA
B
2.0
2.0 n
n
p<0.001
E 1.5 -
1.5-
pO.001
w
w
S 1.0
1.0 p<0.001
0.5 -
N=
89
89
79
NORMAL
0.4-0.6
0.6-0.8
N=
390
195
154
164
0.0
0.0
NORMAL
0.8-1.0
CUP-DISC RATIO
0.4-0.6
0.6-0.8
CUP-DISC RATIO
0.8-1.0
D
FIGURE 9. Comparisons of the mean differences in intraretinal axon diameter of midget (A, C) and parasol (B, D) cells from normal
(open) and glaucomatous (hatched) eyes. In glaucoma, parasol cells differed from midget cells; on average, their intraretinal axons
were smaller than normal (A, B). This reduction was not restricted to eyes that were severely cupped.
that despite qualitative changes in appearance, the sizes of the
somas, dendritic fields, and axons of midget and parasol cells
typically were not reduced significantly with a C-D ratio of
approximately 0.6 or more. This finding agrees closely with
previous reports that the probability of glaucoma-related abnormalities increases significantly when the C-D ratio equals
or exceeds O.6.39 However, it is important to note that in most
cases, our final C-D ratio assessments were made on eyes with
elevated levels of IOP (47.6 ± 1 5 mm Hg, on average). Because
the optic disc of the young monkey is highly compliant and
therefore can undergo pressure-induced deformations that may
or may not be reversible,42 the possibility exists that we overestimated slightly our C-D ratios, and therefore the level of
optic nerve damage, in the glaucomatous eyes. That the optic
discs of eyes with C-D ratios even in the range of 0.8 to 1.0
showed good color across most of the disc area, with pallor
restricted primarily to the temporal regions, supports this possibility. An overestimation of C-D ratio, however, implies that
the neuronal changes we describe occurred at an even earlier
stage of the disease process.
Identification of Pressure-Induced Degeneration
Because the data presented here were obtained using an in
vitro preparation, it can be argued that many of the morphologic changes ascribed to elevated IOP resulted instead from
severing the axons of ganglion cells during isolation of the
retina. This seems unlikely for several reasons. First, the dendritic abnormalities described in Figures 2 and 4 were uncharacteristic of normal midget and parasol cells examined using
the same experimental conditions. Second, we were unable to
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
Retinal Ganglion Cell Degeneration in Glaucoma
induce comparable structural changes in normal ganglion cells
by altering parameters associated with the in vitro preparation
or with our intracellular staining techniques. Reducing the
flow of oxygenated solution to the tissue, exposing single
neurons to the mercury vapor light for extended periods (> 15
seconds), or staining cells using high levels of negative current
(>5 nA), resulted in neurons whose axons and dendrites contained numerous large, regularly spaced translucent varicosities. These structures were atypical of ganglion cells from
normal and glaucomatous eyes using our standard experimental procedures. Although results of previous Golgi and retrograde labeling studies have suggested that dendritic beading
may be a regular feature of primate ganglion cells,1617 our data
do not support this suggestion and are consistent with data in
other studies in which similar intracellular staining techniques
have been used to examine the morphology of midget and
parasol cells in the primate retina.18"2023'40'41 Thus, although
we cannot rule out the possibility that some neurons were
affected adversely by our experimental approach, we feel confident that the morphologic abnormalities we have described
for ganglion cells in the glaucomatous eye are highly representative of degenerative changes caused by elevated IOP and not
by the in vitro technique per se.
sol, 42.4%) at this stage of the disease as well. That a reduction
in soma size was not prevalent during mild and moderate
stages of the disease is in agreement with Glovinsky et al.,"
who concluded that the differences in cell size distributions
between normal and glaucomatous monkey eyes are not
caused by selective shrinkage of large ganglion cells. Recent
studies in which the rat model of glaucoma has been used,
however, have indicated that the somas and dendriticfieldsof
retinal ganglion cells in the glaucomatous eye may actually
increase in size as a result of the disease process.53 Although
we did not find the somas or dendritic fields of midget or
parasol cells as a whole to be significantly larger than normal in
any of our experimental eyes, it is interesting to note that the
comparisons of soma and dendritic field size versus C-D ratio
(Figs. 5D through 8D) showed small increases in these features
in eyes with mild glaucoma. Whether this represents a shortterm initial response by these neurons to the effects of elevated
IOP or is simply a slight sampling bias remains unclear.
The subtle differences in the degenerative patterns of
midget and parasol cells reported here do not exclude the
possibility of a true differential effect. Although the intracellular method provided detailed information concerning the
soma, axon, and dendritic morphologies of single ganglion
cells, it was limited in the range of retinal area and number of
ganglion cells that could be examined in a single eye. Because
the region of retinal ganglion cell loss in glaucoma can be
highly variable,6'911'54 it is likely that by restricting our injections to the midtemporal retina our cell samples were not
always focused on the most severely affected area of each
retina. Similarly, because the pattern of axon and ganglion cell
loss in glaucoma can be diffuse,3'55'56 not all cells within the
sample region were necessarily affected equally. Indeed, with
the exception of eyes that had uniformly pale, deeply cupped
optic discs, with near complete loss of ganglion cells in midtemporal retina, a wide variety of cell morphology could be
found in each glaucomatous eye. For this reason, it is important
to keep in mind that although the qualitative data presented
here show the range of morphologic features characteristic of
ganglion cells from eyes with different levels of glaucoma, the
quantitative data reflect soma, dendritic field, and axonal differences in the population as a whole.
A third factor that may have affected our ability to detect
a clear differential effect in glaucomatous changes in midget
and parasol cells is an unconscious bias toward the injection of
neurons with larger cell bodies. In all retinas, these neurons
were more visible and easier to inject, particularly in regions
close to the fovea. Because previous studies have suggested
that cell size, and not cell class, may be the determining factor
underlying glaucoma-related retinal ganglion cell degeneration, 5 ' 61011 ' 39 such a bias may have resulted in the undersampling of small cells unaffected by elevated IOP.
Midget Versus Parasol Cells
An issue common to many studies of glaucomatous retinopathy
is whether midget and parasol cells, and therefore the P- and
M-pathways of the primate visual system, are affected differentially by the disease. The significance of this issue derives from
the fact that these pathways are considered to subserve different functional roles, 1314 ' 25 " 29 and thus a preferential effect on
one or the other could have important implications for the
development of more sensitive psychophysical tests to achieve
early detection of the disease. In recent studies in which
changes in axon diameter,5'6 soma size, 1011 and neuronlament
content43 have been examined in ganglion cells from eyes with
glaucoma, results have indicated that although cells of all sizes
are lost, large ganglion cells appear to be affected most severely. That these large neurons may represent primarily parasol cells and the M-pathway is suggested by data indicating an
apparent differential effect on neurons in the magnocellular
and parvocellular layers of the LGN.35'44'45 Functional support
for a preferential effect on the M-pathway also has been provided by psychophysical studies showing a diminution in pattern electroretinogram and pattern visual evoked responses to
stimuli of low spatial and high temporal frequencies46"48 and
a reduction in motion detection49"51 and high-frequency
flicker sensitivity5152in the glaucomatous eye.
Although the axon and dendritic field size measurements
presented here also indicate that chronic elevation of IOP may
have a more detrimental effect on parasol than midget ganglion
cells, the data, in general, suggest that the magnitude of any
differential effect may be small. Midget and parasol cells
showed similar patterns and degrees of degenerative change,
and there was no clear indication in any of the retinas examined that a disproportionate number of cells representing either class were more affected. In addition, the somas of midget
and parasol cells were found to undergo similar reductions in
size (12.5% and 13-3%, respectively), and in both classes of
neurons these reductions were significant only in eyes with
advanced glaucomatous damage. Both classes of cells showed
similar reductions in dendritic field size (midget, 41.3%; para-
2317
Pattern of Retinal Ganglion Cell Degeneration
Our primary goal in carrying out this study was to define more
clearly the degenerative effect that chronic elevation of IOP
has on the morphology of single ganglion cells in the primate
retina. To this end, the data show for the first time that the
earliest signs of retinal ganglion cell degeneration in the glaucomatous eye involved abnormalities in the dendritic field
structures of these neurons. That these changes preceded
anatomic changes at the level of the cell soma indicates that the
onset of retinal ganglion cell degeneration in glaucoma oc-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2318
Weber et al.
curred earlier than previously thought, based on estimates of
ganglion cell loss alone.
Changes in axon diameter also followed those at the level
of the dendritic tree, and these seemed to be closely related to
changes in cell soma size. This pattern of degeneration is not
surprising. Pressure-induced damage to the optic nerve in the
region of the lamina cribrosa has been shown to result in a
reduction or cessation in the normal flow of intracellular materials between the retinal ganglion cells and their target neurons in the LGN.2'57"60 As a first response to this injury, the
retinal ganglion cells begin to pare their distal dendrites to
conserve energy and maintain homeostasis at the level of the
cell soma. With time, many of the damaged axons undergo
retrograde degeneration, further depriving their parent neurons of any residual stores of trophic materials located within
the axon. As these stores are depleted, the dendritic field
becomes progressively more degenerate, and finally the cell
itself begins to shrink. At some as yet undefined point in the
degeneration process, an intracellular signal is activated, and
the injured neuron undergoes apoptosis.6162 The fact that
structural changes at the level of the cell soma are not a
primary feature of the degenerative process suggests a window
of opportunity for possibly mitigating or reversing glaucomatous neuropathy, possibly through the application of different
neuroprotectants or through genetic modification. Investigators have recently identified a wide variety of trophic factors in
the developing vertebrate retina, and many of these factors also
have been shown to be upregulated and neuroprotective after
injury to the retina or the optic nerve.63"73
Although the data presented here indicate that retinal
ganglion cell degeneration in glaucoma is a progressive process, they cannot address two important issues. First, they do
not define the threshold level of insult that results in the
initiation of ganglion cell atrophy. Second, they do not define
the temporal relation between the onset of ganglion cell degeneration and activation of the apoptotic signal. These data
are essential for defining the window of opportunity during
which therapeutic intervention may be most beneficial.
Functional Considerations
Our finding that the earliest signs of retinal ganglion cell degeneration in eyes with chronic elevation of IOP involves
structural changes associated with midget and parasol cells is
consistent with recent psychophysical studies that have described functional deficits related to the M- and P- pathways in
glaucoma. In brief, motion-automated perimetry74 ~78 and highfrequency temporal flicker perimetry51'52—tests designed to
assess the functional integrity of the M-pathway based on the
use of moving targets and gratings of low spatial and high
temporal frequency—have been shown to be sensitive methods for detecting early visual defects in patients with glaucoma.
More recently, Johnson and Samuels79 have shown that frequency-doubled perimetry also provides a quick and efficient
means of screening for glaucomatous visual field loss. The test
is based on the phenomenon that when a sinusoidal grating of
low spatial frequency (e.g., 0.25 cycles/degree) is presented at
a high counterphase rate (>l6 Hz), the grating appears to have
twice the actual spatial frequency. This doubling illusion, first
described by Kelly,80'8' is thought to result from the nonlinear
summation properties characteristic of neurons in the M-, but
not P-, visual pathway.'4
IOVS, November 1998, Vol. 39, No. 12
Of the more recent psychophysical tests intended for
detection of early glaucomatous damage and its relation to
functional defects in the P-pathway, short wavelength automated perimetry has received the most attention. This test uses
large blue targets presented on a bright yellow background to
isolate and measure the responsiveness of short wavelengthsensitive mechanisms. To date, short wavelength automated
perimetry has proved beneficial not only in the detection of
glaucoma-related deficits, but also in the prediction of glaucomatous damage in eyes with ocular hypertension.82"84 Although the blue-sensitive pathway seems to originate from a
population of ganglion cells (small-field bistratified) that are
structurally and functionally distinct from midget and parasol
cells,40'41'85 that the axons of these neurons terminate in the
parvocellular region (although in the interlaminar zones)86 of
the LGN suggests that they are, in general, part of the Ppathway. That the somas and, presumably, axons of these cells
tend to be similar in size to those of surrounding parasol, and
not midget, cells supports the theory that retinal ganglion cell
sensitivity in glaucoma may be based primarily on cell size,
rather than on cell class.5l<5'1011'39 However, it is unlikely that
selective atrophy of these two types of neurons alone represents the earliest degenerative changes in glaucoma, in that
psychophysical studies also have described defects in the redgreen system early in the disease process,87"89 and this information is thought to be carried by midget ganglion cells.90'91
The relation between dendritic field structure and spatial,
temporal, and spectral response abnormalities of midget and
parasol cells is not surprising, considering that the spatial,
temporal, and chromatic properties of these neurons are derived, in large part, by the number, pattern, and type of synaptic inputs they receive on their dendritic arbors. Ongoing
studies are intended to provide better understanding at the
single-cell level of the relation between the dendritic field
integrity of midget and parasol cells and their spatial and
temporal response properties.
Acknowledgments
The authors thank Laurence R. Stanford for his advice and support with
the intracellular methods; Todd Perkins and Michael Bueche for assisting with clinical evaluations of the eyes; Elaine Bostad, Jane Walsh, and
Judy McMillan for technical assistance; and Dan Houser and Shelly
Zimbric of the Wisconsin Regional Primate Research Center (Madison,
WI) for their assistance with the animals.
References
1. Quigley HA. Pathophysiology of the optic nerve in glaucoma. In:
McAllister JA, Wilson RP, eds. Glaucoma. London: Butterworths;
1986:30-53.
2. Quigley HA, Addicks EM. Chronic experimental glaucoma in primates, II: effect of extended intraocular pressure elevation on
optic nerve head and axonal transport. Invest Ophthalmol Vis Sci.
1980;19:137-152.
3. Quigley HA, Addicks EM, Green WR. Optic nerve damage in
human glaucoma, III: quantitative correlation of nerve fiber loss
and visual field defect in glaucoma, ischemic neuropathy, papilledema, and toxic neuropathy. Arch Ophthalmol. 1982; 100:135146.
4. Quigley HA, Addicks EM, Green WR, Maumenee AE. Optic nerve
damage in human glaucoma, II: the site of injury and susceptibility
to damage. Arch Ophthalmol. 1981 ;98:635- 649.
5. Quigley HA, Dunkelberger GR, Green WR. Chronic human glaucoma causing selectively greater loss of large optic nerve fibers.
Ophthalmology. 1988;95:357-363-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
IOVS, November 1998, Vol. 39, No. 12
Retinal Ganglion Cell Degeneration in Glaucoma
6. Quigley HA, Sanchez RM, Dunkelberger GR, L'Hernault NL, Baginski TA. Chronic glaucoma selectively damages large optic nerve
fibers. Invest Ophthalmol Vis Sci. 1987;28:913-920.
7. Radius RL, Pederson JE. Laser-induced primate glaucoma, II: histology. Arch Ophthalmol. 1984;102:l693-l698.
8. Radius RL, Anderson DR. The histology of retinal nerve fiber layer
bundles and bundle defects. Arch Ophthalmol. 1979:97:948-950.
9. Quigley HA, Dunkelberger GR, Green WR. Retinal ganglion cell
atrophy correlated with automated perimetry in human eyes with
glaucoma. AmJ Ophthalmol. 1989; 107:453-464.
10. Glovinsky Y, Quigley HA, Pease ME. Foveal ganglion cell loss is size
dependent in experimental glaucoma. Invest Ophthalmol Vis Sci.
1993:34:395-400.
11. Glovinsky Y, Quigley HA, Dunkelberger GR. Retinal ganglion cell
loss is size dependent in experimental glaucoma. Invest Ophthalmol Vis Sci. 199132:484- 490.
12. Zamber RW, Mills RP, Koontz MA, Phillips JO, Hendrickson AE.
Ganglion cell loss in laser-induced primate glaucoma [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1988;29(4):S421.
13- Dowling, JE. The Retina, An Approachable Part of the Brain.
Cambridge, MA: Belknap Press; 1987:12-123.
14. Kaplan E, Lee BB, Shapley RM. New views of primate retinal
function. In: Osborne N, Chader G, eds. Progress in Retinal
Research. Oxford, UK: Pergamon; 1990:273-336.
15. Rodieck RW, Binmoeller KF, Dineen J. Parasol and midget ganglion
cells of the human retina./ Comp Neurol. 1985;233:115-132.
16. Kolb H, Linberg KA, Fisher SK. Neurons of the human retina: a
Golgi study: / Comp Neurol. 1992;318:147-187.
17. Leventhal AG, Rodieck RW, Dreher B. Retinal ganglion cell classes
in the old world monkey: morphology and central projections.
Science. 1981;213:1139-ll42.
18. Dacey D, Petersen MR. Dendritic field size and morphology of
midget and parasol ganglion cells in the human retina. Proc Natl
AcadSci USA. 1992;89:9666-9670.
19- Dacey D. The mosaic of midget ganglion cells in the human retina.
J Neurosci. 1993;13:5334-5355.
20. Watanabe M, Rodieck RW. Parasol and midget ganglion cells of the
primate retina. / Comp Neurol. 1989;289:434-454.
21. Perry VH, Cowey A. The morphological correlates of X- and Y-like
retinal ganglion cells in the retina of monkeys. Exp Brain Res.
1981;43:226-228.
22. Rodieck RW. The primate retina. In: Stoklis E, ed. Comparative
Primate Biology. Vol. 4. New York: Alan R. Liss; 1988:203-278.
23- Perry VH, Oehler R, Cowey A. Retinal ganglion cells that project to
the dorsal lateral geniculate nucleus in the macaque monkey.
Neuroscience. 1984;12:1101-1123.
24. Rodieck RW, Watanabe M. Survey of the morphology of macaque
retinal ganglion cells that project to the pretectum, superior colliculus, and parvicellular laminae of the lateral geniculate nucleus.
J Comp Neurol. 1993;338:289-303.
25. DeMonasterio FM, Gouras P. Functional properties of ganglion
cells of the rhesus monkey retina./Physiol. 1975;251:l67-195.
26. Kaplan E, Shapley RM. The primate retina contains two types of
ganglion cells, with high and low contrasts sensitivity. Proc Natl
Acacl Sci USA. 1986;83:2755-2757.
27. Merigan WH. Chromatic and achromatic vision of macaques: role
of the P pathway. / Neurosci. 1989;9:776-783.
28. Merigan WH, Katz LM, Maunsell JHR. The effects of parvicellular
lateral geniculate lesions on the acuity and contrast sensitivity of
macaque monkeys./Neurosci. 1991;ll:994-1001.
29- Merigan WH, Maunsell JHR. Macaque vision after magnocellular
lateral geniculate lesions. Vis Neurosci. 1990;5:347-352.
30. Kaufman PL, Davis GE. Minified Goldmann applanating prism for
tonometry in monkeys and humans. Arch Ophthalmol. 1980;98:
542-546.
31. Pederson JE, Gaasterland DE. Laser-induced primate glaucoma, I:
progression of cupping. Arch Ophthalmol. 1984;102:l689-l692.
32. Gaasterland DE, Kupfer C. Experimental glaucoma in the rhesus
monkey. Invest Ophthalmol. 1974;13:455-457.
33- Quigley HA, Hohman RM. Laser energy levels for trabecular meshwork damage in the primate eye. Invest Ophthalmol Vis Sci.
1983;24:1305-1307.
34. Weber AJ, Zelenak D. Experimental glaucoma in the primate eye
induced by injection of latex microspheres into the anterior chamber [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1996;37(3):S815.
35. Weber AJ, Chen H, Kaufman PL, Hubbard WC. Effects of elevated
IOP on cell size, density and number in the primate lateral geniculate nucleus (LGN) [ARVO Abstract]. Invest Ophthalmol Vis Sci.
1997;38(4):S159.
36. Saito AH. Morphology of physiologically identified X-, Y-, and
W-type retinal ganglion cells of the cat./ Comp Neurol. 1983;221:
279-288.
37. Quigley HA, Addicks EM. Regional differences in the structure of
the lamina cribrosa and their relation to glaucomatous optic nerve
damage. Arch Ophthalmol. 1981;99:137-l43.
38. Heijl A. Visual field loss and perimetry in glaucoma. In: Podos SM,
Yanoff M, Kaufman PL, Mittag TW, eds. Textbook of Ophthalmology. Vol. 7. London: Mosby; 1994;7:6-7.27.
39. Quigley HA. Open-angle glaucoma. NEnglJMed. 1993;328:10971106.
40. Dacey DM. Morphology of a small-field bistratified ganglion cell
type in the macaque and human retina. Vis Neurosci. 1993;10:
1081-1098.
41. Ghosh KK, Martin PR, Griinert U. Morphological analysis of the
blue cone pathway in the retina of a New World monkey, the
marmoset Callithrix jacchus. J Comp Neurol. 1997;379:211-225.
42. Burgoyne CF, Quigley HA, Thompson HW, Vitale S, Varma R.
Measurement of optic disc compliance by digitized image analysis
in the normal monkey eye. Ophthalmology. 1995;12:1790-1799.
43. Vickers JC, Schumer RA, Podos SM, Wang RF, Riederer BM, Morrison JH. Differential vulnerability of neurochemically identified
subpopulations of retinal ganglion neurons in monkey model of
glaucoma. Brain Res. 1995;680:23-35.
44. Chaturvedi N, Hedley-Whyte ET, Dreyer EB. Lateral geniculate
nucleus in glaucoma. AmJ Ophthalmol. 1993;ll6:182-188.
45. Chou P, Brandt JD, Tenhula W, Sadun AA. Quantitative measurement of macaque lateral geniculate nucleus (LGN) after chronic
deafferentation and experimental glaucoma [ARVO Abstract]. Invest Ophthalmol Vis Sci. 1992;33(4):S1092.
46. Stamper RL, Tyler CW. Contrast sensitivity testing in glaucoma. In:
Shields MB, Pollack IP, Kokler AE, eds. Perspectives in Glaucoma.
Thorofare, NJ: Slack; 1988:79-93.
47. Marx MS, Podos SM, Bodis-Wollner I, Lee P, Wang R, Severin C.
Signs of early damage in glaucomatous monkey eyes: low spatial
frequency losses in the pattern ERG and VEP. Exp Eye Res. 1988;
46:173-184.
48. Atkin A, Bodis-Wollner I, Podos SM, Wolkstein M, Mylin L,
Nitzberg S. Flicker threshold and pattern VEP latency in ocular
hypertension and glaucoma. Invest Ophthalmol Vis Sci. 1983;24:
1524-1527.
49- Silverman SE, Trick GL, Hart WM Jr. Motion perception is abnormal in primary open-angle glaucoma and ocular hypertension.
Invest Ophthalmol Vis Sci. 1990;31:722-729.
50. Bullimore MA, Wood JM, Swenson K. Motion perception in glaucoma. Invest Ophthalmol Vis Sci. 1993;34:3526-3533.
51. Johnson CA. Early losses of visual function in glaucoma. Optom Vis
Sci. 1995;72:359-370.
52. Casson EJ, Johnson CA. Temporal modulation perimetry in glaucoma and ocular hypertension. In: Mill RP, Heijl A, eds. Perimetry
Update 1992/1993 Amsterdam: Kugler; 1993:443-450.
53- Ahmed F, Chaudhary P, Sharma SC. Effects of increased intraocular
pressure on retinal ganglion cell morphology in albino rat [ARVO
Abstract]. Invest Ophthalmol Vis Sci. 1997;38(4):Sl60.
54. Airaksinen PJ, Tuulonen A, Werner EB. Clinical evaluation of the
optic disc and retinal nerve fiber layer. In: Ritch R, Shields MB,
Krupin T, eds. The Glaucomas. St. Louis: Mosby; 1989:467-494.
55. Airaksinen PJ, Drance SM, Douglas GR. Diffuse and localized nerve
fiber loss in glaucoma. AmJ Ophthalmol. 1984;98:566-571.
56. Radius RL, Pederson JE. Laser-induced primate glaucoma, II: Histology. Arch Ophthalmol. 1984;102:l693-l698.
57. Anderson DR, Hendrickson A. Effect of intraocular pressure on
rapid axonal transport in monkey optic nerve. Invest Ophthalmol.
1974;13:771-783.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017
2319
2320
Weber et al.
58. Quigley HA, Anderson DR. The dynamics and location of axonal
transport blockade by acute intraocular pressure elevation in primate optic nerve. Invest Ophthalmol. 1976;15:606-6l6.
59- Minckler DS, Bunt AH, Johnason GW. Orthograde and retrograde
axoplasmic transport during acute ocular hypertension in the
monkey. Invest Ophthalmol Vis Sci. 1977;l6:426-44l.
60. Dandona L, Hendrickson A, Quigley HA. Selective effects of experimental glaucoma on axonal transport by retinal ganglion cells
to the dorsal lateral geniculate nucleus. Invest Ophthalmol Vis Sci.
1991;32:1593-1599.
61. Quigley HA, Nickells RW, Kerrigan LA, Pease ME, Thibault DJ,
Zack DJ. Retinal ganglion cell death in experimental glaucoma and
after axotomy occurs by apoptosis. Invest Ophthalmol Vis Sci.
1995;36:774-786.
62. Nickells RW. Retinal ganglion cell death in glaucoma: the how, the
why, and the maybe. / Glaucoma. 1996;5:345-356.
63- Johnson JE, Barde Y-A, Schwab M, Thoenen H. Brain derived
neurotrophic factor supports the survival of cultured rat retinal
ganglion cells. / Neurosci. 1986;6:3031-3038.
64. Sievers J, Hausmann B, Unsicker K, Berry M. Fibroblast growth
factors promote the survival of adult retinal ganglion cells after
transection of the optic nerve. Neurosci Lett. 1987;76:157-162.
65. Thanos S, Bahr M, Barde Y-H, Vanselow J. Survival and elongation
of adult rat retinal ganglion cells: in vitro effect of lesioned sciatic
nerve and brain derived neurotrophic factor. Eur J Neurosci.
1989;l:9-26.
66. Park CM, Hollenberg MJ. Basic fibroblast growth factor induces
retinal regeneration in vivo. Dev Biol. 1989;134:201-205.
67. Noji S, Matsuo T, Koyama E, et al. Expression pattern of acidic and
basic fibroblast growth factor genes in adult rat eyes. Biochem
Biophys Res Commun. 1990; 168:343-349.
68. Mey J, Thanos S. Intravitreal injections of neurotrophic factors
support the survival of axotomized retinal ganglion cells in adult
rats in vivo. Brain Res. 1993:602:304-317.
69. Mansour-Robaey S, Clarke DB, Wang Y-C, Bray GM, Aguayo AJ.
Effects of ocular injury and administration of brain-derived neurotrophic factor on survival and regrowth of axotomized retinal
ganglion ells. Proc Natl Acad Sci USA. 1994;91:l632-l636.
70. Kostyk SK, D'Amore PA, Herman IM, Wagner JA. Optic nerve
injury alters basicfibroblastgrowth factor localization in the retina
and optic tract. / Neurosci. 1994; 14:1441-1449.
71. Wen R, Song Y, Cheng T, et al. Injury-induced upregulation of
bFGF and CNTF mRNAS in the rat retina. / Neurosci 1995;15:
7377-7385.
72. Peinado-Ramon P, Salvador M, Villegas-Perez MP, Vidal-Sanz M.
Effects of axotomy and intraocular administration of NT-4, NT-3,
and brain-derived neurotrophic factor on the survival of adult rat
retinal ganglion cells. Invest Ophthalmol Vis Sci. 1996;37:489500.
73. Perez M-TR, Caminos E. Expression of brain-derived neurotrophic
factor and of its function receptor in neonatal and adult rat retina.
Neurosci Lett. 1995;183:96-99.
IOVS, November 1998, Vol. 39, No. 12
74. Bosworth CF, Sample PA, Weinreb RN. Motion perception thresholds in area of glaucomatous visual field loss. Vision Res. 1997;37:
355-364.
75. Bosworth CF, Sample PA, Weinreb RN. Perimetric motion thresholds are elevated in primary open angle glaucoma patients. Vision
Res. 1997;37:1989-1997.
76. Trick GL, Steinman BS, Amyot M. Motion perception deficits in
glaucomatous optic neuropathy. Vision Res. 1995;25:22252233.
77. Silverman SE, Trick GL, Hart WM Jr. Motion perception is abnormal in primary open angle glaucoma. Invest Ophthalmol Vis Sci.
1990;31:722-729.
78. Sample PA, Bosworth CF, Weinreb RN. Short-wavelength automated perimetry and motion automated perimetry in patients with
glaucoma. Arch Ophthalmol. 1997;115:1129-1133.
79- Johnson CA, Samuels SJ. Screening for glaucomatous visual field
loss with frequency-doubling perimetry. Invest Ophthalmol Vis
Sci. 1997;38:4l3-425.
80. Kelly DH. Frequency doubling in visual responses./ Opt Soc Am.
1966;56:1628-1633.
81. Kelly DH. Nonlinear visual responses to flickering sinusoidal gratings. / Opt Soc Am. 1981;71:1O51-1O5582. Sample PA, Taylor JDN, Martinez GA, Lusky M, Weinreb, RN.
Short-wavelength color visual fields in glaucoma suspects at risk.
Am J Ophthalmol. 1993:115:225-233.
83. Johnson CA, Adams AJ, Casson EJ, Brandt JD. Blue-on-yellow perimetry can predict the development of glaucomatous visual field
loss. Arch Ophthalmol. 1993; 111:645- 650.
84. Johnson CA, Adams AJ, Casson EJ, Brandt JD. Progression of early
glaucomatous visual field loss for blue-on-yellow and standard
white-on-white automated perimetry. Arch Ophthalmol. 1993;
111:651-656.
85. Dacey DM, Lee BB. The 'blue-on' opponent pathway in primate
retina originates from a distinct bistratified ganglion cell type.
Nature. 1994;367:731-735.
86. Martin PR, White AJR, Goodchild AK, Wilder HD, Sefton AE.
Evidence that blue-on cells are part of the third geniculocortical
pathway in primates. Eur J Neurosci. 1997;9:1536 -1541.
87. Greenstein VC, Halevy D, Zaidi Q, Koenig KL, Ritch RH. Chromatic
and luminance systems deficits in glaucoma. Vision Res. 1996;36:
621-629.
88. Kelly JP, Fourman SM, Jindra LF. Foveal color and luminance
sensitivity losses in glaucoma. Ophthalmic Surg Lasers. 1996;27:
179-187.
89. Felius J, van den Berg TJ, Spekreijse H. Peripheral cone contrast
sensitivity in glaucoma. Vision Res. 1995;35:1791 -1797.
90. Dacey DM. Circuitry for color coding in the primate retina. Proc
Natl Acad Sci USA. 1996;93:582-588.
91. Kolb H. Anatomical pathways for color vision in the human retina.
Vis Neurosci. 1991;7:6l-74.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933203/ on 05/05/2017