Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
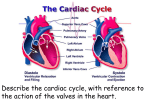
Human Physiology Lecture Notes for Chapter 13 Circulatory System Overview 1. cardiovascular system: blood, heart, blood vessels 2. lymphatic system: lymph, lymph vessels, associated lymphoid tissue (nodes, spleen) Functions cardiovascular system lymphatic system Transport O2 and CO2 nutrients waste hormones and regulatory chemicals immune cells fat from villi immune cells return fluid to blood (vascular system) Protection clotting factors immune cells lymphoid tissue with associated immune cells Regulation cardiovascular system is an important effector for temperature regulation --- Vascular System The vascular system performs its transport function by using series of vessels that are the conduit for blood. (FOX Fig 13.25 gives anatomical differences.) In order for there to be adequate blood flow the body maintains a constant blood pressure (one of the essential parameters). arteries: Thick muscular walls with a elastic layer. During systole (heart contraction) the arteries expand from the pressure. Then when the heart is relaxing (diastole) the arteries “push” due to elastic recoil. Although they don't actually contract the elastic recoil acts as a “pump” and maintains blood pressure (BP). For this reason they are sometimes referred to as a pressure reservoir. Mean arterial pressure (MAP)is 100mmHg arterioles: less elastic, relatively thicker smooth muscle layer, smaller diameter offer resistance to blood flow, greatest area of regulation vasoconstriction/dilation (or precapillary sphincters) controls flow to capillary bed capillaries: single layer of endothelium no cell is further than 3 to 4 cells from a capillary 5% of blood volume is here only 30-50% of the capillary beds are open at one time (not enough blood) different gaps between endothelium cells allows differences in movement venous vessels: veins and venules thin walled, distensible (stretch easily), one way valve average pressure 2 mmHg 64% of blood volume is here: volume reservoir lymph vessels: one way valves pacemaker cells: smooth muscle contracts spontaneously The following support the blood return to the heart: 1. 2. 3. 4. pressure differential one way valves skeletal muscle pumps decrease in thoracic pressure caused by inhalation Heart Anatomy Fox pages 394-406 (8th edition: pgs 378-390) Chambers of the heart: atria (singular = atrium) receive venous blood. ventricles pump blood to either the lungs (pulmonary circulation) or the body (systemic circulation). The blood flow to the body equals the blood flow to the lungs. The left ventricle is more developed because the average back pressure is 100mmHg, while the pulmonary back pressure averages about 15mmHg. The valves between the atria and the ventricles are the AV valves (atrioventricular valves ). The valves leaving the ventricles are semilunar valves (pulmonary semilunar valve and aortic semilunar valve). myocardial cells - short, branched, striated. Connected with gap junctions. The two atria contract as one unit and are referred to as a myocardium. The two ventricle also contract as one unit and are a myocardium. pacemaker cells - spontaneously depolarize and fire A.P. The pacemaker cells in the sinoatrial node (SA node) drive the rest of the heart to depolarize. These are innervated (as mentioned in chapter 9) by parasympathetic and sympathetic neurons. (More on regulation in chapter 14) Spread of depolarization: Conduction through atria is fast (1m/sec), slows through the atrioventricular node (AV node) (0.03 to 0.05m/sec) and then speeds up again through the bundle of His and Purkinje fibers (5m/sec) to ensure even contraction of ventricles. Ventricular contraction is delayed by 0.1 to 0.2 seconds from atrial contraction. Review of action potentials (A.P.) Action potentials in the SA node (pacemaker cells): Calcium slowly “leaks” into the pacemaker cells resulting in spontaneous depolarization to the threshold of voltage gated calcium channels. Opening of voltage gated calcium channels begins the action potential. Repolarization is fostered by opening of potassium channels. SA nodes spontaneously fire A.P. at a rate of 70 to 80 per minute. Other cells in the conducting tissue of the heart also spontaneously depolarize, but at rate slower than the SA node, so they are “driven” to fire A.P. at a rate that is set by the SA node. (They are never given a chance to spontaneously depolarize, except in pathological conditions. When cells other than the SA node are setting the heart beat it is referred to as an ectopic focus.) Action potential in the heart muscle cells Notice long plateau phase. This extends the time of the action potential. Action potentials in cardiac cells last from 200 to 300 msec! This long plateau prevents summation and tetanus. It allows the muscle to relax between beats and ensures that the chambers fill with blood before the next beat. Action potential compared to contraction: The Cardiac Cycle Repeating pattern of contraction and relaxation of the heart. systole - contraction (ventricular) diastole - relaxation (ventricular) Numbers refer to diagram on the next page. 1. Atria and ventricles are relaxed (AV valves are open) Chambers fill with blood (ventricles fill to about 80%) 2. Atria contract and add the last 20% of blood to the ventricles Ventricles 100% full (about 120ml) this is the end diastolic volume. 3. Ventricles begin to contract increase pressure causes AV valves to close (pressure not high enough yet to open the semilunar valves) isometric (or isovolumetric) contraction 4. Pressure increases over arterial pressure (about 80 mmHg in the aorta) semilunar valves open, blood is ejected pressure continues to rise as ventricles contract (to about 120 mmHg for aorta and 25 mmHg in the pulmonary artery) isotonic contraction two thirds of the end diastolic volume is ejected - this is called the stroke volume (about 80ml) 5. Pressure drops below arterial pressure and semilunar valves shut from the back pressure isometric (isovolumetric) relaxation of ventricles this is the beginning of diastole (relaxation of ventricles) 6. When pressure of ventricles is below atria the AV valves open and filling begins again (back to step 1) Electocardiogram (ECG) P wave: atria depolarize (and contract) QRS wave: ventricles depolarize (beginning of systole) ST segment: plateau phase of cardiac action potential T wave: ventricles repolarize (beginning os diastole) First heart sound immediately after this. Second heart sound shortly after T wave begins